

Abstract
This study examined cross-national similarities in a developmental model linking early age of alcohol use onset to frequent drinking and heavy drinking and alcohol problems 1 and 2 years later in a binational sample of 13-year-old students from 2 states: Washington State, United States, and Victoria, Australia (N = 1,833). A range of individual, family, school, and peer influences were included in analyses to investigate their unique and shared contribution to development of early and more serious forms of alcohol use and harms from misuse. Data were collected annually over a 3-year period from ages 13 to 15. Analyses were conducted using multiple-group structural equation modeling. For both states, early use of alcohol predicted frequent drinking, which predicted alcohol problems. Family protective influences had no direct effects on heavy drinking, nor effects on alcohol harm in either state, whereas school protection directly reduced the risk of heavy drinking in both states. Exposure to antisocial peers and siblings predicted a higher likelihood of heavy drinking and alcohol harm for students in both Washington and Victoria. Implications for the prevention of adolescent alcohol problems are discussed.
Keywords: Early onset of alcohol, heavy drinking, alcohol harm, risk and protective influences, zero tolerance, harm reduction
In many developed countries, alcohol is the most commonly used substance among adolescents. Considerable research has been carried out on the etiology and progression of adolescent alcohol use (Donovan, 2004; Fisher, Miles, Austin, Camargo, & Colditz, 2007; Kirisci et al., 2013; Wills et al., 2001), noting that alcohol involvement has biopsychosocial roots and manifests itself in different forms (e.g., initiation, regular use, problematic use) over time.
Early-onset alcohol use (EOA) is associated with an increased likelihood of engaging in frequent and problematic use of alcohol among adolescents (Fergusson, Lynskey, & Horwood, 1994; French & Maclean, 2006; Gruber, DiClemente, Anderson, & Lodico, 1996; Hawkins et al., 1997; Hingson, Heeren, & Winter, 2006; Mason & Spoth, 2012; Swahn, Bossarte, & Sullivent, 2008). Although the defining age of EOA varies across studies (Kuntsche, Rossow, Engels, & Kuntsche, 2016; e.g., before age 13, 14, or 15), there is a general consensus that the younger youth are when they initiate alcohol, the more likely they are to experience alcohol-related harms (e.g., externalizing problems) later in life (Liang & Chikritzhs, 2015; Morean et al., 2014).
Despite a well-established link between EOA and later alcohol harms (Buchmann et al., 2009; DeWit, Adlaf, Offord, & Ogborne, 2000; Hingson et al., 2006), it is not well understood if EOA is itself a direct cause of these harms or whether its effect is indirect through high-frequency drinking. Moreover, few studies have systematically examined predictors that underlie adolescents' progressive use of alcohol (Stice, Barrera, & Chassin, 1998). Comparative studies of family and peer influences are particularly important in that certain factors in these domains may emerge as salient predictors. For example, parents' favorable attitudes toward the use of alcohol may be more strongly related to EOA than to heavy and harmful drinking in the mid-adolescent years (van der Vorst, Engels, Meeus, & Dekovic, 2006). Social risks, such as exposure to siblings or peers who use alcohol, may be less predictive of early-onset use, but more predictive of problematic use among older youth (Mason & Spoth, 2012; Windle, 2000). Additionally, more research is needed to identify protective factors, such as youths' strong attachments to parents (Oxford, Harachi, Catalano, & Abbott, 2001; Patock-Peckham & Morgan-Lopez, 2010), parental involvement and recognition of positive behavior (Nash, McQueen, & Bray, 2005), high academic achievement (Bryant, Schulenberg, O'Malley, Bachman, & Johnston, 2003), and youths' bonds to school (Resnick et al., 1997), that emerge from within family and school contexts, reducing the risk of early-onset, frequent, or problematic use of alcohol.
As suggested by social-developmental theories (Catalano & Hawkins, 1996; Tarter, 2002; Toumbourou & Catalano, 2005), risk and protective factors are developmentally ordered and have both proximal and distal influences on alcohol use behaviors. Individual cognitions and peer-influence risk factors, such as attitudes favorable to alcohol use and peer drinking, are strong proximal predictors of adolescent alcohol use (Fisher et al., 2007). Importantly, some of the strongest protective factors, although more distal to alcohol involvement than attitudinal and peer-related risk factors, emerge from within the family (e.g., parental discipline and family bonding; Nash et al., 2005; Patock-Peckham & Morgan-Lopez, 2010) and school contexts (e.g., academic commitment and achievement; Bryant et al., 2003; Hawkins et al., 1997). Thus, social-developmental theories suggest a progression leading from background factors representing contextual family and school influences to more proximal attitudinal and peer-related risk factors for alcohol involvement, including EOA as well as a more frequent and problematic pattern of use. However, there is a need to fully test this hypothesized progression over time to provide information useful for understanding when and how to intervene.
Although debate exists (Kuntsche et al., 2016), the public health burden of EOA underscores the need to implement intervention programs that delay the onset of drinking (DeWit et al., 2000; Ellickson, Tucker, & Klein, 2003). Prior research has demonstrated that substance misuse preventive interventions can be effective in slowing the rate of alcohol and other substance use initiation in youth (Park et al., 2000; Trudeau, Spoth, Lillehoj, Redmond, & Wickrama, 2003). Yet, little is known about whether the same risk and protective factors associated with EOA and later problem drinking found in the United States are applicable to other countries that might have different alcohol-related cultures or policies. This knowledge is essential for understanding the degree to which evidenced-based prevention programs that address these risk and protective factors to prevent EOA and alcohol use might have comparable effects in the United States and other countries.
The current study seeks to examine the progression of adolescent alcohol use from EOA to heavy drinking and alcohol harm through frequent alcohol use. To address the question of whether the same risk and protective factors are associated with different dimensions of alcohol use, we include a range of individual and social influence variables, both proximal and distal, that have been documented as correlates and predictors of adolescent substance use (Beyers, Toumbourou, Catalano, Arthur, & Hawkins, 2004; Hawkins, Catalano, & Miller, 1992; Hemphill et al., 2011; Mason et al., 2011). Based on social-developmental theory and existing research (Bahr, Marcos, & Maughan, 1995; Nash et al., 2005; Oxford et al., 2001), we hypothesized that family and school protection indirectly influence early and more serious alcohol use by influencing youths' choice of friends, and attitudes toward alcohol use and antisocial behavior.
Given that the data for this study are part of a large international investigation that focuses on risks and behaviors of youth in Washington (WA) State, United States, and Victoria (VIC), Australia, the present study also seeks to contribute to extending knowledge regarding the generalizability of direct and indirect effects of EOA on adolescent heavy and harmful drinking through frequent use, and associated risk and protective factors across two states. Findings from this study could contribute to knowledge of cross-national applicability of prevention programs that address the same risk and protective factors to reduce the overall rates of alcohol use and problems for youth in WA, United States and VIC, Australia, which have different alcohol-related norms and policies to guide the prevention and control of alcohol use.
Methods
Study Procedures and Sample
Data were collected through the International Youth Development Study (IYDS), a binational study of youth development in WA, United States, and VIC, Australia. The study uses the Communities That Care (CTC) Youth Survey, an instrument with good reliability and validity for multiple demographic groups in the United States (Glaser, Van Horn, Arthur, Hawkins, & Catalano, 2005). Items of the CTC survey were cognitively pretested and pilot tested in both states prior to being finalized. The larger study used matched sampling, recruitment, and survey administration procedures to ensure the comparability of the data collected (see McMorris et al., 2007 for details on the study design).
Data for the current analyses are from the Grade 7 cohort of the IYDS, which includes 961 students in WA (78.4% of those eligible) and 984 students in VIC (75.6% of those eligible) who participated in three annual survey administrations from 2002 to 2004. Surveys were group administered each year in classrooms from February to June in WA and from May to October in VIC to maintain seasonal equivalence. Retention rates for 2 consecutive follow-up years were 98% in both states. Consistent with prior analyses (McMorris, Catalano, Kim, Toumbourou, & Hemphill, 2011), tests of selective attrition indicated that attrited versus retained students were somewhat more likely to be from Victoria, to be slightly older, and to be from slightly lower income levels (results available on request). Study protocols were approved and are in compliance with the University of Washington Human Subjects Review Committee and the Royal Children's Hospital Ethics in Human Research Committee in Melbourne, Australia.
The analysis sample consists of 1,833 students, excluding 112 students classified as dishonest (reported use of a fictional drug or had improbably excessive illicit drug use—cumulative use >120 times in past 30 days) or who had not responded to the “honesty” questions across all three data collection periods. This sample is composed primarily of 13-year-olds in the 1st year of the study (WA M = 13.1, SD = 0.4; VIC M = 13.0, SD = 0.4), and is roughly gender balanced (49% male and 51% female overall and in each state sample). In WA, 65% of students described themselves as White, 16% as Latino(a), 6% as Asian/Pacific Islander, 6% as Native American, 4% as African American, and 3% reported belonging to other ethnic groups. In VIC, the majority of students described themselves as Australian (91%), 6% as Asian/Pacific Islander, 1% as Aboriginal or Torres Strait Islander, less than 1% each as African or Spanish, and 1% reported belonging to other ethnic groups. Because Australians have a tendency to identify as Australians if they were not foreign born regardless of race, racial/ethnic categories are not directly comparable across the states; thus, the present analyses do not control for race/ethnicity.
Measures
Alcohol involvement variables
EOA was measured at age 13 by asking students how old they were when they first had more than just a sip or two of an alcoholic beverage. Response options were coded based on a 5-point scale (from 0 “never had by age 13” to 4 “age 10 or under” so that earlier initiation is a higher score). Frequent alcohol use was assessed at age 14 by asking students on how many occasions they had more than just a sip or two of an alcoholic beverage in the past 30 days. Heavy drinking was measured at age 15 by asking students how many times they had five or more alcoholic drinks in a row in the past 2 weeks. Although these measures of frequent alcohol use and heavy drinking originally used an 8-point response option from 0 “never” to 7 “40 or more times,” responses were recoded to reduce skewness. The recoded items were scored on a 4-point scale, ranging from 0 “never” to 3 “6 or more times.” Alcohol harm, measured at age 15, focused on eight harmful consequences of drinking, scored on a frequency scale of “never” to “40 or more times” over the past year (Hibbert, Caust, Patton, Rosier, & Bowes, 1996). Consequences included loss of control (e.g., “not able to stop drinking once you had started”) and social conflict (e.g., “become violent and get into a fight”). Because few responses exceeded a frequency of three or more times, responses were dichotomized to indicate 1 “ever experienced a particular alcohol-related harm in the past year” versus 0 “never.” Items were summed to produce a count of the number of harmful alcohol consequences experienced in the past year, ranging from 0 to 6 or more consequences.
Individual and social influences and other covariates
Measures of the 15 individual and social influences assessed at age 13 are summarized in Table 1. For all measures, higher scores indicate more of the individual and social influences, as labeled. Except for information on the household, which is based on parent reports, variables in the model are based on youth reports.
Table 1. Construct Information, Rotated Factor Loadings, and Standardized Factor Loadings.
| Constructs | Description/Example | Number of items | Reliability alphaa | Standardized loadings | ||
|---|---|---|---|---|---|---|
|
|
||||||
| WA | VIC | WA | VIC | |||
| Control variables | ||||||
| Gender | Male = 0, female = 1 | 1 | - | - | - | - |
| SES | Parent report of their income and education | 2 | .50 | .36 | - | - |
| Family protection | ||||||
| Low family conflict | We argue about the same things in my family over and over. | 3 | .81 | .81 | .65 | .55 |
| Attachment to parents | Do you feel very close to your mother? | 6 | .76 | .79 | .76 | .77 |
| Prosocial family opportunities | If I had a personal problem, I could ask my mom or dad for help. | 3 | .74 | .75 | .79 | .83 |
| Prosocial family rewards | My parents notice when I am doing a good job and let me know about it. | 2 | .72 | .75 | .81 | .84 |
| School protection | ||||||
| Academic achievement | What were your grades like last year? | 2 | .55 | .48 | .51 | .52 |
| Commitment to school | How often did you try to do your best work in school? | 2 | .32 | .39 | .64 | .75 |
| Prosocial school opportunities | I have lots of chances to be part of class discussions of activities. | 5 | .49 | .58 | .48 | .53 |
| Prosocial school rewards | The school lets my parents know when I have done something well. | 4 | .65 | .72 | .55 | .57 |
| Favorable attitudes toward problem behavior | ||||||
| Parental favorable attitudes toward alcohol/drugs | How wrong do your parents feel it would be for you to drink beer or wine regularly? | 4 | .85 | .72 | .53 | .64 |
| Parental favorable attitudes toward antisocial behavior | How wrong do your parents feel it would be for you to pick a fight with someone? | 3 | .71 | .72 | .56 | .59 |
| Student favorable attitudes toward alcohol/drugs | How wrong do you think it is for someone your age to drink beer or wine regularly? | 2 | .87 | .78 | .79 | .77 |
| Student favorable attitudes toward antisocial behavior | How wrong do you think it is for someone your age to pick a fight with someone? | 5 | .82 | .83 | .83 | .83 |
| Exposure to sibling and peer problem behavior | ||||||
| Siblings' alcohol/drug use problems | Have any of your brothers or sisters ever drunk alcohol? | 5 | .85 | .82 | .68 | .62 |
| Attachment to problem peers | In the past year, how many of your best friends have been suspended from school? | 8 | .81 | .66 | .68 | .70 |
| Peers' alcohol use | In the past year, how many of your best friends have tried alcohol? | 1 | - | - | .73 | .63 |
WA = Washington State; VIC = Victoria
Alpha coefficients were estimated for the scales based on three or more than three items, while correlation coefficients were provided for the scales using two items.
Analysis Strategy
There were three steps in the analyses. First, we examined differences in the prevalence and mean levels of alcohol use for students in WA and VIC. Mean differences were compared using t-tests, and effect sizes were calculated with pooled standard deviations (Cohen, 1988). Second, we used exploratory factor analysis (EFA) to identify a set of latent factors that combine the individual and social risk and protective variables. The GEOMIN oblique rotation was used to handle variables loaded on more than one latent factor (Browne, 2001), and the maximum likelihood method was used for factor extraction (Fabrigar, Wegener, MacCallum, & Strahan, 1999). Parallel analysis was performed to determine the optimum number of factors to retain from randomly generated correlation matrixes (Hayton, Allen, & Scarpello, 2004), which provides more accurate numbers of components to retain than does Kaiser's (1960) eigenvalue greater than 1 rule (Zwick & Velicer, 1986). In the third step, multiple-group confirmatory factor analysis (MGCFA) and multiple-group structural equation modeling (MGSEM) were conducted to examine correlations among the variables and to test hypothesized structural paths.
The EFA, MGCFA, and MGSEM analyses were conducted using Mplus version 7.11 (L. K. Muthén & Muthén, 1998-2010). In order to accommodate the modeling of ordered categorical dependent variables (e.g., EOA, frequent alcohol use), we used the weighed least squares mean-and variance-adjusted (WLSMV) estimator. As a robustness check, the primary analyses were re-run treating the dependent variables as continuous under maximum likelihood robust (MLR) estimation. In that the substantive findings were highly similar across the two approaches, we present only results for the WLSMV approach below. Model fit was assessed using the mean-and variance-adjusted chi-square statistic (B. O. Muthén, du Toit, & Spisic, 1997), Root Mean Square Error of Approximation index (RMSEA; Browne & Cudeck, 1993), and the Comparative Fit Index (CFI; Browne & Cudeck, 1993). WLSMV estimation in Mplus implements a pairwise missing data strategy known to perform well when the data are missing at random after taking exogenous covariates into account. Because the WLSMV estimator was used, differences in the fit of nested models were estimated based on mean- and variance-adjusted chi-square statistics and degrees of freedom using the Mplus Difftest command (Satorra, 2000). Tests of mediation hypotheses are based on an estimation of indirect effects generated with the Mplus Model Indirect command (L. K. Muthén & Muthén, 1998-2010).
Results
Differences in Prevalence and Levels of Alcohol Involvement
Table 2 provides differences in prevalence and means, as well as Cohen's effect sizes (d; Cohen, 1988) for alcohol involvement variables for youth in both state samples. For all types of alcohol use, students in VIC showed higher prevalence and mean levels relative to those in WA.
Table 2. Differences in Prevalence Rates and Means in Alcohol Involvement Variables Between Washington State and Victoria.
| Washington | Victoria | |||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| Prevalence | Prevalence | |||||
| Variables | Range | (%)* | Mean (SD) | (%)* | Mean (SD) | Effect size d |
| Early onset of alcohol use | 0∼4 | 43.7 | 1.23 (1.57) | 65.9 | 1.86 (1.58) | .40 |
| Frequent alcohol use | 0∼3 | 21.5 | 0.30 (0.66) | 43.6 | 0.68 (0.92) | .47 |
| Heavy drinking | 0∼3 | 15.4 | 0.28 (0.74) | 29.9 | 0.53 (0.92) | .30 |
| Alcohol harm | 0∼6 | 20.8 | 0.53 (1.24) | 35.9 | 0.98 (1.66) | .31 |
Note: All of the mean differences between states were significant using t-tests at p < .001: mean and pooled standard deviations were used to calculate effect size, d specified by Cohen (1988) that d of.20 indicates small, of .50 indicates medium, and of .80 indicates large effect size.
Prevalence rates were computed based on the proportion of youth involved in the indicated alcohol problems; for early onset of alcohol use, prevalence was estimated based on the number of youth who had initiated alcohol by age 13.
Exploratory Factor Analysis
The EFA produced four latent factors with an eigenvalue of 1.16 from the sample data and 1.08 from the parallel analysis (the five-factor model eigenvalues were 0.84 for the sample data and 1.05 for the parallel analysis). Table 3 shows the results of the EFA for the four-factor solution, including rotated factor loadings of the measured variables. The latent factors are labeled to correspond to the items grouped in each factor: family protection, school protection, favorable attitudes toward problem behavior, and exposure to sibling and peer problem behavior. These four latent factors are used for subsequent analyses to test the model in Figure 1.
Table 3. Oblique GEOMIN-rotated Factor Loadings From Exploratory Factor Analysis.
| Family protective factor | School protective factor | Favorable attitudes toward problem behavior | Exposure to sibling and peer problem behavior | |
|---|---|---|---|---|
| Family protection | ||||
| Low family conflict | .43 | -.02 | .01 | -.24 |
| Attachment to parents | .90 | -.04 | .03 | .00 |
| Prosocial family opportunities | .73 | .11 | -.01 | -.03 |
| Prosocial family rewards | .79 | .08 | -.04 | .02 |
| School protection | ||||
| Academic achievement | .06 | .33 | .09 | -.22 |
| Commitment to school | .02 | .49 | -.09 | -.17 |
| Prosocial school opportunities | -.01 | .69 | -.01 | .02 |
| Prosocial school rewards | .03 | .70 | -.01 | .02 |
| Favorable attitudes toward problem behavior | ||||
| Parental favorable attitudes toward alcohol/drugs | .01 | .06 | .75 | -.01 |
| Parental favorable attitudes toward antisocial behavior | -.04 | -.01 | .67 | -.02 |
| Student favorable attitudes toward alcohol/drugs | .02 | -.03 | .55 | .28 |
| Student favorable attitudes toward antisocial behavior | -.04 | -.12 | .50 | .27 |
| Exposure to sibling and peer problem behavior | ||||
| Siblings' alcohol/drug use problems | -.20 | .10 | .06 | .46 |
| Attachment to problem peers | -.01 | -.07 | -.05 | .69 |
| Peers' alcohol use | .04 | .02 | .11 | .66 |
Note: Results were based on both Washington State and Victorian students. Separate tests for each state yielded the same four components, with patterns of loadings consistent with those reported here.
Figure 1.
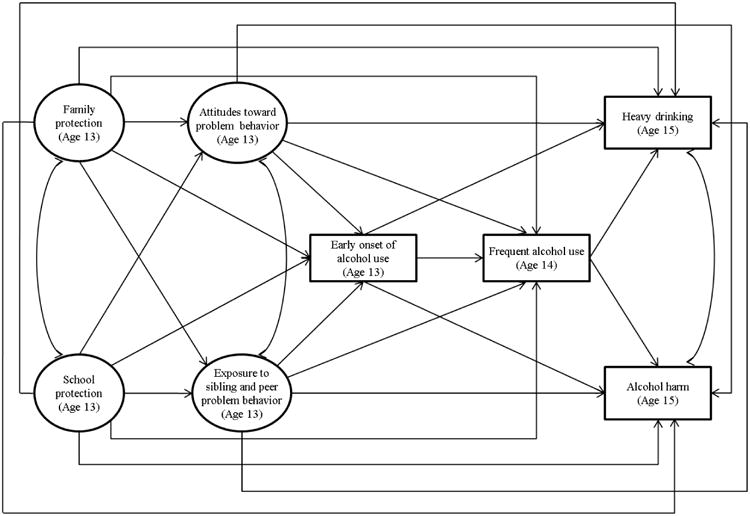
Hypothesized model.
Multiple-group Structural Equation Modeling
Multiple-group confirmatory factor analysis
To evaluate the equivalence of the measures, an MGCFA was conducted. The unconstrained model in which factor loadings of the two state samples were allowed to be free (χ2 (284) = 1109.39, p < .05, CFI = .92, RMSEA = .06) showed that all factor loadings are significant and of a similar magnitude (Table 1). A subsequent MGCFA in which loadings were constrained equal for the two samples also fit the data adequately (χ2 (295) = 896.23, p < .05, CFI = .94, RMSEA = .05). In addition, there was a nonsignificant difference in fit between the constrained and unconstrained CFA models after using a Bonferroni correction to adjust for the multiple constraints tested (0.05/11 = .005), Δχ2 (Δdf) = 25.32 (11), p < .01, Bonferroni adjusted p = 0.08. Thus, we constrained all of the factor loadings across two states in subsequent MGSEM analyses. Standardized correlation coefficients among the variables from the constrained MGCFA are presented in Table 4.
Table 4. Standardized Correlation Coefficients for Washington State and Victoria From the Confirmatory Factor Analysis.
| Female | SES | Early onset | Favorable attitudes | Exposure to problem behavior | Family protection | School protection | Frequent alcohol use | Heavy drinking | |
|---|---|---|---|---|---|---|---|---|---|
| SES | -.01ns (.00ns) | - | |||||||
| Early onset of alcohol use | .03ns (-.16) | -.10 (-.14) | - | ||||||
| Favorable attitudes toward problem behavior | -.07ns (-.09) | -.10 (-.04ns) | .39 (.41) | - | |||||
| Exposure to sibling and peer problem behavior | .06ns (-.13) | -.21 (-.15) | .48 (.40) | .65 (.60) | - | ||||
| Family protection | -.07ns (.03ns) | .14 (.10) | -.37 (-.27) | -.49 (-.50) | -.51 (-.39) | - | |||
| School protection | .20 (.20) | .18 (.19) | -.34 (-.39) | -.50 (-.53) | -.41 (-.46) | .64 (.71) | - | ||
| Frequent alcohol use | .07 (-.03 ns) | -.10 ns (-.11) | .40 (.42) | .37 (.39) | .44 (.36) | -.23 (-.19) | -.21 (-.26) | - | |
| Heavy drinking | .05ns (.06ns) | -.22 (-.20) | .38 (.38) | .36 (.40) | .48 (.41) | -.29 (-.26) | -.30 (-.37) | .46 (.58) | - |
| Alcohol harm | .09 (.03ns) | -.10 (-.14) | .42 (.34) | .43 (.42) | .52 (.43) | -.39 (-.28) | -.36 (-.35) | .55 (.55) | .76 (.75) |
nonsignificant (i.e., p ≥ .05).
Note: Coefficients were from the constrained confirmatory factor analysis model in which equality constraints were imposed on all of the factor loadings across the states of Washington and Victoria; coefficients for Victoria are in parentheses; unless otherwise noted, correlations are significant at p < .05 or better.
Multiple-group structural model
To test the cross-state equivalence in structural paths shown in Figure l (gender and SES were included as controls, although not presented in Figure 1), we first estimated an unconstrained MGSEM in which all structural paths were freely estimated. That model fit the data adequately (χ2 (295) = 896.23, p < .05, CFI = .94, RMSEA = .05).
A second test of the model constrained all structural paths to equality. Although the fully constrained model fit the data well (χ2 (322) = 914.58, p < .05, CFI = .94, RMSEA = .05), the chi-square difference test indicated a significant group difference (Δχ2 (Δdf) = 65.96 (27), p < .001, Bonferroni adjusted p = 0.001). To understand which path contributed to the significant state difference, we used modification indices from the fully constrained model. The cross-equality constraints producing the largest modification index values were on the paths from family protection to exposure to sibling and peer problem behavior, and from frequent alcohol use to heavy drinking; thus, we compared the unconstrained model with a partially constrained model in which the cross-state constraints on those two paths were released from the fully constrained model. This comparison yielded a nonsignificant chi-square statistic (Δχ2 (Δdf) = 32.55 (25), p > .05), resulting in the final model in which all of the paths were fixed to equality except for the two freely estimated paths mentioned above (χ2 (320) = 882.85, p < .05, CFI = .95, RMSEA = .04).
Figure 2 shows only statistically significant unstandardized coefficients from the partially constrained model. Standardized coefficients, estimated using group-specific standard deviations of the variables, are also presented in parentheses to assist in understanding the magnitude of an estimated effect within a group. Coefficients for gender and SES are separately presented in Table 5. Findings indicated that the hypothesized relationships are more similar than different for the two states, with two exceptions: the magnitude of the state difference in the association between family protection and the exposure variable was larger for WA relative to VIC, whereas the association between frequent alcohol use and heavy drinking was larger for VIC relative to WA. Together, these paths partially mediated the relationship between EOA and heavy drinking and fully mediated the association between EOA and alcohol harm. Direct effects of EOA on alcohol harm are not statistically significant. Additionally, the standardized indirect effects of EOA on heavy drinking (WA = .07, VIC = .12) and alcohol harm (WA = .10, VIC = .10) through frequent use are significant in both states (p < .05).
Figure 2.
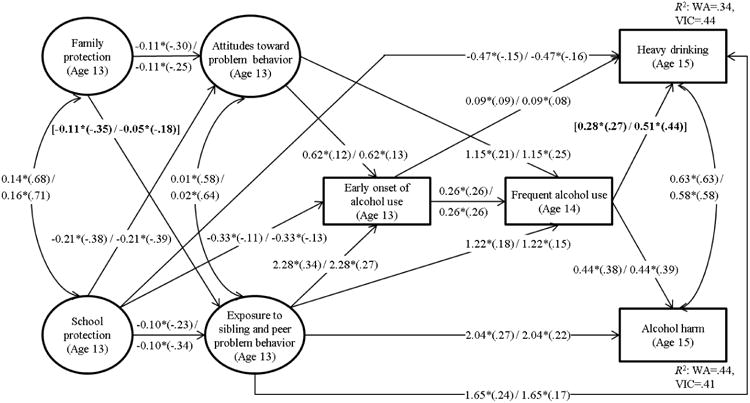
Statistically significant path coefficients from the final structural equation model for Washington State and Victoria students. WA = Washington State; VIC = Victoria.
Note: Unstandardized coefficients are presented with standardized coefficients in parentheses, first for Washington and then for Victoria; path coefficients that were freely estimated across two states are in brackets; analysis sample size for Washington State is 923, and 910 for Victoria; family and school protection, attitudes toward problem behavior, and exposure to risky environment; heavy drinking and alcohol harm variables were freely correlated; all variables were regressed on gender and SES, and results for control variables are presented in Table 5.
*p < .05 or better
Table 5. Unstandardized and Standardized Path Coefficients on Gender and SES for Washington State and Victoria From the Final Structural Equation Model.
| Washington | Victoria | |||
|---|---|---|---|---|
|
|
||||
| Paths | Unstandardized coefficients (SE) | Standardized coefficients | Unstandardized coefficients (SE) | Standardized coefficients |
| Gender (0 = male, 1 = female)→ | ||||
| Family protection | -0.08* (.04) | -.07* | 0.03 (.04) | .03 |
| School protection | 0.18* (.04) | .22* | 0.18* (.04) | .19* |
| Favorable attitudes toward problem behavior | -0.00 (.02) | -.01 | -0.01 (.02) | -.01 |
| Exposure to sibling and peer problem behavior | 0.03* (.01) | .09* | -0.02* (.01) | -.07* |
| Early onset of alcohol use | 0.09 (.10) | .04 | -0.19* (.08) | -.08* |
| Frequent alcohol use | 0.26* (.12) | .11* | 0.11 (.09) | .05 |
| Heavy drinking | 0.17 (.13) | .07 | 0.38* (.11) | .14* |
| Alcohol harm | 0.10 (.12) | .04 | 0.29* (.10) | .11* |
| SES→ | ||||
| Family protection | 0.10* (.03) | .15* | 0.06* (.02) | .10* |
| School protection | 0.09* (.02) | .19* | 0.11* (.02) | .19* |
| Favorable attitudes toward problem behavior | 0.01 (.01) | .02 | 0.01 (.01) | .04 |
| Exposure to sibling and peer problem behavior | -0.02* (.01) | -.12* | -0.02* (.01) | -.09* |
| Early onset of alcohol use | 0.01 (.05) | .00 | -0.08 (.05) | -.06 |
| Frequent alcohol use | -0.03 (.07) | -.02 | -0.06 (.06) | -.04 |
| Heavy drinking | -0.16* (.08) | -.11* | -0.14* (.06) | -.08* |
| Alcohol harm | 0.03 (.07) | .02 | -0.03 (.06) | -.02 |
Note: other significant path coefficients from the final structural equation model are shown in Figure 2, while nonsignificant path coefficients are available upon request.
p < .05 or better
Results show that protection by the family is only indirectly related to alcohol use variables shown in the model. School protection had direct effects on EOA and heavy drinking, after accounting for other variables. In neither state did favorable attitudes toward problem behavior at age 13 predict heavy drinking or alcohol harm directly. The effects of the attitudes variable only indirectly increase the risk of heavy drinking and alcohol harm through EOA and frequent alcohol use (range in standardized indirect paths: .07 ∼.12, p < .05). For both states, exposure to sibling and peer problem behavior predicted heavy drinking and alcohol harm directly and indirectly by increasing risk of EOA and frequent alcohol use.
Discussion
This study analyzed binational data to examine the developmental progression of adolescent alcohol use and associated risk and protective factors in WA, United States, and VIC, Australia. For both state samples, EOA by age 13 increased risk of heavy drinking and alcohol harm at age 15 through frequent alcohol use at age 14. EOA also had a small but statistically significant direct effect on heavy drinking for students in both states. This study also found that attitudes toward problem behavior and exposure to sibling and peer problems had positive influences on EOA as well as frequent drinking. The exposure variable further predicted heavy drinking and alcohol harm over and above EOA and frequent alcohol use among students in both WA and VIC. Family protection showed more distal impacts on alcohol involvement for students in the two states, having direct negative associations with attitudes toward problem behavior and exposure to sibling and peer problem behavior. In addition, school protection had direct negative associations with EOA and heavy drinking for students in both states. Results of the MGSEM suggest these patterns are largely similar in the two state samples, consistent with previous findings from the larger IYDS study (Mason et al., 2011; McMorris et al., 2011).
Consistent with earlier published research addressing a robust association between EOA and later heavy drinking (DeWit et al., 2000; Liang & Chikritzhs, 2015), this study found a persistent direct effect on heavy drinking when controlling for risk and protective factors. This suggests that early alcohol onset directly increases risk for later heavy drinking, perhaps because early-onset drinkers have more time to escalate their alcohol consumption and transition into heavier patterns of use than late-onset drinkers. The effect of frequent alcohol use on heavy drinking was 2 times greater in VIC. However, we found no direct impact of EOA on alcohol harm, which includes alcohol-related externalizing problem behavior (e.g., fighting) as well as loss of control (e.g., not able to stop drinking). This suggests that those negative consequences of drinking may be more vulnerable to alcohol-favorable attitudes and behavior within family, peer, and school compared to heavy alcohol consumption per se, resulting in no direct association between EOA and later alcohol harm when these environmental influences are held constant.
Consistent with previous research, this study found that contextual family protective factors predict alcohol involvement only indirectly through individual attitudinal and peer exposure variables (Bahr et al., 1995; Nash et al., 2005). Family protection had a stronger negative association with exposure to problem behavior for students in WA compared to those in VIC. For both WA and VIC students, positive influences and experiences within the school context further had direct negative predictive associations with early onset of alcohol and heavy drinking, but not later, more harmful drinking patterns. In contrast, parents' and students' favorable attitudes toward problem behavior and sibling and peer substance use predicted not only EOA but also alcohol frequency, and in the case of sibling and peer substance use, heavy drinking and alcohol harm as well. These findings illustrate both common (exposure to substance use models) and unique (e.g., school protection, attitudes toward problem behavior) predictors of the different dimensions of alcohol involvement (e.g., Mason & Spoth, 2012), which has implications for understanding what intervention targets to address for specific outcomes.
Several study limitations are worth noting. First, although we treated risk and protective variables as predictors of EOA, these variables were measured contemporaneously, leaving the possibility of bidirectional effects. Second, this study relies predominantly on youth self-reports. Although, most studies have found these reports to be valid (Johnston, O'Malley, Bachman, & Schulenberg, 2007), it is possible the results are influenced somewhat from relying on data from a single source. Third, heavy drinking was measured in the past 2-week time frame, which may underestimate the prevalence of infrequent heavy drinking. However, a recent study found that the measure of past 2-week heavy drinking had about 78% concordance with heavy drinking in the past year (Cranford, McCabe, & Boyd, 2006). Fourth, generalizability of study results is limited to youth (ages 13 - 15) of the two states.
The current investigation extends previous findings (Hemphill et al., 2011; Mason et al., 2011; McMorris et al., 2011) by indicating that the direction and magnitude of associations between alcohol involvement variables in the pathways from EOA to heavy and harmful drinking and the risk and protective factor variables related to different dimensions of alcohol use were largely the same for youth in the United States (WA) and Australia (VIC). Differences were found between the two states in the magnitude but not the statistical significance of paths between EOA and frequent alcohol use and between family protection and problem behavior exposure. Thus, despite country context differences, students with higher protection from the family and school appear less likely to initiate drinking at an early age. Also, students in both countries who are exposed to peers and siblings who use alcohol are at higher risk themselves for drinking earlier and more frequently, and for eventually experiencing alcohol-related problems. Therefore, the same prevention programs targeting these protective and risk factors are likely to reduce problems from alcohol whether they are implemented in the United States or in Australia. As noted elsewhere (see Hawkins et al., 1997; Spoth, Trudeau, Guyll, Shin, & Redmond, 2009), delaying the age of alcohol use onset may help lower the risk of alcohol problems for most adolescents, particularly in Australia where the impact of EOA on frequency of use is higher.
Acknowledgments
Funding. Data collection for the International Youth Development Study was supported by the National Institute on Drug Abuse (R01-DA012140) and the analysis and writing of this article was funded by the National Institute on Alcohol Abuse and Alcoholism (R01-AA017188). The content of this paper is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
Footnotes
Compliance with Ethical Standards: Conflict of Interest. All authors declare that they have no conflict of interest.
Ethical Approval. Study protocols were approved by the Royal Children's Hospital Ethics in Human Research Committee and the University of Washington Human Subjects Review Committee. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent. Informed consent was obtained from all study participants.
References
- Bahr SJ, Marcos AC, Maughan SL. Family, educational and peer influences on the alcohol use of female and male adolescents. Journal of Studies on Alcohol. 1995;56:457–469. doi: 10.15288/jsa.1995.56.457. [DOI] [PubMed] [Google Scholar]
- Beyers JM, Toumbourou JW, Catalano RF, Arthur MW, Hawkins JD. A cross-national comparison of risk and protective factors for adolescent substance use: The United States and Australia. Journal of Adolescent Health. 2004;35:3–16. doi: 10.1016/j.jadohealth.2003.08.015. [DOI] [PubMed] [Google Scholar]
- Browne MW. An overview of analytic rotation in exploratory factor analysis. Multivariate Behavioral Research. 2001;36:111–150. [Google Scholar]
- Browne MW, Cudeck R. Alternative ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing structural equation models. Newbury Park, CA: Sage; 1993. pp. 136–162. [Google Scholar]
- Bryant AL, Schulenberg JE, O'Malley PM, Bachman JG, Johnston LD. How academic achievement, attitudes, and behaviors relate to the course of substance use during adolescence: A 6-year, multiwave national longitudinal study. Journal of Research on Adolescence. 2003;13:361–397. [Google Scholar]
- Buchmann AF, Schmid B, Blomeyer D, Becker K, Treutlein J, Zimmermann US, et al. Laucht M. Impact of age at first drink on vulnerability to alcohol-related problems: Testing the marker hypothesis in a prospective study of young adults. Journal of Psychiatric Research. 2009;43:1205–1212. doi: 10.1016/j.jpsychires.2009.02.006. [DOI] [PubMed] [Google Scholar]
- Catalano RF, Hawkins JD. The social development model: A theory of antisocial behavior. In: Hawkins JD, editor. Delinquency and crime: Current theories. New York: Cambridge University Press; 1996. pp. 149–197. [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd. Hillsdale, NJ: Lawrence Erlbaum; 1988. [Google Scholar]
- Cranford JA, McCabe SE, Boyd CJ. A new measure of binge drinking: Prevalence and correlates in a probability sample of undergraduates. Alcoholism: Clinical and Experimental Research. 2006;30:1896–1905. doi: 10.1111/j.1530-0277.2006.00234.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeWit DJ, Adlaf EM, Offord DR, Ogborne AC. Age at first alcohol use: A risk factor for the development of alcohol disorders. American Journal of Psychiatry. 2000;157:745–750. doi: 10.1176/appi.ajp.157.5.745. [DOI] [PubMed] [Google Scholar]
- Donovan JE. Adolescent alcohol initiation: A review of psychosocial risk factors. Journal of Adolescent Health. 2004;35:529, e527–518. doi: 10.1016/j.jadohealth.2004.02.003. [DOI] [PubMed] [Google Scholar]
- Ellickson PL, Tucker JS, Klein DJ. Ten-year prospective study of public health problems associated with early drinking. Pediatrics. 2003;111:949–955. doi: 10.1542/peds.111.5.949. [DOI] [PubMed] [Google Scholar]
- Fabrigar LR, Wegener DT, MacCallum RC, Strahan EJ. Evaluating the use of exploratory factor analysis in psychological research. Psychological Methods. 1999;4:272–299. [Google Scholar]
- Fergusson DM, Lynskey MT, Horwood LJ. Childhood exposure to alcohol and adolescent drinking patterns. Addiction. 1994;89:1007–1016. doi: 10.1111/j.1360-0443.1994.tb03360.x. [DOI] [PubMed] [Google Scholar]
- Fisher LB, Miles IW, Austin B, Camargo CA, Colditz GA. Predictors of initiation of alcohol use among US adolescents - Findings from a prospective cohort study. Archives of Pediatrics & Adolescent Medicine. 2007;161:959–966. doi: 10.1001/archpedi.161.10.959. [DOI] [PubMed] [Google Scholar]
- French MT, Maclean JC. Underage alcohol use, delinquency, and criminal activity. Health Economics. 2006;15:1261–1281. doi: 10.1002/hec.1126. [DOI] [PubMed] [Google Scholar]
- Glaser RR, Van Horn ML, Arthur MW, Hawkins JD, Catalano RF. Measurement properties of the Communities That Care® Youth Survey across demographic groups. Journal of Quantitative Criminology. 2005;21:73–102. [Google Scholar]
- Gruber E, DiClemente RJ, Anderson MM, Lodico M. Early drinking onset and its association with alcohol use and problem behavior in late adolescence. Preventive Medicine: An International Journal Devoted to Practice and Theory. 1996;25:293–300. doi: 10.1006/pmed.1996.0059. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychological Bulletin. 1992;112:64–105. doi: 10.1037/0033-2909.112.1.64. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Graham JW, Maguin E, Abbott RD, Hill KG, Catalano RF. Exploring the effects of age of alcohol use initiation and psychosocial risk factors on subsequent alcohol misuse. Journal of Studies on Alcohol. 1997;58:280–290. doi: 10.15288/jsa.1997.58.280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayton JC, Allen DG, Scarpello V. Factor retention decisions in exploratory factor analysis: A tutorial on parallel analysis. Organizational Research Methods. 2004;7:191–205. [Google Scholar]
- Hemphill SA, Heerde JA, Herrenkohl TI, Patton GC, Toumbourou JW, Catalano RF. Risk and protective factors for adolescent substance use in Washington State, United States and Victoria, Australia: A longitudinal study. Journal of Adolescent Health. 2011;49:312–320. doi: 10.1016/j.jadohealth.2010.12.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hibbert M, Caust J, Patton GC, Rosier M, Bowes G. The health of young people in Victoria: Adolescent Health Survey. Melbourne, Australia: Centre for Adolescent Health Monograph; 1996. [Google Scholar]
- Hingson RW, Heeren T, Winter MR. Age at drinking onset and alcohol dependence: Age at onset, duration, and severity. Archives of Pediatrics and Adolescent Medicine. 2006;160:739–746. doi: 10.1001/archpedi.160.7.739. [DOI] [PubMed] [Google Scholar]
- Johnston LD, O'Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national survey results on drug use, 1975-2006 Volume I: Secondary school students. Bethesda, MD: National Institute on Drug Abuse; 2007. Publication No.07-6205. [Google Scholar]
- Kaiser HF. The application of electronic computers to factor analysis. Educational and Psychological Measurement. 1960;20:141–151. [Google Scholar]
- Kirisci L, Tarter R, Ridenour T, Zhai ZW, Fishbein D, Reynolds M, Vanyukov M. Age of alcohol and cannabis use onset mediates the association of transmissible risk in childhood and development of alcohol and cannabis disorders: Evidence for common liability. Experimental and Clinical Psychopharmacology. 2013;21:38–45. doi: 10.1037/a0030742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuntsche E, Rossow I, Engels R, Kuntsche S. Is ‘age at first drink’ a useful concept in alcohol research and prevention? We doubt that. Addiction. 2016;111:957–965. doi: 10.1111/add.12980. [DOI] [PubMed] [Google Scholar]
- Liang W, Chikritzhs T. Age at first use of alcohol predicts the risk of heavy alcohol use in early adulthood: A longitudinal study in the United States. International Journal of Drug Policy. 2015;26:131–134. doi: 10.1016/j.drugpo.2014.07.001. [DOI] [PubMed] [Google Scholar]
- Mason WA, Spoth R. Sequence of alcohol involvement from early onset to young adult alcohol abuse: Differential prediction and moderation by family-focused preventive intervention. Addiction. 2012;107:2137–2148. doi: 10.1111/j.1360-0443.2012.03987.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mason WA, Toumbourou JW, Herrenkohl TI, Hemphill SA, Catalano RF, Patton GC. Early-age alcohol use and later alcohol problems in adolescents: Individual and peer mediators in a bi-national study. Psychology of Addictive Behaviors. 2011;25:625–633. doi: 10.1037/a0023320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McMorris BJ, Catalano RF, Kim MJ, Toumbourou JW, Hemphill SA. Influence of family factors and supervised alcohol use on adolescent alcohol use and harms: Similarities between youth in different alcohol policy contexts. Journal of Studies on Alcohol and Drugs. 2011;72:418–428. doi: 10.15288/jsad.2011.72.418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McMorris BJ, Hemphill SA, Toumbourou JW, Catalano RF, Patton GC. Prevalence of substance use and delinquent behavior in adolescents from Victoria, Australia and Washington State, United States. Health Education and Behavior. 2007;34:634–650. doi: 10.1177/1090198106286272. [DOI] [PubMed] [Google Scholar]
- Morean ME, Kong G, Camenga DR, Cavallo DA, Connell C, Krishnan-Sarin S. First drink to first drunk: Age of onset and delay to intoxication are associated with adolescent alcohol use and binge drinking. Alcoholism: Clinical and Experimental Research. 2014;38:2615–2621. doi: 10.1111/acer.12526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén BO, du Toit SHC, Spisic D. Robust inference using weighted least squares and quadratic estimating equations in latent variable modeling with categorical and continuous outcomes. 1997 Retrieved July 14 2010 from http://www.gseis.ucla.edu/faculty/muthen/articles/Article_075.pdf.
- Muthén LK, Muthén BO. Mplus user's guide. 6th ed. Los Angeles, CA: Muthén & Muthén; 1998-2010. [Google Scholar]
- Nash SG, McQueen A, Bray JH. Pathways to adolescent alcohol use: Family environment, peer influence, and parental expectations. Journal of Adolescent Health. 2005;37:19–28. doi: 10.1016/j.jadohealth.2004.06.004. [DOI] [PubMed] [Google Scholar]
- Oxford ML, Harachi TW, Catalano RF, Abbott RD. Preadolescent predictors of substance initiation: A test of both the direct and mediated effect of family social control factors on deviant peer associations and substance initiation. American Journal of Drug and Alcohol Abuse. 2001;27:599–616. doi: 10.1081/ada-100107658. [DOI] [PubMed] [Google Scholar]
- Park J, Kosterman R, Hawkins JD, Haggerty KP, Duncan TE, Duncan SC, Spoth R. Effects of the “Preparing for the Drug Free Years” curriculum on growth in alcohol use and risk for alcohol use in early adolescence. Prevention Science. 2000;1:125–138. doi: 10.1023/a:1010021205638. [DOI] [PubMed] [Google Scholar]
- Patock-Peckham JA, Morgan-Lopez AA. Direct and mediational links between parental bonds and neglect, antisocial personality, reasons for drinking, alcohol use, and alcohol problems. Journal of Studies on Alcohol and Drugs. 2010;71:95–104. doi: 10.15288/jsad.2010.71.95. [DOI] [PubMed] [Google Scholar]
- Resnick MD, Bearman PS, Blum RW, Bauman KE, Harris KM, Jones J, et al. Udry JR. Protecting adolescents from harm: Findings from the National Longitudinal Study on Adolescent Health. Journal of the American Medical Association. 1997;278:823–832. doi: 10.1001/jama.278.10.823. [DOI] [PubMed] [Google Scholar]
- Satorra A. Scaled and adjusted restricted tests in multi-sample analysis of moment structures. In: Heijmans RDH, Pollock DSG, Satorra A, editors. Innovations in multivariate statistical analysis A Festschrift for Heinz Neudecker. London: Kluwer Academic; 2000. pp. 233–247. [Google Scholar]
- Spoth R, Trudeau L, Guyll M, Shin C, Redmond C. Universal intervention effects on substance use among young adults mediated by delayed adolescent substance initiation. Journal of Consulting and Clinical Psychology. 2009;77:620–632. doi: 10.1037/a0016029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stice E, Barrera M, Chassin L. Prospective differential prediction of adolescent alcohol use and problem use: Examining the mechanisms of effect. Journal of Abnormal Psychology. 1998;107:616–628. doi: 10.1037//0021-843x.107.4.616. [DOI] [PubMed] [Google Scholar]
- Swahn MH, Bossarte RM, Sullivent EE., III Age of alcohol use initiation, suicidal behavior, and peer and dating violence victimization and perpetration among high-risk, seventh-grade adolescents. Pediatrics. 2008;121:297–305. doi: 10.1542/peds.2006-2348. [DOI] [PubMed] [Google Scholar]
- Tarter RE. Etiology of adolescent substance abuse: A developmental perspective. American Journal on Addictions. 2002;11:171–191. doi: 10.1080/10550490290087965. [DOI] [PubMed] [Google Scholar]
- Toumbourou JW, Catalano RF. Predicting developmentally harmful substance use. In: Stockwell T, Gruenewald PJ, Toumbourou JW, Loxley W, editors. Preventing harmful substance use: The evidence base for policy and practice. London: Wiley; 2005. pp. 53–65. [Google Scholar]
- Trudeau L, Spoth R, Lillehoj C, Redmond C, Wickrama K. Effects of a preventive intervention on adolescent substance use initiation, expectancies, and refusal intentions. Prevention Science. 2003;4:109–122. doi: 10.1023/a:1022926332514. [DOI] [PubMed] [Google Scholar]
- van der Vorst H, Engels R, Meeus W, Dekovic M. The impact of alcohol-specific rules, parental norms about early drinking and parental alcohol use on adolescents' drinking behavior. Journal of Child Psychology and Psychiatry. 2006;47:1299–1306. doi: 10.1111/j.1469-7610.2006.01680.x. [DOI] [PubMed] [Google Scholar]
- Wills TA, Cleary S, Filer M, Shinar O, Mariani J, Spera K. Temperament related to early-onset substance use: Test of a developmental model. Prevention Science. 2001;2:145–163. doi: 10.1023/a:1011558807062. [DOI] [PubMed] [Google Scholar]
- Windle M. Parental, sibling, and peer influences on adolescent substance use and alcohol problems. Applied Developmental Science. 2000;4:98–110. [Google Scholar]
- Zwick WR, Velicer WF. Comparison of five rules for determining the number of components to retain. Psychological Bulletin. 1986;99:432–442. [Google Scholar]