

Abstract
SPONASTRIME (SPOndylar and NAsal changes, with STRIations of the MEtaphyses) dysplasia is a rare, autosomal recessive bone disorder first described by Fanconi et al. [1983: Helv Paediatr Acta 38:267–280]. Radiographic findings include abnormal vertebral bodies with age-dependent changes, and striations of the metaphyses, scoliosis, and retarded ossification of the carpal bones. Physical features include severe short stature, lumbar lordosis, midface hypoplasia, frontal bossing, and a depressed nasal root. To date, 12 patients from 6 families have been reported. Four additional patients have been reported with a variant of this condition, which includes mental retardation. We report on an 11-year-old boy with features consistent with SPONASTRIME dysplasia. Height was 106.1 cm (−6 SD). He had a coarse appearing face with a depressed nasal bridge, short, upturned nose, and midface hypoplasia. Intelligence was normal. A clinical evaluation at 6 years of age suggested the diagnosis of spondylo-epiphyseal dysplasia (SED). However, genetics evaluation at 11 years of age with repeat radiologic studies revealed delayed carpal ossification (−4 to −5 SD), metaphyseal irregularities and striations most notably in the distal femurs and the proximal tibias, lumbar lordosis, narrow interpedicular distances of the lumbar spine, and pear-shaped vertebral bodies. These findings were most consistent with the diagnosis of SPONASTRIME dysplasia, and not SED. Although radiographic findings of SPONASTRIME dysplasia are distinguishable from SED, the physical appearance may be similar. Many bone dysplasias have overlapping radiographic findings and clinical presentation but with different recurrence risks, making genetic counseling a challenge.
Keywords: SPONASTRIME dysplasia, bone dysplasia, short stature, genetic counseling
INTRODUCTION
SPONATSRIME (SPOndylar and NAsal changes, with STRIations of the MEtaphyses) dysplasia is a rare bone dysplasia first characterized by Fanconi et al. [1983] in four sisters with similar radiograph findings and clinical appearance. Currently, 12 patients from 6 families have been described [Fanconi et al., 1983; Lachman et al., 1989; Langer et al., 1996; Masuno et al., 1996]. Both male and female siblings have been reported suggesting an autosomal recessive inheritance pattern. Four additional patients have been reported with a variant of this condition, which includes mental retardation [Camera et al., 1993; Nishimura et al., 1998; Verloes et al., 1995]. Langer et al. [1997] reported diagnostic criteria for this condition, the most important being the appearance of the vertebral bodies. The lumbar vertebral bodies are always abnormal with age-dependent changes. Metaphyseal striations and irregular metaphyseal margins are reported features of this condition. Other skeletal abnormalities include a progressive decrease in the interpediculate distance from lumbar vertebrae 1–5, delayed carpal bone ossification, flattened maxilla and nasal bridge, and mild scoliosis. Physical features include marked short stature, large appearing head, lumbar lordosis, and a consistent facial appearance with flattened mid-face and nasal bridge with a short, upturned nose. Because the phenotypic appearance resembles that of other bone dysplasias, radiographic evidence is necessary to confirm the diagnosis. Herein, we report an 11-year-old boy with the physical and radiographic presentation of SPONASTRIME dysplasia.
CLINICAL REPORT
Our patient was born at 39 weeks to a G3P1 female. Repeated prenatal ultrasound studies revealed a small size. The pregnancy was otherwise unremarkable. Delivery was vaginal with no complications. Birth weight was 2.45 kg (−2 SD) and length was 43.5 cm (−4 SD). At the time of our evaluation at 11 years of age, height was 106.1 cm (−6 SD), weight was 19.7 kg (−4 SD), and OFC was 49.5 cm (−3 SD). His mother is of average height and weight and has an OFC of 54.8 cm (50th centile). The father was not available for evaluation. The family history was negative for other members with short stature. He is an only child, and the parents denied consanguinity. The past medical history was not significant except for chronic otitis media. Growth hormone evaluations were normal. Calcium, phosphorus, and alkaline phosphatase levels were within normal range. His tonsils and adenoids were removed at 11 years of age. Tympanostomy tubes were placed due to fluid build-up during the same year. There have been no vision problems. Development had been normal, and he has completed the fourth grade. The physical exam revealed a short boy of Caucasian/Mexican descent (Fig. 1a and b). He had a coarse facial appearance with midface hypoplasia, flattened nasal bridge, short, upturned nose, and thick full lips. Review of photographs at 1 year of age showed a short, upturned nose and midface hypoplasia (Fig. 1c). Height was 61.6 cm (−5 SD) and weight was 6.9 kg (−3 SD).
Fig. 1.

Facial (a) and full body view (b) of our patient at 11 years of age. Facial view at 1 year of age showing midface hypoplasia and a short, upturned nose (c).
An evaluation for an underlying etiology for his short stature syndrome was conducted at 6 years of age. At that time the diagnosis of a form of spondyloepiphyseal dysplasia (SED) was considered. On review, the radiographs showed mild dolichocephaly with maxillary hypoplasia (Fig. 2). There were biconcave deformities of the posterior one third of the thoracic and lumbar vertebral bodies. A progressive decrease in the interpediculate distances of the lumbar vertebrae from L1 to L5 was noted. There were mild striations at the ends of the long bones, especially at the knees. Epiphyseal ossification centers of the long bones were small for age and the epiphyseal ossification of the right hip had an irregular contour, suggestive of Meyer’s dysplasia. A film of the hand showed delayed skeletal maturation, 3 SD below the mean. Only two carpal bones were ossified.
Fig. 2.
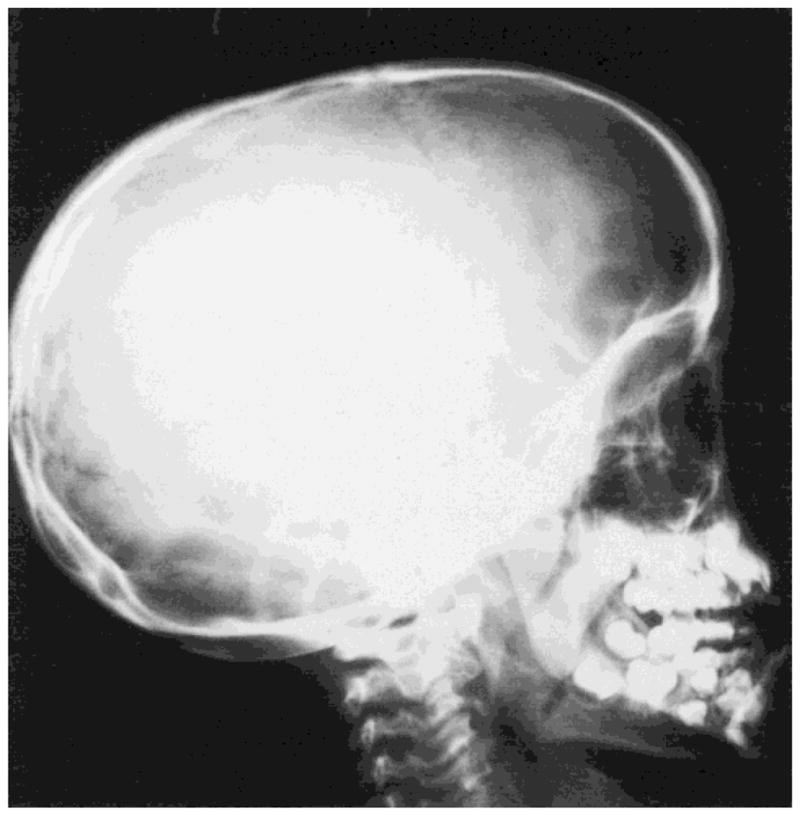
Lateral skull film taken at 67/12 years of age shows mild dolichocephaly with flattening of the midface due to maxillary hypoplasia.
A repeat skeletal survey at 11 years of age showed the same findings as described earlier with interval progression of the changes in the vertebral bodies and in the metaphyseal striations. Skeletal maturation was delayed by 4–5 SD (Figs. 3–5). Epiphyseal ossification centers remained small for age, especially those of the proximal humeri and proximal femurs. The irregularity of the proximal right femoral epiphyseal ossification center had resolved. These findings, in conjunction with the clinical findings, led us to the conclusion that the diagnosis was more consistent with SPONASTRIME dysplasia and not SED (Figs. 3–5).
Fig. 3.

Hand radiographs taken at 11 years of age showing delayed carpal ossification (4–5 SD below the mean).
Fig. 5.
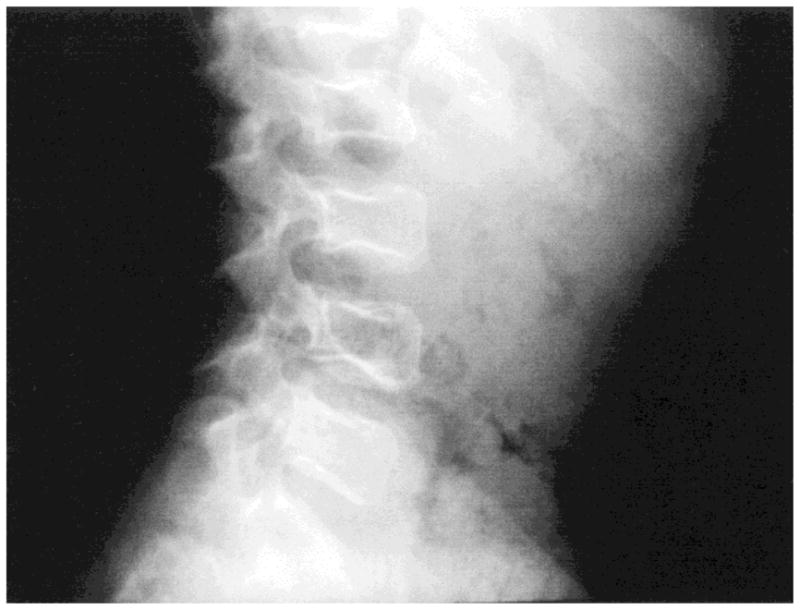
Lateral lumbar spine at 11 years of age. Biconcave deformities of the posterior aspect of the vertebral bodies are noted.
DISCUSSION
At 6 years of age, our patient was thought to have a nonspecific form of SED based on physical characteristics and radiographic evidence. At that time, the metaphyseal striations were present but not pronounced. These striations have become more apparent at an older age, thus indicating the diagnosis of SPONASTRIME dysplasia. Langer et al. [1997] noted that some patients with this condition do not have striations of the metaphyses. Striations may be a variable feature of this condition that appears to increase with time. Early diagnosis of this condition may be hindered by the lack of metaphyseal striations. Vertebral body abnormalities may be a more consistent diagnostic feature of this condition.
Severe short stature, characteristic facial appearance, and radiographic findings are the diagnostic hallmarks that distinguish this bone dysplasia from others with similar outward appearance. The X-linked form of SED is a bone dysplasia with a 50% recurrence risk for male children. SPONASTRIME dysplasia is an autosomal recessive condition. Therefore, with the diagnosis of SPONASTRIME dysplasia, more accurate reproductive risks could be shared with the family. The chance for our patient to have a similarly affected child would be less than 1% due to a presumed low carrier frequency in the general population. The chance for his parents to have another affected child would be 25%.
A summary of the clinical findings in our patient and the reported cases of SPONASTRIME dysplasia are seen in Table I. Of the 13 subjects including our patient, ages ranged from 5 months to 18 years with an average age of 9 years 6 months. Eight females and 5 males have been reported to date. Short stature and delayed bone age are cardinal features and reported in 100% of subjects. Short stature was notable throughout the life span. Average height was 4.5 SD below the mean. Generally, children with SPONASTRIME dysplasia have relatively large head sizes in relation to their body. Our patient’s head was less than the 3rd centile based on the standard growth chart but was large compared to his length parameters. Maternal head size is at the 50th centile, and therefore not presumed to be a contributing factor for his microcephaly. All other reported cases showed a notable difference in relative size of their heads as compared to their height. Clinically, he had the facial appearance of this condition with the typical low nasal root and midface hypoplasia as seen in 100% of reported subjects. A prominent forehead was also noted as seen in 91% of reported subjects.
TABLE I.
Clinical Findings in Reported Cases of SPONASTRIME Dysplasia
| Patients |
Fanconi et al., 1983
|
Lachman et al., 1989
|
Langer et al., 1996
|
Masuno et al., 1996 | Our patient 10 7/12 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | 1 | 2 | 3 | |||||
| Age (years) | 18 | 15 | 13 | 2 | 11 7/12 | 8 11/12 | 6 9/12 | 5/12 | 7 7/12 | 5 9/12 | 17 7/12 | 6 | |
| Sex | F | F | F | F | M | F | F | F | M | M | M | F | M |
| Physical | |||||||||||||
| Height (cm) | 145.1 | 141.4 | 139.9 | ? | 112.5 | 108 | 102 | 53.5 | 100.7 | 85.6 | 154 | 94.2 | 106.1 |
| Height (SD) | −3.4 | −4.1 | −4.6 | −3.9 | −6 | −5 | −3 | −4 | −4.5 | −6 | −4 | −4.4 | −6 |
| OFC (SD) | +0.4 | +1.2 | −0.5 | +2.7 | −1 | −0.5 | ? | ? | ? | ? | ? | 0.0 | −2 |
| Prominent forehead | + | + | − | + | + | + | ? | ? | + | + | + | + | + |
| Saddle nose | + | + | + | + | + | + | + | + | ? | ? | + | + | + |
| Midface hypoplasia | + | + | + | + | + | + | + | + | + | + | + | ? | + |
| Radiographic | |||||||||||||
| Mild osteoporosis | + | + | + | + | + | + | ? | ? | ? | ? | ? | ? | + |
| Delayed bone age | + | + | + | + | + | + | + | ? | ? | ? | ? | + | + |
| Thickened skull | + | + | − | + | + | + | ? | ? | ? | ? | ? | ? | − |
| Abnormal vertebral bodies | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Pear-shaped | − | − | − | + | ? | ? | + | + | ? | ? | ? | + | + |
| Thickened endplates | + | + | + | + | ? | ? | ? | ? | ? | ? | ? | ? | − |
| Endplate indentation | + | + | + | − | + | + | ? | + | + | + | ? | ? | + |
| L1–L5 narrowing | + | + | + | + | + | + | ? | ? | ? | ? | + | ? | + |
| Thorocolumbar scoliosis | − | + | + | − | − | + | ? | ? | ? | ? | ? | + | + |
| Lumbar lordosis | + | + | + | − | ? | ? | + | + | ? | ? | ? | + | + |
| Striations of metaphyses | + | + | + | + | + | + | + | + | + | ? | ? | + | + |
| Brachymetacarpy | + | + | + | + | ? | ? | ? | ? | ? | ? | ? | ? | + |
A metacarpophalangeal pattern profile (MCPP) analysis was also performed on this subject by measuring the individual 19 hand bones in millimeters with a vernier caliper from a hand radiograph obtained at 6 years 7 months of age and then comparing them to bone-length standards (appropriate for age and sex) published by Garn et al. [1972] (White Americans, age 2 years to adulthood) and Poznanski et al. [1972] (Gefferth Hungarian sample, birth to 15 months). Through these comparisons, Z score values for the 19 bones were obtained (Z score = observed bone length − mean bone length/SD) [Butler et al., 1986; Butler et al., 1988; Butler et al., 1993]. The MCPP for our patient in Fig. 6 shows up and down deviation of the phalanges but a relatively flat pattern for the metacarpals. The hand pattern showed small hand bones with negative Z scores calculated for all 19 bones. The Z scores ranged between −0.1 (middle phalanx 5) to −2.8 (metacarpal 2). All metacarpals were outside of the normal range (+2 to −2 Z scores), supporting brachymetacarpy as a common feature of this condition. Of patients who have been evaluated, 100% have shown brachymetacarpy.
Fig. 6.

Metacarpophalangeal pattern profile demonstrating small hand bones (all bones were short with each Z score < 0) with the metacarpals having the smallest Z scores (brachymetacarpy). Up and down deviation of the phalanges were noted with a relatively flat pattern for the metacarpals.
A pattern variability index [ΣZ2/N − (Z/N)2] for quantitation of hand changes as described by Garn et al. [1987] was also calculated from the MCPP data; a score of 0.73 was obtained. A score greater than 0.7 is considered abnormal, indicating hand dysmorphogenesis. In comparison with reported MCPP data from other SPONASTRIME dysplasia subjects [Fanconi et al., 1983], we found a similar hand pattern with up and down deviation for the phalanges, indicating overlap in the development of the hand bones in this dysplasia. Therefore, the MCPP observations suggest the potential of this analysis for providing a useful tool in assisting in the diagnosis of SPONASTRIME dysplasia.
Fig. 4.

a: Radiograph of long bones taken at 6 years of age showing mild striations of the distal femurs and proximal tibias. b: Radiographs taken at 11 years of age showing increased striations of the long bones.
Acknowledgments
We thank Mr. Kerry Kirk for his expert technical assistance in development of the photographs and figures.
References
- Butler MG, Meaney FJ, Kaler SG. Metacarpophalangeal pattern profile analysis in clinical genetics: an applied anthropometric method. Am J Phys Anthropol. 1986;70:195–201. doi: 10.1002/ajpa.1330700206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butler MG, Dijkstra PF, Meaney FJ, Gale DD. Metacarpophalangeal pattern profile analysis in Sotos syndrome: a follow-up report on 34 subjects. Am J Med Genet. 1988;29:143–147. doi: 10.1002/ajmg.1320290118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butler MG, Dahir GA, Gale DD, Meaney FJ. Metacarpophalangeal pattern profile analysis in Brachman-de Lange syndrome. Am J Med Genet. 1993;47:1003–1005. doi: 10.1002/ajmg.1320470713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Camera G, Camera A, Di Rocco M, Gatti R. Sponastrime dysplasia: report on two siblings with mental retardation. Pediatric Radiol. 1993;23:611–614. doi: 10.1007/BF02014981. [DOI] [PubMed] [Google Scholar]
- Fanconi S, Issler Chr, Giedion A, Prader A. The SPONASTRIME dysplasia: familial short-limb dwarfism with saddle nose, spinal alterations, and metaphyseal striation. Helv Paediatr Acta. 1983;38:267–280. [PubMed] [Google Scholar]
- Garn SM, Hertzog KP, Poznanski AK, Nagy JM. Metacarpophalangeal length in the evaluation of skeletal malformation. Radiology. 1972;105:375–381. doi: 10.1148/105.2.375. [DOI] [PubMed] [Google Scholar]
- Garn SM, Leonard WR, Poznanski AK. Applications of the pattern variability index (OZ) to the quantification of dysmorphogenesis in the hand. Am J Med Genet. 1987;27:143–152. doi: 10.1002/ajmg.1320270115. [DOI] [PubMed] [Google Scholar]
- Lachman RS, Stoss H, Spranger J. Sponastrime dysplasia: a radiologic–pathologic correlation. Pediatric Radiol. 1989;19:417–424. doi: 10.1007/BF02387640. [DOI] [PubMed] [Google Scholar]
- Langer LO, Jr, Beals RK, LaFranchi S, Scott CI, Jr, Sockalosky JJ. Sponastrime dysplasia: five new cases and review of nine previously published cases. Am J Med Genet. 1996;63:20–27. doi: 10.1002/(SICI)1096-8628(19960503)63:1<20::AID-AJMG7>3.0.CO;2-W. [DOI] [PubMed] [Google Scholar]
- Langer LO, Jr, Beals RK, Scott CI., Jr Sponastrime dysplasia: diagnostic criteria based on five new and six previously published cases. Pediatric Radiol. 1997;27:409–414. doi: 10.1007/s002470050157. [DOI] [PubMed] [Google Scholar]
- Masuno M, Nishimura G, Adachi M, Hotsubo T, Tachibana K, Makita Y, Imaizumi K, Kuroki Y. Sponastrime dysplasia: report on a female patient with severe skeletal changes. Am J Med Genet. 1996;66:429–432. doi: 10.1002/(SICI)1096-8628(19961230)66:4<429::AID-AJMG8>3.0.CO;2-F. [DOI] [PubMed] [Google Scholar]
- Nishimura G, Mikawa M, Fukushima Y. Another observation of Langer-type Sponastrime dysplasia variant. Am J Med Genet. 1998;80:288–290. [PubMed] [Google Scholar]
- Poznanski AK, Garn SM, Nagy JM, Gall JC. Metacarpophalangeal pattern profiles in the evaluation of skeletal malformations. Radiology. 1972;104:1–11. doi: 10.1148/104.1.1. [DOI] [PubMed] [Google Scholar]
- Verloes A, Mission JP, Dubru JM, Jamblin P, Le Merrer M. Heterogeneity of SPONASTRIME dysplasia: delineation of a variant form with severe mental retardation. Clin Dysmorphol. 1995;4:208–215. [PubMed] [Google Scholar]