

Abstract
Background:
Despite abundant sunshine, Vitamin D deficiency is prevalent in urban India. However, reports on analyzing Vitamin D status from rural Indian population are scanty. Here, we have evaluated Vitamin D status in patients attending outpatient department (OPD) in a rural Indian hospital setting.
Methods:
A hospital-based cross-sectional study was conducted at a secondary level rural hospital in patients attending medicine OPD. After obtaining informed consent, demographic information was collected from consecutive adult patients along with 3 ml blood sample for Vitamin D analysis using electro chemiluminescene on cobas elecys E411 fully automated system. Vitamin D levels were compared across various groups by using Mann–Whitney or Kruskal–Wallis tests, and multiple linear regression analysis was performed to identify the predictors of Vitamin D level.
Results:
A total of 640 patients were enrolled in the study, and the prevalence of Vitamin D deficiency (<20 ng/ml) was found to be 65.4% with 95% confidence interval of 61.7–69.1%. On univariate analysis, Vitamin D levels were statistically significantly lower among younger age group, those who have dark complexion, wearing Burkha (veil), and those who were not adequately exposed to sunlight. After multiple linear regressions, dark complexion, wearing Burkha, inadequate exposure to sunlight, and presence of diabetes were identified as statistically significant predictors of Vitamin D deficiency.
Conclusion:
We report a high prevalence of Vitamin-D deficiency in patients attending medicine OPD. Thus, patients with generalized complaints may be evaluated for serum Vitamin D levels.
Keywords: Diabetes, hypertension, ischemic heart disease, Vitamin D
INTRODUCTION
Vitamin D deficiency is known to be associated with rickets in children and osteomalacia and osteoporosis in adults. Its association with various cardiovascular, infectious (tuberculosis), and cancers has been recently reported.[1] Thus, Vitamin D deficiency has a bearing not only on skeletal but also on extraskeletal diseases including neuromuscular, endocrinal, cardiovascular, degenerative, and autoimmune diseases.[2] It is known that on exposure to ultraviolet B rays, Vitamin D is synthesized in the skin. Vitamin D deficiency is multi-factorial in origin, and some of the risk factors are poor sunlight exposure, skin pigmentation, and dietary insufficiency. Atmospheric pollution has also been attributed to Vitamin D deficiency in children.[3] Intriguingly, despite ample sunshine, Vitamin D deficiency is reported in widely prevalent tropical countries such as India.[4,5,6,7,8,9] Cultural and social practices including lifestyle pattern such as clothing (Burkha or veil including black socks covering hand and feet) that limit the exposure to sunlight impact the level of Vitamin D in the body. Strict vegetarian diet, poor source of Vitamin D and B12, folic acid, and pyridoxine may attribute to premature ischemic heart disease (IHD) along with hyperhomocysteinemia.[10,11]
Burden of Vitamin D deficiency has been documented by many investigators recently. Moderate-to-severe Vitamin D deficiency is reported in urban Indian population, despite availability of abundant sunshine.[2,6,9,12] In addition, the high prevalence of clinical and biological hypovitaminosis D in apparently healthy school children in India has been reported.[13] Meticulous and close clinical examination during school time is essential to detect accurate Vitamin D deficiency in school children.[13] Because of asymptomatic or vague nature of symptoms of Vitamin D deficiency, it remains undetected in a majority of individuals.[6] Clinical detection of symptomatic cases is the tip of iceberg of Vitamin D deficiency. Myth of routine exposure to sunshine does not require extra Vitamin D, results in severe asymptomatic Vitamin D deficiency in Indian population. Objective of this study was to estimate the prevalence of Vitamin D deficiency in outpatients of a secondary level rural hospital.
METHODS
Settings, patients, and procedures
This hospital-based cross-sectional study was conducted at a peripheral hospital situated at west coast region at Taluka (block) place on Mumbai-Goa highway. This hospital caters to general medicine patients coming from around 120 small villages in neighborhood. Consecutive patients attending outpatient department (OPD) were invited to participate in this study. Patients from all age group, religion, gender, and occupation who attended OPD were eligible to participate. Written informed consent was obtained, and then participants were subjected to clinical and laboratory investigations.
We have collected information on age, gender, and prevailing symptoms and known medical disorders such as diabetes, hypertension, and IHDs. We have also probed for symptoms such as weakness, laziness, muscle aches, and bony pain. Then, general and systemic clinical examination was done on every patient. After obtaining written consent, 3 ml of blood sample was collected by phlebotomy in dry glass test tube and was transferred in cool-box to the laboratory. The term “Vitamin D” refers to compound Vitamin D3 (cholecalciferol) or Vitamin D2 (ergocalciferol). Vitamin D3 level in serum was estimated by electro-chemiluminescence on cobas elecsys 411 fully automated system. Following are the operation definitions of variables used in the study.
Dark complexion – Extensive black color of the skin. Often seen in farmers and workers exposed to summer sun [Figure 1]
Burkha or veil – Enveloping outer garment worn by women in some Islamic traditions to cover their bodies when in public. Muslim females usually wear it from age above 12 years. Mostly, black Burkha is used which completely covers body except for eyes. Some even wear black socks and hand gloves. This practice was probed and routine users have been classified in Burkha practice category
Exposure to sunlight – The person who is directly exposed to sunlight either at workplace or at other places for at least 90–120 min in a day is classified in this category
Nonexposure – Those not included in exposure to sunlight category. Commonly includes office workers, closed industrial workers, shop and business owners, and homemakers
Hypertension – Those who are already taking anti-hypertensive therapy were included. In addition, repeated three reading blood pressure by mercury sphygmomanometer at 5 min interval was measured for each participant and those with blood pressure systolic >140 or diastolic >90 mm hg included as hypertension
IHDs - Classic manifestation of IHD is Angina. Angina is characterized by heaviness in the chest, squeezing or a burning feeling, or suffocation or difficulty in breathing. Chest pain or discomfort radiates to left shoulder, neck, jaw, epigastrium, and inner side of the left arm. Its intensity is built up over period of minutes (<2–10 min) and not in seconds. Pain may start with exercise or psychological stress and strain or cold weather. However, acute coronary syndrome most commonly occurs without any precipitating factors. Unstable angina is more severe with intolerable chest pain at rest, recent onset of increased in severity. Acute myocardial infarction sudden onset of retro-sternal severe agonizing chest pain lasting for >30 min or longer referred to both shoulder and arms, associated with shortness of breath, profuse sweating, weakness, nausea and vomiting, or shock.[9] Electrocardiograms (ECG). Angina-resting ECG may be normal during chest pain ST-T changes suggestive IHD or positive stress test further evaluated by coronary angiography
Diabetes mellitus – Those who are already taking anti-diabetes therapy were included. In addition, every participant was subjected to blood glucose estimation. Fasting blood sugar 126 mg/dl or ≥7.0 mmol/L, (normal 100 mg/dl or < 5.6 Mmol/L, hemoglobin A1c <5.6%) 2 h of postglucose (1 g kg glucose) 200 mg/dl or 11.1 mmol (normal 140 mg/dl or <7.8 mmol) Hba1c >6.5%.
Vitamin D deficiency is defined as 25(OH) D <20 ng/ml, insufficiency as 20–29 ng/ml and sufficiency as ≥30 ng/ml.[2]
Figure 1.

Skin pigmentation in farmer due to daily exposure to heavy sunlight (please close the eyes to obscure the identity)
Sampling and statistical analysis
Required sample size to estimate the prevalence of 50% Vitamin D deficiency with 95% confidence interval (CI) of 46–54% was 600. Final sample size with 10% nonresponse rate was 660. All analyses were performed using Epi-Info 7, CDC, Atlanta, GA, USA. Categorical variables were presented as count and percentage. Numerical variables were summarized as mean and standard deviation when normally distributed and median with inter-quartile range when nonnormally distributed. Prevalence of deficiency was reported as proportion with 95% CI. Comparison of Vitamin D levels across groups was conducted using Mann–Whitney or Kruskal–Wallis tests. Multiple linear regression analysis was used where Vitamin D level was entered as dependent variable and presence of dark complexion, Burkha (veil) wearing, hypertension, diabetes, exposure to sunlight, age, and gender were entered as independent variables. Categorical variables were dummy coded as 0 - No and 1 - Yes for this purpose. P < 0.05 was considered statistically significant.
RESULTS AND ANALYSIS
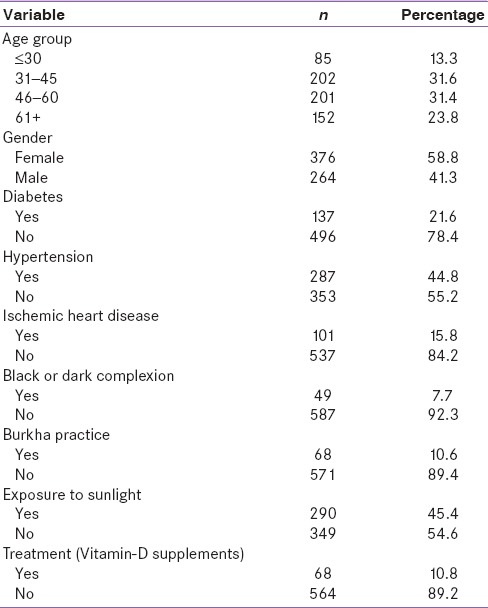
A total of 640 participants from OPD were enrolled in the study. Mean age was 49.4 years (standard deviation 16.4) which included participants from minimum of 9 years of age to maximum of 95 years. Distribution of participants as per their gender, complexion, Burkha practices, disease status, and treatment among various categories of vitamin D level is shown in Table 1.
Table 1.
Distribution of participants as per Vitamin D level categories and demographic and clinical features
Mean vitamin D level was 19.43 with a standard deviation of 15.12 and was nonnormally distributed [Figure 2].
Figure 2.
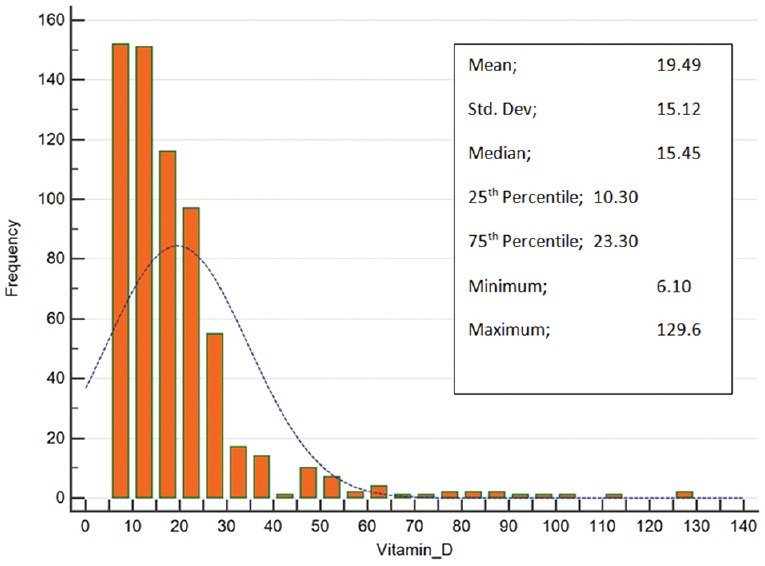
Distribution of Vitamin D Levels
Vitamin D deficiency (<20 ng/ml) was observed in 419 (65.4% 95% CI: 61.7–69.1) and insufficiency (20–29.9 ng/ml) was observed in 152 (23.5%) patients.
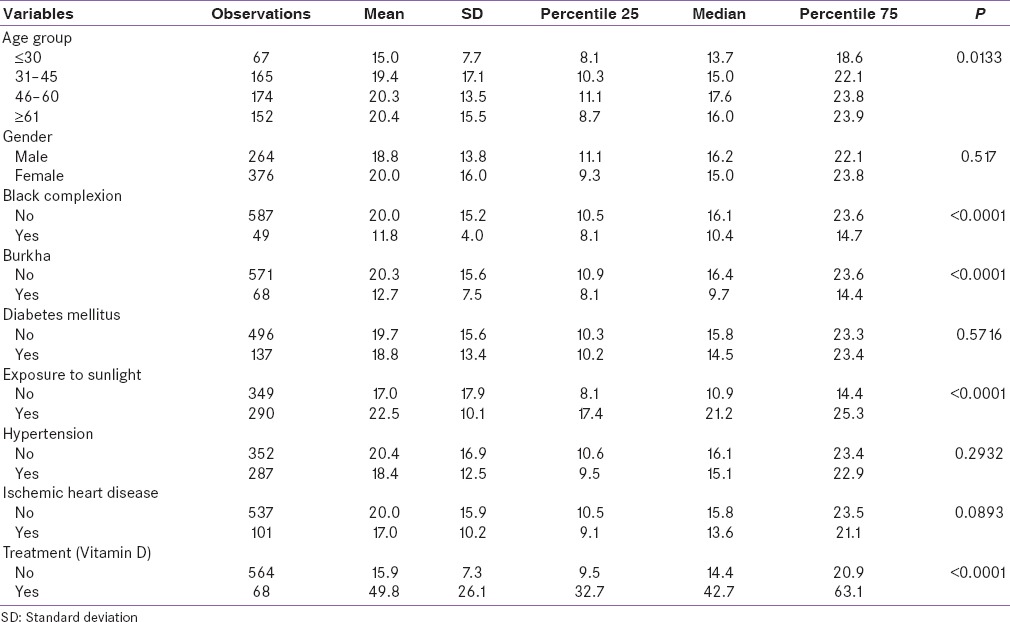
We compared Vitamin D level across age group, gender, Veil (Burkha)-wearing practices, exposure status, and disease and treatment status by using Kruskal–Wallis or Mann–Whitney tests appropriately. It is evident from Table 2 that Vitamin D levels were significantly lower is age group below 30 years, people with black/dark complexion, those who wear Burkha, those who do not have adequate exposure to sunlight, and those who did not receive any treatment.
Table 2.
Distribution of participants as per Vitamin D level and demographic and clinical features
We have performed multiple linear regression analyses where Vitamin-D level was dependent variable and age group, gender, Veil (Burkha)-wearing practices, exposure status, disease, and treatment status were independent variables. Statistically significant predictors of Vitamin D level were treatment, exposure status, presence of diabetes mellitus, Burkha practices, and dark complexion [Tables 3a and b].
Table 3a.
Results of multiple linear regression
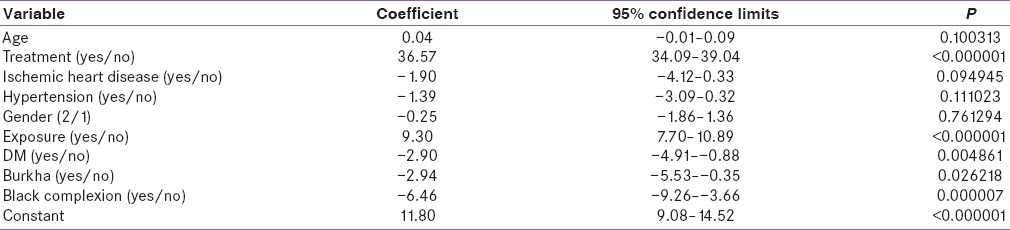
Table 3b.
Results of multiple linear regression

DISCUSSION
Our study shows a high prevalence of Vitamin-D deficiency among general medicine outpatients of rural hospital. All age groups are prone for the development of Vitamin D deficiency despite of plenty sunshine.[14] However, dark complexion and Muslim women with routine use of Burkha are more susceptible for severe Vitamin D deficiency. In the present study, we noted that Vitamin D deficiency is observed in patients with diabetes, hypertension, and IHD. Our study is based on the fact that Vitamin D is one of the most underrated nutrients, and it is time to address this issue. Vitamin D is not just a vitamin, but actually a hormone, thus a class by itself and its predominant renal metabolic product, calcitriol, a secosteroid hormone, targets over 1000 genes in the human body. Role of Vitamin D deficiency has been implicated as factor responsible in the pathogenesis of 17 varieties of cancers, heart disease, stroke, hypertension, autoimmune diseases, diabetes, depression, chronic pain, osteoarthritis, osteoporosis, myopathies, birth defect, dental diseases, and many more diseases.[15]
Professor Michael Hollick has extensively worked on vitamin D and documented that a few minutes in the summer sun produces 100 times more Vitamin D than daily requirement.[16] Sufficient serum level of vitamin D is crucial to maintain the autocrine and paracrine functions. Low Vitamin D results in oncogenesis and affects the basic cell biology.[15]
In the present report, we found Muslim women wearing Burkha and persons having dark complexion had severe and significant Vitamin D deficiency. Biological balance of Vitamin D is done by human skin. A total of 20,000 units of vitamin D can be made in skin every day, and the sunlight that makes Vitamin D begins to break it down. After skin turns dark (tan), because of heavy and prolonged exposure to sunlight, the dark skin synthesizes less amount of Vitamin D which may be up to 10,000 units.[17] Thus, melanin content of skin may regulate cholecalciferol production.[18] Humans have a natural system in the skin that prevents Vitamin D toxicity. All sunscreens block the Vitamin D production.[19]
Vitamin D receptors have been demonstrated in almost all major cardiovascular tissues including myocardial cells, arterial wall cells, and immune cells.[15] Vitamin D plays an important role in cardiovascular functions and diseases including thrombosis, inflammation, and rennin-angiotensin system. Vitamin D deficiency results in degenerative cardiovascular diseases and vascular calcification. Thus, the presence of Vitamin D deficiency is significantly high among individuals with cardiovascular diseases including atherosclerosis IHD, and hypertension.[20,21,22]
We found an inverse relationship of Vitamin D level and diabetes. Prevalence of diabetes is high in urban as well rural India.[23] By 2030, India will be the world capital for diabetes. Vitamin D plays a vital role in diabetes mellitus because it improves beta cell function by increasing intracellular ionized calcium which enhances insulin release in circulation. It improves the insulin resistance by sensitizing the insulin receptors to circulating insulin. By inhibiting beta cell apoptosis, it delays the insulin dependency in diabetes mellitus.[24]
Chronic Vitamin D deficiency in adults and in old age results in osteomalacia, osteoporosis, muscle weakness, and increased risk of fall and long bone fractures. In particular, hip bone fracture with trivial trauma is common in old population.[2,15]
Considering the vast deleterious effects of Vitamin D deficiency, its supplementation is essential if the serum D levels are below 30 ng/ml. Many people will not have any particular symptom although they have Vitamin D deficiency. Vitamin D supplementation can be done by exposure to sun or artificial light, oral Vitamin D supplements to maintain 25 (OH) level between 30 and 70 ng/ml.
Because of wide publicity regarding vitamin D and health, public become more aware of vitamin D and consumed without doctor prescription, may develop hypervitaminosis[headache, anorexia] or vitamin D toxicity. Hence regular monitoring of blood vitamin is crucial important to prevent vitamin D toxicity.
CONCLUSION
We report a high prevalence of Vitamin D deficiency in general medicine outpatients of rural hospital. It was higher than the prevalence reported for general population. Thus, physicians should be vigilant to rule out Vitamin D deficiency and consider supplementation in those who are at risk, particularly persons with dark complexion, routine Burkha usage, inadequate exposure to sunlight, and chronic disease patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We are grateful to Ashwin Kotnis assistant professor biochemistry at AIIMS Bhopal in language editing.
REFERENCES
- 1.Trilok Kumar G, Chugh R, Eggersdorfer M. Poor Vitamin D status in healthy populations in India: A review of current evidence. Int J Vitam Nutr Res. 2015;85:185–201. doi: 10.1024/0300-9831/a000228. [DOI] [PubMed] [Google Scholar]
- 2.Ritu G, Gupta A. Vitamin D deficiency in India: Prevalence, causalities and interventions. Nutrients. 2014;6:729–75. doi: 10.3390/nu6020729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Agarwal KS, Mughal MZ, Upadhyay P, Berry JL, Mawer EB, Puliyel JM. The impact of atmospheric pollution on Vitamin D status of infants and toddlers in Delhi, India. Arch Dis Child. 2002;87:111–3. doi: 10.1136/adc.87.2.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sahu M, Bhatia V, Aggarwal A, Rawat V, Saxena P, Pandey A, et al. Vitamin D deficiency in rural girls and pregnant women despite abundant sunshine in northern India. Clin Endocrinol (Oxf) 2009;70:680–4. doi: 10.1111/j.1365-2265.2008.03360.x. [DOI] [PubMed] [Google Scholar]
- 5.Goswami R, Kochupillai N, Gupta N, Goswami D, Singh N, Dudha A. Presence of 25(OH) D deficiency in a rural North Indian village despite abundant sunshine. J Assoc Physicians India. 2008;56:755–7. [PubMed] [Google Scholar]
- 6.Goswami R, Gupta N, Goswami D, Marwaha RK, Tandon N, Kochupillai N. Prevalence and significance of low 25-hydroxyvitamin D concentrations in healthy subjects in Delhi. Am J Clin Nutr. 2000;72:472–5. doi: 10.1093/ajcn/72.2.472. [DOI] [PubMed] [Google Scholar]
- 7.Ghai B, Bansal D, Kapil G, Kanukula R, Lavudiya S, Sachdeva N. High Prevalence of hypovitaminosis D in Indian chronic low back patients. Pain Physician. 2015;18:E853–62. [PubMed] [Google Scholar]
- 8.Harinarayan CV, Ramalakshmi T, Prasad UV, Sudhakar D, Srinivasarao PV, Sarma KV, et al. High prevalence of low dietary calcium, high phytate consumption, and Vitamin D deficiency in healthy South Indians. Am J Clin Nutr. 2007;85:1062–7. doi: 10.1093/ajcn/85.4.1062. [DOI] [PubMed] [Google Scholar]
- 9.Marwaha RK, Tandon N, Garg MK, Kanwar R, Narang A, Sastry A, et al. Vitamin D status in healthy Indians aged 50 years and above. J Assoc Physicians India. 2011;59:706–9. [PubMed] [Google Scholar]
- 10.Bawaskar HS. Homocysteine: Often neglected but common culprit of coronary heart diseases. J Cardiovasc Dis Res. 2014;5:40–3. [Google Scholar]
- 11.Bawaskar HS, Himmatrao BP, Bawaskar PH. Homocysteine and cardiovascular system. Int Res J Pharm Sci. 2015;6:1–7. [Google Scholar]
- 12.Arya V, Bhambri R, Godbole MM, Mithal A. Vitamin D status and its relationship with bone mineral density in healthy Asian Indians. Osteoporos Int. 2004;15:56–61. doi: 10.1007/s00198-003-1491-3. [DOI] [PubMed] [Google Scholar]
- 13.Marwaha RK, Sripathy G. Vitamin D & bone mineral density of healthy school children in northern India. Indian J Med Res. 2008;127:239–44. [PubMed] [Google Scholar]
- 14.Joshi SR. Vitamin D paradox in plenty sunshine in rural India – An emerging threat. J Assoc Physicians India. 2008;56:749–52. [PubMed] [Google Scholar]
- 15.Pludowski P, Holick MF, Pilz S, Wagner CL, Hollis BW, Grant WB, et al. Vitamin D effects on musculoskeletal health, immunity, autoimmunity, cardiovascular disease, cancer, fertility, pregnancy, dementia and mortality-a review of recent evidence. Autoimmun Rev. 2013;12:976–89. doi: 10.1016/j.autrev.2013.02.004. [DOI] [PubMed] [Google Scholar]
- 16.Holick MF. Calcium and Vitamin D. Diagnostics and therapeutics. Clin Lab Med. 2000;20:569–90. [PubMed] [Google Scholar]
- 17.Holick MF. The cutaneous photosynthesis of previtamin D3: A unique photoendocrine system. J Invest Dermatol. 1981;77:51–8. doi: 10.1111/1523-1747.ep12479237. [DOI] [PubMed] [Google Scholar]
- 18.Clemens TL, Adams JS, Henderson SL, Holick MF. Increased skin pigment reduces the capacity of skin to synthesise vitamin D3. Lancet. 1982;1:74–6. doi: 10.1016/s0140-6736(82)90214-8. [DOI] [PubMed] [Google Scholar]
- 19.Matsuoka LY, Wortsman J, Hanifan N, Holick MF. Chronic sunscreen use decreases circulating concentrations of 25-hydroxyvitamin D. A preliminary study. Arch Dermatol. 1988;124:1802–4. [PubMed] [Google Scholar]
- 20.Kassi E, Adamopoulos C, Basdra EK, Papavassiliou AG. Role of Vitamin D in atherosclerosis. Circulation. 2013;128:2517–31. doi: 10.1161/CIRCULATIONAHA.113.002654. [DOI] [PubMed] [Google Scholar]
- 21.Norman PE, Powell JT. Vitamin D and cardiovascular disease. Circ Res. 2014;114:379–93. doi: 10.1161/CIRCRESAHA.113.301241. [DOI] [PubMed] [Google Scholar]
- 22.Siasos G, Tousoulis D, Oikonomou E, Maniatis K, Kioufis S, Kokkou E, et al. Vitamin D serum levels are associated with cardiovascular outcome in coronary artery disease. Int J Cardiol. 2013;168:4445–7. doi: 10.1016/j.ijcard.2013.06.151. [DOI] [PubMed] [Google Scholar]
- 23.Unnikrishnan R, Anjana RM, Mohan V. Diabetes mellitus and its complications in India. Nat Rev Endocrinol. 2016;12:357–70. doi: 10.1038/nrendo.2016.53. [DOI] [PubMed] [Google Scholar]
- 24.Pittas AG, Harris SS, Stark PC, Dawson-Hughes B. The effects of calcium and Vitamin D supplementation on blood glucose and markers of inflammation in nondiabetic adults. Diabetes Care. 2007;30:980–6. doi: 10.2337/dc06-1994. [DOI] [PubMed] [Google Scholar]