

Abstract
Purpose
The hedgehog (Hh) signaling pathway, a key regulator of cell growth and differentiation during development is implicated in pathogenesis of certain cancers. Vismodegib (GDC-0449) is a small-molecule inhibitor of smoothened, a key component of Hh signaling. This phase I trial assessed GDC-0449 treatment in patients with solid tumors refractory to current therapies or for which no standard therapy existed.
Experimental Design
Sixty-eight patients received GDC-0449 at 150 mg/d (n = 41), 270 mg/d (n = 23), or 540 mg/d (n = 4). Adverse events, tumor responses, pharmacokinetics, and pharmacodynamic down-modulation of GLI1 expression in noninvolved skin were assessed.
Results
Thirty-three of 68 patients had advanced basal cell carcinoma (BCC), 8 had pancreatic cancer, 1 had medulloblastoma; 17 other types of cancer were also represented. GDC-0449 was generally well-tolerated. Six patients (8.8%) experienced 7 grade 4 events (hyponatremia, fatigue, pyelonephritis, presyncope, resectable pancreatic adenocarcinoma, and paranoia with hyperglycemia), and 27.9% of patients experienced a grade 3 event [most commonly hyponatremia (10.3%), abdominal pain (7.4%), and fatigue (5.9%)]. No maximum tolerated dose was reached. The recommended phase II dose was 150 mg/d, based on achievement of maximal plasma concentration and pharmacodynamic response at this dose. Tumor responses were observed in 20 patients (19 with BCC and 1 unconfirmed response in medulloblastoma), 14 patients had stable disease as best response, and 28 had progressive disease. Evidence of GLI1 down-modulation was observed in noninvolved skin.
Conclusions
GDC-0449 has an acceptable safety profile and encouraging anti-tumor activity in advanced BCC and medulloblastoma. Further study in these and other cancer types is warranted.
Introduction
The hedgehog (Hh) signaling pathway is a key regulator of cell growth and differentiation during development. While the Hh pathway is inactive in most normal adult tissues, Hh pathway reactivation has been implicated in the pathogenesis of several cancers (1–8). Aberrant Hh signaling was initially shown in patients with Gorlin syndrome, a genetic disorder associated with predisposition to basal cell carcinoma (BCC) and medulloblastoma (1–4). Excessive and/or inappropriate expression of the Hh ligand has since been implicated in the pathogenesis of a number of sporadic cancers, such as colon, pancreas, prostate, and B cell malignancies (5–7). Disruption of Hh signaling may therefore be beneficial in a broad array of tumor types.
The Hh pathway controls epithelial and mesenchymal interactions in many tissues (9). Extracellular Hh protein binds to patched-1 (PTCH1), a 12-transmembrane receptor, and prevents PTCH1-mediated inhibition of signaling by smoothened (SMO), a 7-transmembrane protein (Fig. 1A; refs. 9, 10). Signaling by SMO results in activation of GLI transcription factors and consequent induction of Hh target genes, including GLI1 and PTCH1 (9, 10).
Figure 1.
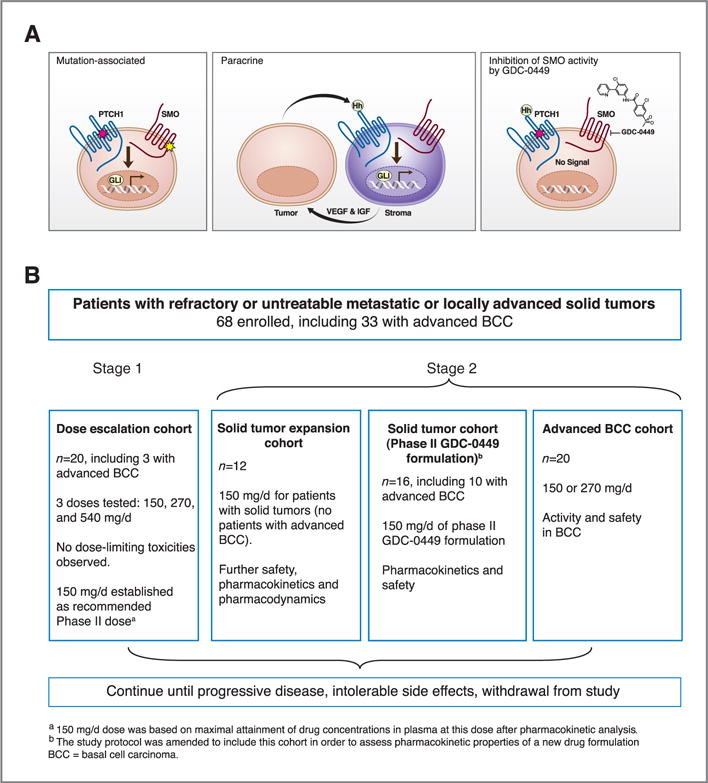
Abnormalities in hedgehog pathway signaling, mechanism of GDC-0449 activity, and study schema. A, mechanisms of abnormal hedgehog signaling associated with different cancers are shown in the first 3 panels. Type I, left, BCC and medulloblastoma are associated with mutations in hedgehog signaling pathways; mutations in PTCH1 (pink star) can prevent PTCH1 from inhibiting SMO activity, or mutations in SMO (yellow star) can constitutively activate SMO, resulting in downstream effects of increased GL1 expression. Type III, middle, production of hedgehog ligand by tumor cells may stimulate stromal cells to produce factors associated with tumor growth, possibly including vascular endothelial growth factor (VEGF) and insulin-like growth factor (IGF). The right panel shows how GDC-0449 inhibits hedgehog pathway signaling by inhibiting the activity of SMO. B, a schema for the phase I study.
The vast majority of BCCs contain mutations that result in inactivation of PTCH1 (refs. 2, 11; loss-of-function, or, less frequently, constitutive activation of SMO (ref. 12; gain-of-function; Fig. 1A, left), leading to activation of the Hh pathway. Similar pathway activating mutations have been noted in medulloblastoma (4, 13). In contrast, other types of cancer that have been linked to aberrant Hh signaling are not known to harbor Hh-related mutations, but are instead associated with over-expression of Hh ligands by tumor cells. Hh ligands produced by tumors may stimulate tumor growth and/or survival in a paracrine manner, whereby ligands produced by tumor cells activate the pathway in the surrounding stromal cells leading to the secretion or expression of stromal mediators that enhance tumor growth and survival (5–8; Fig. 1A, middle). In addition, Hh pathway activation has also been proposed to occur in cancer stem cells in some tumor types such as chronic myelogenous leukemia (CML; refs. 14, 15). These multiple mechanisms may be amenable to inhibition of Hh pathway signaling through SMO (10).
The novel SMO inhibitor vismodegib (GDC-0449; 2-chloro-N-[4-chloro-3-pyridin-2-yl-phenyl]-4-methanesulfonyl benzamide, molecular weight 421.30 g/mol, Fig. 1A, right), was discovered by high throughput screening of a small molecule compound library, with subsequent optimization through medicinal chemistry (5, 10, 16–18). GDC-0449 is a selective Hh pathway inhibitor that blocks Hh signaling by binding to SMO and inhibiting activation of downstream Hh target genes (Fig. 1A, right), with greater potency and more favorable pharmaceutical properties than the steroidal alkaloid cyclopamine (19, 20). GDC-0449 has anti-tumor activity in a mouse model of medulloblastoma and in primary human tumor cell xenograft models, including colorectal cancer and pancreatic carcinoma; its effects correlated with blockade of the Hh pathway (5, 21).
A phase I trial was initiated to evaluate the safety and tolerability of daily oral administration of GDC-0449 in patients with locally advanced or metastatic solid tumors, refractory to standard therapy, or for whom no standard therapy was available. Early in the study, activity was observed in the first two treated patients with metastatic or locally advanced BCC, and the study was amended to enroll additional patients with advanced BCC (17). A total of 33 patients with advanced BCC were enrolled in this trial, with a previously reported overall response rate of 55%, including 16 partial and 2 complete responses (17). A partial but transient tumor response in a patient with medulloblastoma was described in a separate case report (18). GDC-0449 was generally well-tolerated in these patients, with an acceptable safety profile.
This report summarizes final safety, efficacy, and pharmacokinetic results of this phase I trial for all patients with advanced or metastatic solid tumors.
Methods
Study objectives
The primary objectives of this phase I clinical trial were to evaluate safety and tolerability of escalating doses of GDC-0449, to estimate the maximum tolerated dose (MTD), to characterize dose-limiting toxicities and pharmacokinetic properties, and to determine the recommended phase II dose and schedule. The secondary objectives were to assess whether inhibition of Hh signaling by GDC-0449 could be reliably measured in human hair follicles and/or skin for characterization of pharmacodynamic effects, and to make a preliminary assessment of tumor response in patients with advanced solid tumors. GDC-0449 was discovered by Genentech, Inc., and was jointly validated through a series of preclinical studies performed under a collaborative agreement between Genentech, Inc., and Curis, Ltd. This phase I clinical trial was designed jointly by the clinical investigators and Genentech, Inc.
Eligibility
All patients were at least 18 years of age, and had advanced or metastatic solid malignancies that were refractory to standard therapy, or for which no standard therapy existed (as determined by the investigator). Patients had Eastern Cooperative Oncology Group performance status (ECOG PS) of ≤2. Women of child-bearing potential had documentation of a negative pregnancy test. GDC-0449 treatment did not begin until >3 weeks after the patient’s last therapy or major surgical procedure. Exclusion criteria included major organ dysfunction, a long QT interval or any medication known to prolong the QT interval, active infection requiring intravenous antibiotics, pregnancy, an inability to swallow pills, or other conditions that would contraindicate investigational drug use in the opinion of the investigator.
Study design
This was an open-label, multicenter, two stage phase I trial to evaluate the safety and tolerability of GDC-0449 in patients with a variety of solid tumors that were refractory to standard therapy. The study design has been described (17), and is shown schematically in Fig. 1B. Patients provided written informed consent according to federal and institutional guidelines before study procedures began. Human investigations were performed after approval by a human investigations committee and in accordance with an assurance filed with and approved by the Department of Health and Human Services.
A total of 68 patients enrolled in the study at three centers. Stage 1 was a dose escalation stage, designed to estimate the MTD of GDC-0449. Patients received a single oral dose of GDC-0449 on day 1, followed by daily administration at the same dose beginning on day 8; 7 patients received 150 mg/d, 9 received 270 mg/d, and 4 received 540 mg/d. Patients with dose-limiting toxicities, other intolerable side effects, disease progression, or who did not benefit from treatment, as decided by the investigator, were discontinued from treatment.
Stage 2 included an expansion cohort of 12 patients with solid tumors (none of whom had advanced BCC) who began continuous daily dosing at 150 mg/d on day 1, to further assess the safety profile, pharmacokinetics, and pharmacodynamics of GDC-0449. After a study amendment, two further cohorts were added: a cohort of 16 patients (including 10 with advanced BCC), to investigate pharmacokinetic properties of a new GDC-0449 formulation at 150 mg/d; and a cohort of 20 patients with advanced BCC (treated at150 or 270 mg/d), to evaluate safety and efficacy, based on encouraging response of 2 patients in stage 1 with advanced BCC. Patients in stage 2 were treated until disease progression, occurrence of intolerable side effects, or study withdrawal.
Data collection
For the first 6 weeks, all patients underwent weekly physical examinations, along with monitoring of vital signs, ECOG PS, electrocardiographic evaluations, blood counts, and chemical analyses. Subsequent assessments were conducted every 4 weeks. Data concerning adverse events were collected for up to 30 days after the last study treatment for all patients who received any amount of GDC-0449. Graded adverse events (number and percent) were summarized and reported according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events (version 3.0). Per protocol, any deaths reported within 30 days of discontinuation of study drug treatment were to be reported as adverse events, including deaths due to disease progression.
For patients with radiologically measurable disease, tumor assessment was performed at baseline, after 8 weeks of continuous dosing, and every 8 weeks thereafter with the use of Response Evaluation Criteria in Solid Tumors (RECIST; version 1.0; ref. 22) to determine stable disease, progressive disease, and best overall response. A complete or partial response was determined on two consecutive occasions ≥4 weeks apart. For patients with locally advanced BCC that was not radiographically measurable, tumors were assessed by physical examination. Because of the heterogeneity of tumor locations and characteristics in these patients, RECIST was not utilized; rather, a complete response was defined as complete disappearance of a palpable or visible tumor, and a partial response was defined as a reduction of more than 50% in the diameter of a palpable or visible tumor. Tumor site biopsy was not required for assessment of complete response. Patients whose tumor diameter did not decrease by 50% but who did not have demonstrable increase in tumor size were assessed as having stable disease.
Pharmacokinetics
Baseline and weekly plasma samples were collected from patients in stages 1 and 2 for the first 4 weeks, and then at approximately monthly intervals, more frequent sampling was conducted during the first week for stage 1 patients. Total and unbound plasma levels of GDC-0449 were determined using liquid chromatography-tandem mass spectrometry (23). Unbound GDC-0449 was first purified from bound protein by dialysis. The steady state levels of GDC-0449 (Css) were calculated by averaging all available concentrations after 21 days of daily dosing.
Pharmacodynamic assessment of GLI1 expression
RNA was extracted from biopsy specimens of non-involved skin or hair follicles at baseline and at 7 and 21 days after the start of daily drug therapy. Patients were not required to provide tumor-biopsy samples. Expression levels of GLI1 were assessed by TaqMan quantitative real-time polymerase-chain-reaction (qRT-PCR) assay and calculated by the 2−ΔCt method, in which the cycling threshold (Ct) of GLI1 was normalized to the Ct of SMO and expressed as a power of
(Primer and probe sequences have been described by Von Hoff and colleagues, Table 1 in the Supplementary Appendix; ref. 17) Control mRNA was obtained from formalin-fixed, paraffin-embedded samples of normal skin and hair follicles from patients who were not enrolled in the study.
Results
Patient population
From January 2007 through December 2008, 68 patients enrolled in the study: 33 had metastatic or locally advanced BCC, and 35 had other solid tumors, including 8 with pancreatic cancer, 3 each with colorectal cancer, mesothelioma, or small cell lung cancer, and 1 with medulloblastoma (Table 1). Sixty-four percent of patients had ECOG PS of 1 and 4.5% had ECOG PS of 2. The majority of patients had received prior surgery (98.5%), radiotherapy (52.9%), and/or systemic therapy (70.6%).
Table 1.
Baseline demographics and patient characteristics (N = 68)
| Age, y | |
| Median | 54.0 |
| Range | 26–84 |
| Sex, n (%) | |
| Male | 44 (64.7) |
| Female | 24 (35.3) |
| Race or ethnic background, n (%) | |
| White | 66 (97.1) |
| Black or African American | 2 (2.9) |
| ECOG score, n (%)a (n = 67) | |
| 0 | 21 (31.3) |
| 1 | 43 (64.2) |
| 2 | 3 (4.5) |
| Tumor type, n (%) | |
| Basal cell carcinoma | 33 (48.5) |
| Pancreatic | 8 (11.8) |
| Colorectal | 3 (4.4) |
| Mesothelioma | 3 (4.4) |
| Small cell lung | 3 (4.4) |
| Adenocystic carcinoma | 2 (2.9) |
| Adrenocortical carcinoma | 2 (2.9) |
| Parotid gland | 2 (2.9) |
| Prostate | 2 (2.9) |
| Medulloblastoma | 1 (1.5) |
| Otherb | 9 (13.2) |
| Previous therapies, n (%) | |
| Surgery | 67 (98.5) |
| Radiotherapy | 36 (52.9) |
| Systemic therapyc | 48 (70.6) |
ECOG scores ranging from 0 to 5, with higher scores indicating a greater severity of illness.
Other tumor types included one each of appendix, bladder, carcinoid, chondrosarcoma, endometrial, gastric, liver/biliary, melanoma, and renal.
Includes hormonal, other biologic, chemotherapy, and other systemic therapy.
Safety
GDC-0449 was generally well-tolerated in this study, with no dose-limiting toxicities observed. The most frequently reported adverse events (occurring in greater than 30% of patients) were muscle spasms, dysgeusia (alteration of taste sensation), fatigue, alopecia (including eyelashes, eyebrows, and body hair), and nausea (Table 2).
Table 2.
Most frequently reported adverse events (occurring in >10% of patients)
| Grade of adverse event, n (%)a
|
|||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | Total | |
| Muscle spasms | 26 (38.2) | 5 (7.4) | 1 (1.5) | 0 | 32 (47.1) |
| Dysgeusia | 25 (36.8) | 3 (4.4) | 0 | 0 | 28 (41.2) |
| Fatigue | 15 (22.1) | 8 (11.8) | 4 (5.9) | 1 (1.5) | 28 (41.2) |
| Alopecia | 22 (32.4) | 2 (2.9) | 0 | 0 | 24 (35.3) |
| Nausea | 18 (26.5) | 4 (5.9) | 1 (1.5) | 0 | 23 (33.8) |
| Decreased appetite | 15 (22.1) | 4 (5.9) | 0 | 0 | 19 (27.9) |
| Diarrhea | 14 (20.6) | 4 (5.9) | 0 | 0 | 18 (26.5) |
| Weight decreased | 11 (16.2) | 4 (5.9) | 3 (4.4) | 0 | 18 (26.5) |
| Cough | 13 (19.1) | 2 (2.9) | 0 | 0 | 15 (22.1) |
| Back pain | 8 (11.8) | 3 (4.4) | 2 (2.9) | 0 | 13 (19.1) |
| Dyspnea | 6 (8.8) | 4 (5.9) | 3 (4.4) | 0 | 13 (19.1) |
| Constipation | 9 (13.2) | 3 (4.4) | 0 | 0 | 12 (17.6) |
| Vomiting | 8 (11.8) | 3 (4.4) | 1 (1.5) | 0 | 12 (17.6) |
| Abdominal pain | 3 (4.4) | 3 (4.4) | 5 (7.4) | 0 | 11 (16.2) |
| Anxiety | 7 (10.3) | 3 (4.4) | 0 | 0 | 10 (14.7) |
| Hyponatremia | 1 (1.5) | 1 (1.5) | 7 (10.3) | 1 (1.5) | 10 (14.7) |
| Insomnia | 8 (11.8) | 1 (1.5) | 0 | 0 | 9 (13.2) |
| Pruritus | 9 (13.2) | 0 | 0 | 0 | 9 (13.2) |
| Upper respiratory tract infection | 7 (10.3) | 2 (2.9) | 0 | 0 | 9 (13.2) |
| Abdominal pain upper | 5 (7.4) | 3 (4.4) | 0 | 0 | 8 (11.8) |
| Dyspepsia | 7 (10.3) | 1 (1.5) | 0 | 0 | 8 (11.8) |
| Musculoskeletal chest pain | 3 (4.4) | 4 (5.9) | 1 (1.5) | 0 | 8 (11.8) |
| Pyrexia | 6 (8.8) | 1 (1.5) | 1 (1.5) | 0 | 8 (11.8) |
| Abdominal distension | 7 (10.3) | 0 | 0 | 0 | 7 (10.3) |
| Arthralgia | 6 (8.8) | 1 (1.5) | 0 | 0 | 7 (10.3) |
| Erythema | 6 (8.8) | 1 (1.5) | 0 | 0 | 7 (10.3) |
| Hypokalemia | 7 (10.3) | 0 | 0 | 0 | 7 (10.3) |
| Hypomagnesemia | 7 (10.3) | 0 | 0 | 0 | 7 (10.3) |
| Pain | 5 (7.4) | 0 | 2 (2.9) | 0 | 7 (10.3) |
| Pain in extremity | 5 (7.4) | 2 (2.9) | 0 | 0 | 7 (10.3) |
| Productive cough | 6 (8.8) | 1 (1.5) | 0 | 0 | 7 (10.3) |
| Rhinitis | 7 (10.3) | 0 | 0 | 0 | 7 (10.3) |
Number and percentage of patients experiencing at least 1 event are reported at the highest grade experienced.
Grade 5 (fatal) events related to progression of cancer were reported in 5 patients; per protocol, all deaths within 30 days of discontinuation of study drug were to be reported as adverse events, including those deaths attributed to tumor progression. No other grade 5 events were reported.
Six patients (8.8%) experienced grade 4 events. One patient each experienced grade 4 hyponatremia, fatigue, pyelonephritis, and presyncope, and 1 patient experienced both grade 4 paranoia and hyperglycemia (Table 3). A grade 4 resectable pancreatic adenocarcinoma was newly diagnosed in a patient with metastatic BCC who also had a prior history of testicular cancer, papillary thyroid carcinoma, and mucoepidermoid carcinoma. At the time of enrollment, CT scans did not show a discernible pancreatic mass; an abnormality in the head of the pancreas was first appreciated on routine imaging after 2 months on study, and repeat imaging at 5 months on study showed an ill-defined indeterminate mass, which was followed closely. At approximately 7 months on study, the pancreatic structure became more defined and delineated and a biopsy of this mass was performed, which was consistent with pancreatic adenocarcinoma. The patient was taken off study for management of pancreatic cancer. The treating physicians considered the development of pancreatic cancer in this patient unlikely to be related to GDC-0449.
Table 3.
Listing of all grade ≥3 adverse events
| Grade of adverse event, n (%)a
|
|||
|---|---|---|---|
| 3 | 4 | 5b | |
| Any grade ≥3 AE | 20 (29.4) | 6 (8.8) | 5 (7.4) |
| Pancreatic carcinoma metastatic | 0 | 0 | 2 (3.0) |
| BCC | 0 | 0 | 1 (1.5) |
| Chondrosarcoma | 0 | 0 | 1 (1.5) |
| Pancreatic carcinoma | 0 | 0 | 1 (1.5) |
| Hyponatremia | 7 (10.3) | 1 (1.5) | 0 |
| Fatigue | 4 (5.9) | 1 (1.5) | 0 |
| Hyperglycemia | 1 (1.5) | 1 (1.5) | 0 |
| Pyelonephritis | 0 | 1 (1.5) | 0 |
| Adenocarcinoma pancreas | 0 | 1 (1.5) | 0 |
| Paranoia | 0 | 1 (1.5) | 0 |
| Presyncope | 0 | 1 (1.5) | 0 |
| Abdominal pain | 5 (7.4) | 0 | 0 |
| Weight decreased | 3 (4.4) | 0 | 0 |
| Dyspnea | 3 (4.4) | 0 | 0 |
| Pain | 2 (2.9) | 0 | 0 |
| Dehydration | 2 (2.9) | 0 | 0 |
| Back pain | 2 (2.9) | 0 | 0 |
| Anemia | 1 (1.5) | 0 | 0 |
| Leukopenia | 1 (1.5) | 0 | 0 |
| Lymphopenia | 1 (1.5) | 0 | 0 |
| Atrial fibrillation | 1 (1.5) | 0 | 0 |
| Keratitis | 1 (1.5) | 0 | 0 |
| Nausea | 1 (1.5) | 0 | 0 |
| Vomiting | 1 (1.5) | 0 | 0 |
| Ascites | 1 (1.5) | 0 | 0 |
| Impaired gastric emptying | 1 (1.5) | 0 | 0 |
| Intestinal obstruction | 1 (1.5) | 0 | 0 |
| Pyrexia | 1 (1.5) | 0 | 0 |
| Infection | 1 (1.5) | 0 | 0 |
| Pneumonia | 1 (1.5) | 0 | 0 |
| Urinary tract infection | 1 (1.5) | 0 | 0 |
| Corneal abrasion | 1 (1.5) | 0 | 0 |
| Transfusion reaction | 1 (1.5) | 0 | 0 |
| Blood alkaline phosphatase increased | 1 (1.5) | 0 | 0 |
| Blood potassium increased | 1 (1.5) | 0 | 0 |
| Electrocardiogram QT prolonged | 1 (1.5) | 0 | 0 |
| Myelocyte percentage increased | 1 (1.5) | 0 | 0 |
| Neutrophil count decreased | 1 (1.5) | 0 | 0 |
| Hyperkalaemia | 1 (1.5) | 0 | 0 |
| Muscle spasms | 1 (1.5) | 0 | 0 |
| Musculoskeletal chest pain | 1 (1.5) | 0 | 0 |
| Confusional state | 1 (1.5) | 0 | 0 |
| Hydronephrosis | 1 (1.5) | 0 | 0 |
| Aspiration | 1 (1.5) | 0 | 0 |
| Hypertension | 1 (1.5) | 0 | 0 |
Number and percentage of patients experiencing at least 1 event are reported at the highest grade experienced.
All deaths within 30 days of discontinuation of study drug were to be reported as adverse events, including deaths attributed to tumor progression.
A total of 29.4% of patients experienced grade 3 adverse events as the highest grade. The most common grade 3 adverse event was hyponatremia (7 patients), followed by abdominal pain (5 cases), and fatigue (4 patients). Hyponatremia and fatigue were generally reported to be reversible with temporary discontinuation of drug.
Pharmacokinetics
Steady state plasma concentrations of GDC-0449 by dose level are shown in Fig. 2A. A full analysis of GDC-0449 pharmacokinetic properties is provided in the companion article in this issue of Clinical Cancer Research by Graham and colleagues (24), which describes the role of alpha 1-acid glycoprotein binding in the unusual pharmacokinetic properties of GDC-0449. With multiple daily dosing, all doses showed similar steady state concentrations, based on assessment of bound or unbound drug, and a flat concentration-time profile at steady state (Fig. 2A and B). There was a strong linear correlation (R2 = 0.73) between total GDC-0449 steady state levels and levels of alpha 1-acid glycoprotein protein in plasma [described fully in the companion article in this issue by Graham and colleagues (24)]. Average steady state plasma concentrations were similar across cohorts, including the phase II formulation cohort which supported formulation bridging between the phase I and II formulations (Fig. 2C). The recommended phase II dose was established at 150 mg/d, based on the findings that administering higher drug doses did not result in increased steady state plasma concentrations and that no dose-limiting toxic effects were observed.
Figure 2.
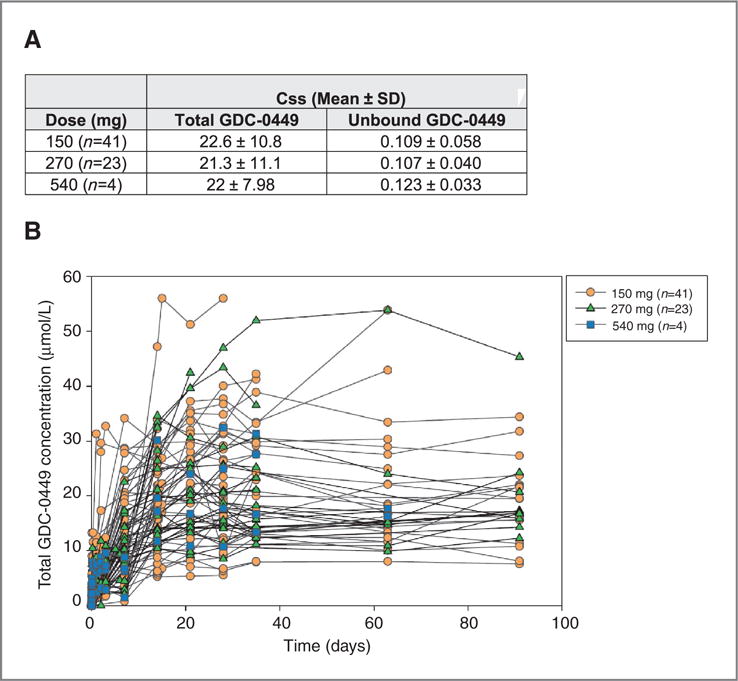
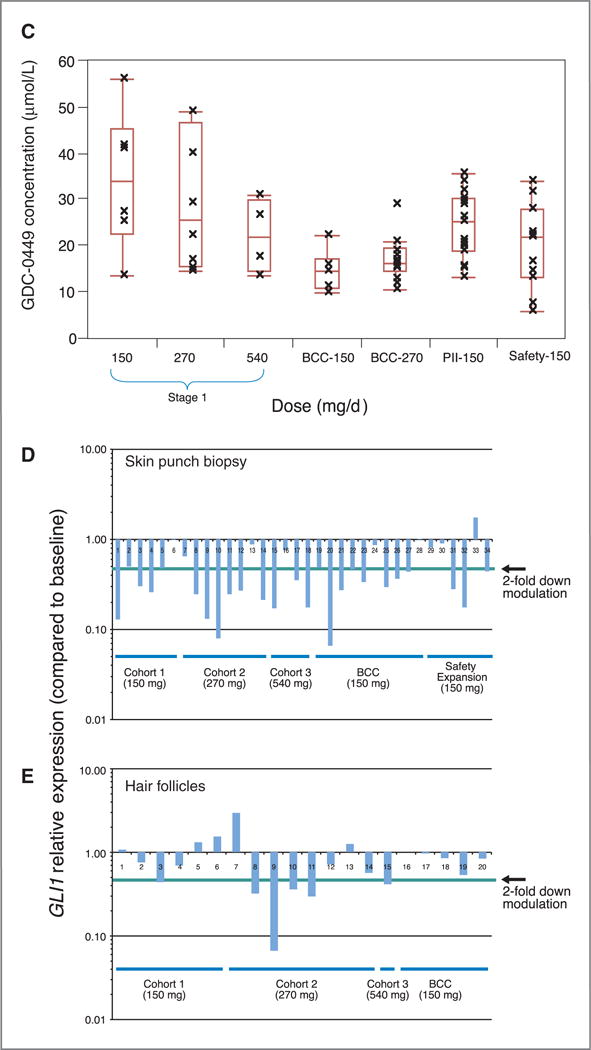
Pharmacokinetics and Pharmacodynamics of GDC-0449. A, steady-state concentrations [Css, mean, and SD] are shown for total and unbound GDC-0449, by dose cohorts. B, Pharmacokinetic plasma concentrations of total GDC-0449 (mmol/L), color-coded by dose cohort, are shown for individual patients over 13 weeks. C, Plots of average GDC-0449 steady state concentrations in the different cohorts. BCC-150 and BCC-270 refer to the cohort of patients with BCC. PII-150 refers to the new GDC-0449 formulation that is being used in phase II studies. The line in the middle of the box represents the median, the top and bottom box limits represent the 25th and 75th percentiles, and the top and bottom bars represent 1.5 times the interquartile range. D and E, Skin punch biopsies or hair follicles were processed for analysis of GLI1 mRNA expression as described in the Methods section. Levels of GLI1 down-modulation, compared with pretreatment patient specimens, are shown for individual patients grouped by dose and staging cohorts.
Pharmacodynamics
Analysis of surrogate tissue (normal skin punch biopsies and hair follicles), on day 7 or 21 after initiation of therapy, showed modulation of GLI1 mRNA expression, compared with GLI1 expression in pretreatment tissue specimens (Fig. 2D and E). Skin biopsy-derived mRNA showed a >2-fold down-modulation of GLI1 expression in 25 of 34 (73.5%) patients, and hair follicle assessment showed >2-fold down-modulation in 6 of 20 patients (30%), compared with pretreatment specimens. A direct quantitative relationship between the magnitude of GLI1 down-modulation and steady state GDC-0449 plasma concentrations was not observed.
Responses to treatment
Sixty-two of the 68 patients enrolled on the study had at least one follow-up tumor assessment and were evaluable for response (Table 4). Responses were only observed in patients with advanced BCC or medulloblastoma, as previously reported (17, 18). The overall response rate (complete and partial responses) in advanced BCC was 19 of 33 (58%). Since the prior report (17), one additional BCC patient has achieved a partial response, and a formerly unconfirmed RECIST partial response has now been confirmed. At the time of study closure, 12 of the 33 advanced BCC patients had been on study for durations of 8.5 to 26.5 months and were then enrolled on an extension study in which they continued to receive GDC-0449. As of 26 January 2010, the median duration of response for patients with advanced BCC was 12.8 months (range, 3.7–26.4 months and ongoing).
Table 4.
Best responses by tumor type
| BCC (n = 33) | Medulloblastoma (n = 1) | Other solid tumors (n = 34) | |
|---|---|---|---|
| Complete response | 2a | 0 | 0 |
| Partial response | 17a | 1b | 0 |
| Stable disease | 10a | 0 | 4 |
| Progressive disease | 4 | 0 | 24 |
| Missingc | 0 | 0 | 6c |
Both complete responses were assessed clinically; 8 partial responses were assessed clinically, 8 by RECIST, and 1 by both clinical and RECIST.
Unconfirmed RECIST partial response.
Patients who experienced clinical progression or withdrew from study before tumor assessments could be performed.
Four patients with other solid tumors experienced stable disease as the best response on study; two had adenocystic carcinoma (durations on study, 3.1 and 5.9 months), one had pancreatic carcinoma (2.8 months on study), and one had metastatic carcinoid (6.5 months on study). The median time on study was 1.4 months for patients with other solid tumors.
Discussion
GDC-0449 was generally well-tolerated in this phase I trial, with an acceptable safety profile. Seven grade 4 adverse events were reported in 6 patients (8.8%). A recommended phase II dose of 150 mg/d was established based on pharmacokinetic properties (no further increase in steady state plasma concentrations with increasing dose), rather than an MTD. There was consistent systemic bioavailability of GDC-0449 at the lowest dose tested (150 mg), with evidence of pathway suppression in surrogate tissues. The nonlinear pharmacokinetic characteristics likely resulted from binding to plasma alpha-1-acid glycoprotein, solubility-limited absorption in the intestine, and a low rate of metabolism, as described in the companion article in this issue of Clinical Cancer Research by Graham and colleagues (24). Studies are ongoing to further characterize these pharmacokinetic properties.
Clinical activity was observed only in advanced BCC (19 out of 33 patients had a response; ref. 17) and in a patient with medulloblastoma (18), consistent with the existence of Hh pathway mutations in these cancer types (1, 2, 4).
For the other solid tumor types studied, mutations or alterations in Hh pathway signaling have not been shown, but overproduction of Hh ligand can activate the Hh pathway in the tumor stroma (5–7), resulting in increased tumor growth (see Fig. 1A). It is perhaps not surprising that tumor shrinkage was not observed in cancers for which type III Hh signaling has been postulated (Fig. 1A, panel 2), such as ovarian, colorectal, and pancreatic cancer. Type III paracrine signaling consists of tumor cell-derived Hh ligand stimulation of stromal cells and resultant activity of stromal-derived factors on tumor cells. In general, patients enrolled in this study had extensively pretreated highly refractory, bulky disease, for which the interplay between Hh pathway factors in stromal and tumor cells is less likely to play a key role, compared with less advanced disease states.
For certain solid tumor types, the combination of GDC-0449 with established chemotherapy regimens is currently being explored in several ongoing or planned clinical trials. A recent preclinical study showed that treatment with a Hh pathway inhibitor transiently improved responsiveness to gemcitabine in a mouse model of pancreatic adenocarcinoma (25).
Pharmacodynamic down-modulation of GLI1 expression was observed in many treated patients, strongly suggesting GDC-0449 inhibition of SMO activity in vivo. In addition, resistance to GDC-0449 mediated by mutation in SMO has been observed in a single patient with medulloblastoma (26), strongly confirming a SMO-targeted mechanism-of-action in vivo. It is unknown whether SMO or other pathway mutations could be a general mechanism of resistance in patients with Type I, II, and/or III tumors; this is an area for further study.
GDC-0449 was generally well-tolerated in this phase I study. A case of pancreatic carcinoma was newly diagnosed during study treatment in a patient with metastatic BCC who had a previous history of three other types of cancer. To date, pancreatic carcinoma has not been reported as an adverse event in other clinical studies of GDC-0449; patients enrolled in clinical studies of GDC-0449 continue to be monitored for this and other adverse events. Given the key role of the Hh signaling pathway in embryo-fetal development, inhibitors of this pathway are anticipated to be teratogenic. For this reason, strict pregnancy prevention measures are in place in all clinical studies. In addition, skeletal growth complications, including effects on both cartilage and bone formation, may limit the use of these therapies in young children (27).
The results from the full cohort of this phase I trial suggest that GDC-0449 is worthy of further study for the treatment of many cancer types. Several phase II studies of GDC-0449, as a single agent or in combination with chemotherapies and/or targeted therapies, are underway.
Translational Relevance.
The Hedgehog (Hh) signaling pathway is a key regulator of cell growth and differentiation during development. In this phase I study of the first-in-class Hh pathway inhibitor vismodegib (GDC-0449), encouraging evidence of clinical benefit was observed in patients with advanced basal cell carcinoma and medulloblastoma, cancers associated with Hh pathway mutations. The overall response rate in 33 patients with advanced BCC was 58% and the duration of response was 12.8 months and ongoing. A partial response of short duration was observed in one patient with metastatic medulloblastoma. No tumor responses were observed among 34 patients with other types of cancer. GDC-0449 was generally well-tolerated. These results represent proof of concept for Hh pathway inhibition as a therapeutic strategy in tumors driven by Hh pathway mutations, and enable the continued development of GDC-0449 as an anti-cancer agent.
Acknowledgments
The authors thank the patients, their families, and the clinical teams who participated in this study. We express our thanks to Drs. Robert L. Yauch, Howard M. Mackey, Bertram L. Lum, James C. Marsters Jr., and Frederic J. de Sauvage at Genentech, Inc.; and all the other investigators and health care practitioners who participated. Genentech, Inc., provided assistance with preparation of the manuscript.
P. LoRusso received research funding from Genentech, is on Genentech’s speakers bureau (compensated) and has participated in Genentech Advisory Boards (compensated); C. Rudin has been a paid consultant to Genentech (not on projects related to Hedgehog inhibitors); G. Weiss is an investigator on hedgehog pathway inhibitor studies for Genentech and Infinity; D. Von Hoff received a grant to his institution for the phase I trial of GDC-0449; J. Reddy, I. Chang, W. Darbonne,, R. Graham, K. Zerivitz, and J. Low are employees of Genentech, a member of the Roche Group, and shareholders of Roche.
Footnotes
Note: Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/).
Disclosure of Potential Conflicts of Interest
The other authors report no conflicts of interest.
References
- 1.Johnson RL, Rothman AL, XIe J, Goodrich LV, Bare JW, Bonifas JM, et al. Human homolog of patched, a candidate gene for the basal cell nevus syndrome. Science. 1996;272:1668–71. doi: 10.1126/science.272.5268.1668. [DOI] [PubMed] [Google Scholar]
- 2.Hahn H, Wicking C, Zaphiropoulous PG, Gailani MR, Shanley S, Chidambaram A, et al. Mutations of the human homolog of Drosophila patched in the nevoid basal cell carcinoma syndrome. Cell. 1996;85:841–51. doi: 10.1016/s0092-8674(00)81268-4. [DOI] [PubMed] [Google Scholar]
- 3.Epstein EH. Basal cell carcinomas: attack of the hedgehog. Nat Rev Cancer. 2008;8:743–54. doi: 10.1038/nrc2503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Raffel C, Jenkins RB, Frederick L, Hebrink D, Alderete B, Fults DW, et al. Sporadic medulloblastomas contain PTCH mutations. Cancer Res. 1997;57:842–45. [PubMed] [Google Scholar]
- 5.Yauch RL, Gould SE, Scales SJ, Tang T, Tian H, Ahn CP, et al. A paracrine requirement for hedgehog signalling in cancer. Nature. 2008;455:406–10. doi: 10.1038/nature07275. [DOI] [PubMed] [Google Scholar]
- 6.Fan L, Pepicelli CV, Dibble CC, Catbagan W, Zarycki JL, Laciak R, et al. Hedgehog signaling promotes prostate xenograft tumor growth. Endocrinology. 2004;145:3961–70. doi: 10.1210/en.2004-0079. [DOI] [PubMed] [Google Scholar]
- 7.Dierks C, Grbic J, Zirlik K, Beigi R, Englund NP, Guo GR, et al. Essential role of stromally induced hedgehog signaling in B-cell malignancies. Nat Med. 2007;13:944–51. doi: 10.1038/nm1614. [DOI] [PubMed] [Google Scholar]
- 8.Scales SJ, de Sauvage FJ. Mechanisms of hedgehog pathway activation in cancer and implications for therapy. Trends Pharmacol Sci. 2009;30:303–12. doi: 10.1016/j.tips.2009.03.007. [DOI] [PubMed] [Google Scholar]
- 9.Ingham PW, McMahon AP. Hedgehog signaling in animal development: paradigms and principles. Genes Dev. 2001;15:3059–87. doi: 10.1101/gad.938601. [DOI] [PubMed] [Google Scholar]
- 10.Rubin LL, de Sauvage FJ. Targeting the hedgehog pathway in cancer. Nat Rev Drug Discov. 2006;5:1026–33. doi: 10.1038/nrd2086. [DOI] [PubMed] [Google Scholar]
- 11.Johnson RL, Rothman AL, Xie J, Goodrich LV, Bare JW, Bonifas JM, et al. Human homolog of patched, a candidate gene for the basal cell nevus syndrome. Science. 1996;272:1668–71. doi: 10.1126/science.272.5268.1668. [DOI] [PubMed] [Google Scholar]
- 12.Xie J, Murone M, Luoh SM, Ryan A, Gu Q, Zhang C, et al. Activating smoothened mutations in sporadic basal-cell carcinoma. Nature. 1998;391:90–2. doi: 10.1038/34201. [DOI] [PubMed] [Google Scholar]
- 13.Cowan R, Hoban P, Kelsey A, Birch JM, Gattamaneni R, Evans DG, et al. The gene for the naevoid basal cell carcinoma syndrome acts as a tumour-suppressor gene in medulloblastoma. Br J Cancer. 1997;76:141–5. doi: 10.1038/bjc.1997.354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Dierks C, Beigi R, Guo GR, Zirlik K, Stegert MR, Manley P, et al. Expansion of Bcr-Abl-positive leukemic stem cells is dependent on Hedgehog pathway activation. Cancer Cell. 2008;14:238–49. doi: 10.1016/j.ccr.2008.08.003. [DOI] [PubMed] [Google Scholar]
- 15.Zhao C, Chen A, Jamieson CH, Fereshteh M, Abrahamsson A, Blum J, et al. Hedgehog signalling is essential for maintenance of cancer stem cells in myeloid leukaemia. Nature. 2009;458:776–9. doi: 10.1038/nature07737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Williams JA. Hedgehog signaling pathway as a target for therapeutic intervention in basal cell carcinoma. Drug News Perspect. 2003;16:657–662. doi: 10.1358/dnp.2003.16.10.829296. [DOI] [PubMed] [Google Scholar]
- 17.Von Hoff DD, LoRusso PM, Rudin CM, Reddy JC, Yauch RL, Tibes R, et al. Inhibition of the hedgehog pathway in advanced basal-cell carcinoma. N Engl J Med. 2009;361:1164–72. doi: 10.1056/NEJMoa0905360. [DOI] [PubMed] [Google Scholar]
- 18.Rudin CM, Hann CL, Laterra J, Yauch RL, Callahan CA, Fu L, et al. Treatment of medulloblastoma with hedgehog pathway inhibitor GDC-0449. N Engl J Med. 2009;361:1173–78. doi: 10.1056/NEJMoa0902903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Binns A, James LF, Shupe JL, Everett G. Congenital cyclopian-type malformation in lambs induced by maternal ingestion of a range plant, Veratrum californicum. Am J Vet Res. 1963;24:1164–75. [PubMed] [Google Scholar]
- 20.Chen JK, Taipale J, Cooper MK, Beachy PA. Inhibition of hedgehog signaling by direct binding of cyclopamine to smoothened. Genes Dev. 2002;16:2743–48. doi: 10.1101/gad.1025302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Robarge KD, Brunton SA, Castanedo GM, Cui Y, Dina MS, Goldsmith R, et al. GDC-0449-a potent inhibitor of the hedgehog pathway. Bioorg Med Chem Lett. 2009;19:5576–81. doi: 10.1016/j.bmcl.2009.08.049. [DOI] [PubMed] [Google Scholar]
- 22.Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92:205–16. doi: 10.1093/jnci/92.3.205. [DOI] [PubMed] [Google Scholar]
- 23.Ding X, Chou B, Graham RA, Cheeti S, Percey S, Matassa LC, et al. Determination of GDC-0449, a small molecule inhibitor of the Hedgehog signaling pathway, in human plasma by solid phase extraction-liquid chromatographic-tandem mass spectrometry. J Chromatogr B Analyt Technol Biomed Life Sci. 2010;878:785–90. doi: 10.1016/j.jchromb.2010.01.039. [DOI] [PubMed] [Google Scholar]
- 24.Graham RA, Lum BL, Cheet S, Jin JY, Jorga K, Von Hoff DD, et al. Pharmacokinetics of hedgehog pathway Inhibitor vismodegib (GDC-0449) in patients with locally advanced or metastatic solid tumors: the role of alpha-1-acid glycoprotein binding. Clin Can Res. 2011;17:2512–20. doi: 10.1158/1078-0432.CCR-10-2736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Olive KP, Jacobetz MA, Davidson CJ, Gopinathan A, McIntyre D, Honess D, et al. Inhibition of hedgehog signaling enhances delivery of chemotherapy in a mouse model of pancreatic cancer. Science. 2009;324:1457–61. doi: 10.1126/science.1171362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Yauch RL, Dijkgraaf GJ, Alicke B, Januario T, Ahn CP, Holcomb T, et al. Smoothened mutation confers resistance to a hedgehog pathway inhibitor in medulloblastoma. Science. 2009;326:572–4. doi: 10.1126/science.1179386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kimura H, Ng JM, Curran T, et al. Transient inhibition of the hedgehog pathway in young mice causes permanent defects in bone structure. Cancer Cell. 2008;13:249–60. doi: 10.1016/j.ccr.2008.01.027. [DOI] [PubMed] [Google Scholar]