

Abstract
Background:
Laparoscopic appendectomy is a well-described surgical technique. However, concerns still exist regarding whether the closure of the appendiceal stump should be done with a clip, an endoloop, or other techniques. In this study, the effect of stump closure on duration of surgery and complications by endoclips was compared with endoloop in patients under laparoscopic appendectomy. The study was carried out as a prospective randomized clinical trial between 2013 and 2015 in Shariati Hospital of Tehran.
Materials and Methods:
Seventy-six patients under laparoscopic appendectomy were enrolled and randomly assigned to receive either endoclips or endoloop for stump closure. The results in terms of the operating time, length of hospital stay, and the complications were compared and analyzed between two groups. After collecting the essential data by using a checklist and examination of patients, the data were analyzed with SPSS.
Results:
The mean age was 23.13 ± 5.07 years and 44.7% of the patients were male. Moreover, in this study, it was seen that the mean duration of surgery was 23.2 min versus 21.5 min in endoloop and endoclips groups, respectively (P = 0.021). There was no difference between hospital stay among two groups (P > 0.05). Furthermore, the complications were same in two groups (P > 0.05).
Conclusion:
The effect of stump closure with endoloop versus endoclips is not different for complications, but the duration of surgery was shorter in endoclips method. Both methods could be used based on the opinion of the surgeon without expecting a statistically significant difference in the results.
Keywords: Appendectomy, complications, endoclips, endoloop, laparoscopy
INTRODUCTION
Appendicitis is an inflammation of the appendix, that comprises approximately 25% of the surgical emergency admissions and 40% of the total laparotomy emergencies.[1] The standard treatment for acute appendicitis is the surgical removal of the appendix called appendectomy This may be done by an open incision in the abdomen or through laparoscopy.[2] Laparoscopy appendectomy surgeries are increasing daily because of its facilities and advantages such as less postoperative pain, faster recovery, shorter hospital stay, less postoperative complications, and minimally sized incisions/scars.[3,4] The main concern in laparoscopic appendectomy is the matter of closure of the appendiceal stump or base. Therefore, many methods have been recommended and examined for its closure, some of these methods include endoloop, double endoloop, cutting with ultrasonic knife, tying with instrument, metal or plyometric clips, ligator and thread, hemolock, and linear endostapler.[5,6,7] Linear stapler and endoloop are nowadays often used as alternatives for closing appendiceal stump in laparoscopic appendectomy since they are equally safe.[5,6,8] Regarding each of these methods, the matter of being economic must also be considered in addition to the issue of safety.
Endoloop is one of the first methods used in closing appendiceal stump.[9,10] The main problem with this method is that the knot may be loose due to the surgeon being concerned with the thread breaking when it is pulled. This could lead to the appendiceal stump leaking; however, if the clips are used, they will not open after being locked; they may however slip and fall but they are easier to use and they are less expensive.[11,12] We may not have sufficient stump when stapler is used since its diameter is large and it is possible to damage the secum and cause a leak.[13] Many researches have been conducted so far to examine each of these methods; but there are a few studies that have compared these two methods. Therefore, with regard to the importance of this subject, we have compared the two methods of closing the appendiceal stump with endoloop and clips in the present study in terms of the length of operating time, postsurgical complications, and the duration of hospitalization.
MATERIALS AND METHODS
This prospective randomized clinical trial study was conducted on the patients diagnosed with acute appendicitis applying to the emergency ward of Shariati Hospital between March 1, 2013 and May 25, 2015. A total of 76 qualified patients who were clinically diagnosed with acute appendicitis, after obtaining informed consent from all patients, randomly were assigned into two groups with 38 individuals in each groups [Figure 1]. Then, they underwent laparoscopic appendectomy. The exclusion criteria for this research included the following: Patients who were in pain more than 4 days, finding a mass in the right lower quadrant area in the examination, phlegmon in images or peritonitis symptoms also the patients who underwent surgeries which turned into open laparoscopic due to adhesion and improper anatomic conditions were excluded from the study (did not occur in our study). Almost all patients had inflammation of the appendix, it should also be mentioned that all operations were performed by single surgeon.
Figure 1.

Consort flow diagram of trial
Three ports were inserted in both groups, two 10-mm ports and one 5-mm port. The mesoappendix was cut with LigaSure in both groups and the appendiceal stump was closed with endoclips in one group and with endoloop in the other group, and they underwent laparoscopic appendectomy. The surgery duration was calculated from the time the skin was cut until the time it was closed. The patients were then compared regarding the surgery duration, postsurgical symptoms such as pain, wound infection, and leakage from the appendiceal stump, the hospitalization period, and the need for repeating the surgery.
Ethical considerations
The study was conducted after registration in Iranian Registry of Clinical Trials (IRCT) center and approved by the University Ethics Committee. Then, informed consent was obtained from all patients. In all steps of research, medical confidentiality and privacy were respected. Clinical trial registration number is: IRCT201507096925N4.
Statistical analysis
After collecting the essential data using a checklist and examination of patients, the data were analyzed with IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp. The continuous variables are reported as means ± standard deviation, and categorical variables are reported by number and percentage. Normality for continuous variables was determined by the Shapiro–Wilk test, which revealed that the continuous variables showed normal distributions (P > 0.05). The unpaired t-test was used for comparison of variables between groups. For statistical evaluation of categorical variables, we used the Chi-square test and Fisher exact test as appropriate. A P < 0.05 was accepted as statistically significant. The study protocol was either approved by the Institutional Review Board and Medical Ethics Committee of Tehran University of Medical Sciences. The study protocol was also registered with Iranian registry for clinical trials (IRCT201507096925N4; www.irct.ir).
RESULTS
In total, 76 patients underwent laparoscopic appendectomy who were randomly divided into two groups, and none of the patients were excluded from the study during the research. The endoclip group consisted of 38 patients (18 male, 20 female; mean age 22 ± 3.69 years), and the endoloop group consisted of 38 patients (16 male, 22 female; mean age 24.26 ± 5.99 years). Overall, based on the findings of our study, the mean age of the all patients was 23.13 ± 5.07 years and 44.7% of the patients were males. No statistically significant differences were detected between the groups in terms of the distribution of age, sex percentage (P > 0.05). The demographic data of the two groups are displayed in Table 1.
Table 1.
The demographic and clinical outcomes of the two groups (distribution and significance)#
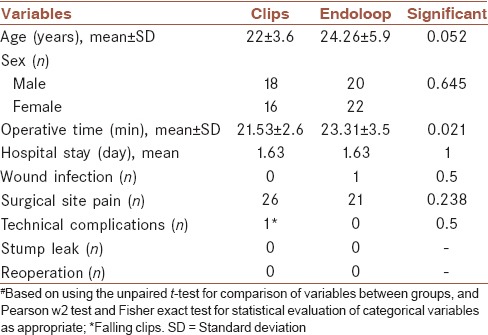
The mean surgery duration was 23.2 min in the endoloop group and 21.5 min in the clips group which indicated a statistically significant difference (P = 0.021). Although this difference value but may not be of much importance clinically. Moreover, the mean hospitalization stay was almost the same in the eldoloop and clips groups (1.63 days), and there was therefore no statistically significant difference between the hospitalization stay of the two groups (P > 0.05). There were no cases of surgical wound infection and postsurgical complications in the group which used clips, but one infection case was reported in the endoloop groups but this difference was not statistically significant. The two under-study groups were not different regarding the technical complications either but one of case in the clips group experienced the clips falling off. However, the comparison between the two groups indicated that the frequency distribution of pain in the surgery site was different in the two groups [Table 1]. About 68% of the patients of the group who had used clips were complaining from pain in the surgery site, but this value was equal to 55% in the endoloop groups (P < 0.023). It is worth mentioning that no cases of stump leak were seen in the two groups and none of the patients are needed to repeat the surgery.
DISCUSSION
Appendiceal stump closure is the most controversial issue in the laparoscopic appendectomy procedure.[11] Despite the fact that many authors have described several modifications with new materials for appendiceal stump closure, an optimal closure material has not yet been determined. Moreover, most of these materials may prolong the operation time or increase cost, which may limit the popularity of laparoscopic appendectomy.[14,15] Recently, linear staplers and endoloops, both equally safe, have frequently been used as an alternative in the closure of the appendiceal stump during laparoscopy.[7] Endoloop is one of the first methods used in closing appendiceal stump. The main problem with this method is that the knot may be loose due to the surgeon being concerned with the thread breaking when it is pulled.[11,12] This could lead to the appendiceal stump leaking; however, if clips are used they will not open after being locked. Many researches have been conducted to examine each of these methods. But yet, has not been leading to the introduction a standard way for stump closure, so it seems that further studies are needed. The results of the present study showed that the mean surgery duration was 23.2 min in the endoloop group and 21.5 min in the endoclips group which indicated a statistically significant difference (P = 0.021). There was no statistically significant difference in the duration of hospitalization between the two groups also the complications in two groups were not statistically significant (P > 0.05). The need to repeat the surgery and leaking was not seen in any of the groups.
In a prospective clinical trial study, 28 patients who were divided into two groups of 14 individuals underwent laparoscopic appendectomy (appendiceal stumps of one group were closed with endoclips and the other through endostapler method). They concluded that the surgery duration was shorter in the endoclips method in comparison with the endostapler method (53.4 min vs. 62.5 min).[15] While in our study, the surgery duration was statistically significantly shorter in the clips method in comparison with the endoloop method although this difference may not be clinically important. However, in another clinical trial on 61 patients, endoclips method was compared with endoloop the findings indicated that the endoclips method was safer and the surgery duration was statistically significantly shorter than the endoloop method (41.27 vs. 62.81).[12] This difference is statistically significant as well as clinically. The safety of the two methods in our study was the same as the abovementioned study.
In an randomized controlled trial (RTC) study conducted in this field, the mean surgery duration was reported to be 53.4 min when closing the appendiceal stump with clips in laparoscopic appendectomy, this period was specifically shorter in our study (21 min)[15] in comparison with the mentioned study with regard to the skillfulness of the surgeon. Moreover, in another prospective randomized trial,[14] the mean operating time was 53.4 min in the endoloop method, which was longer than the periods observed in our study (23 min).
Delibegovic also examined animal samples and demonstrated that using endoloop to close the appendiceal stump is more efficient than using clips[16] in another RTC, 35 patients underwent laparoscopic appendectomy using endoloop and a total of three cases were affected by complications and the mean hospitalization period was also 2 days.[17] The hospitalization period was 1.6 days in our study which is a bit lesser than the mentioned study but no serious complications were seen after or during the surgery, only one case of infection and one case of the clips falling off. Another study examined 242 patients who had undergone laparoscopic appendectomy and indicated that endoloop is efficient and safe, especially in cases where the perforation is highly likely to occur;[18] this method also proved to be safe in our study.
CONCLUSION
Generally, based on the obtained results from present study, we concluded that closing the appendiceal stump with endoloop and clips in patients who undergo laparoscopic appendectomy were not different in terms of postsurgical complications and the length of hospital stay, but the operating time was shorter in the endoclips method. Both methods could be used based on the opinion of the surgeon without expecting a statistically significant difference in the results. However, it is recommended to study this subject with larger samples to obtain more reliable and valid results.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
AUTHORS’ CONTRIBUTION
SASS: contributed in the conception of the work, conducting the study, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work
SHN: contributed in the conception of the work, drafting and revising the draft, approval of the final version of the manuscript
ASH: contributed in the revising of draft, approval of the final version of the manuscript, and agreed for all aspects of the work
MJ: contributed in data analysis, conducting the study, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work
AGA: contributed in the conception of the work, approval of the final version of the manuscript, and agreed for all aspects of the work
AY: contributed in the data collection, approval of the final version of the manuscript, and agreed for all aspects of the work
AYN: contributed in the data collection, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work
ARS: contributed in the conception of the work, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work and data analysis.
Acknowledgments
The authors certify that no other persons have made substantial contributions to this manuscript. The authors gratefully acknowledge the financial support of Shariati Hospital and Tehran University of Medical Sciences.
REFERENCES
- 1.Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132:910–25. doi: 10.1093/oxfordjournals.aje.a115734. [DOI] [PubMed] [Google Scholar]
- 2.Ates M, Sevil S, Bulbul M. Routine use of laparoscopy in patients with clinically doubtful diagnosis of appendicitis. J Laparoendosc Adv Surg Tech A. 2008;18:189–93. doi: 10.1089/lap.2007.0040. [DOI] [PubMed] [Google Scholar]
- 3.Sauerland S, Lefering R, Neugebauer EA. Laparoscopic versus open surgery for suspected appendicitis. Cochrane Database Syst Rev. 2004:CD001546. doi: 10.1002/14651858.CD001546.pub2. doi: 10.1002/14651858.CD001546.pub2. [DOI] [PubMed] [Google Scholar]
- 4.Pedersen AG, Petersen OB, Wara P, Rønning H, Qvist N, Laurberg S. Randomized clinical trial of laparoscopic versus open appendicectomy. Br J Surg. 2001;88:200–5. doi: 10.1046/j.1365-2168.2001.01652.x. [DOI] [PubMed] [Google Scholar]
- 5.Hansen JB, Smithers BM, Schache D, Wall DR, Miller BJ, Menzies BL. Laparoscopic versus open appendectomy: Prospective randomized trial. World J Surg. 1996;20:17–20. doi: 10.1007/s002689900003. [DOI] [PubMed] [Google Scholar]
- 6.Al Hadi HI, Maw A. The “double endoloop” technique – A simple alternative technique for laparoscopic appendectomy. Surg Laparosc Endosc Percutan Tech. 2008;18:67–9. doi: 10.1097/SLE.0b013e318155abd1. [DOI] [PubMed] [Google Scholar]
- 7.Kazemier G, Saad S, Bonjer H, Sauerland S. Securing the appendiceal stump in laparoscopic appendectomy: Evidence for routine stapling? Surg Endosc. 2006;20:1473–6. doi: 10.1007/s00464-005-0525-7. [DOI] [PubMed] [Google Scholar]
- 8.Suttie SA, Seth S, Driver CP, Mahomed AA. Outcome after intra- and extra-corporeal laparoscopic appendectomy techniques. Surg Endosc. 2004;18:1123–5. doi: 10.1007/s00464-003-9135-4. [DOI] [PubMed] [Google Scholar]
- 9.Martín del Olmo JC, Blanco Alvarez JI, Carbajo Caballero MA, de la Cuesta de la Llave C, Vaquero Puerta C, Arenal J. Laparoscopic appendectomy by ultrasonically activated scalpel in acute appendicitis: Preliminary report. J Laparoendosc Adv Surg Tech A. 2002;12:111–3. doi: 10.1089/10926420252939628. [DOI] [PubMed] [Google Scholar]
- 10.Sajid MS, Rimple J, Cheek E, Baig MK. Use of endo-GIA versus endo-loop for securing the appendicular stump in laparoscopic appendicectomy: A systematic review. Surg Laparosc Endosc Percutan Tech. 2009;19:11–5. doi: 10.1097/SLE.0b013e31818a66ab. [DOI] [PubMed] [Google Scholar]
- 11.Beldi G, Vorburger SA, Bruegger LE, Kocher T, Inderbitzin D, Candinas D. Analysis of stapling versus endoloops in appendiceal stump closure. Br J Surg. 2006;93:1390–3. doi: 10.1002/bjs.5474. [DOI] [PubMed] [Google Scholar]
- 12.Ates M, Dirican A, Ince V, Ara C, Isik B, Yilmaz S. Comparison of intracorporeal knot-tying suture (polyglactin) and titanium endoclips in laparoscopic appendiceal stump closure: A prospective randomized study. Surg Laparosc Endosc Percutan Tech. 2012;22:226–31. doi: 10.1097/SLE.0b013e31824f25cd. [DOI] [PubMed] [Google Scholar]
- 13.Partecke LI, Kessler W, von Bernstorff W, Diedrich S, Heidecke CD, Patrzyk M. Laparoscopic appendectomy using a single polymeric clip to close the appendicular stump. Langenbecks Arch Surg. 2010;395:1077–82. doi: 10.1007/s00423-010-0671-9. [DOI] [PubMed] [Google Scholar]
- 14.McAnena OJ, Austin O, O'Connell PR, Hederman WP, Gorey TF, Fitzpatrick J. Laparoscopic versus open appendicectomy: A prospective evaluation. Br J Surg. 1992;79:818–20. doi: 10.1002/bjs.1800790837. [DOI] [PubMed] [Google Scholar]
- 15.Hanssen A, Plotnikov S, Dubois R. Laparoscopic appendectomy using a polymeric clip to close the appendicular stump. JSLS. 2007;11:59–62. [PMC free article] [PubMed] [Google Scholar]
- 16.Delibegovic S, Iljazovic E, Katica M, Koluh A. Tissue reaction to absorbable endoloop, nonabsorbable titanium staples, and polymer Hem-o-lok clip after laparoscopic appendectomy. JSLS. 2011;15:70–6. doi: 10.4293/108680811X13022985131336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Caglià P, Tracia A, Spataro D, Borzì L, Lucifora B, Tracia L, et al. Appendix stump closure with endoloop in laparoscopic appendectomy. Ann Ital Chir. 2014;85:606–9. [PubMed] [Google Scholar]
- 18.Arash S, Langer M, Skarsgard ED. Endoloop versus endostapler closure of the appendiceal stump in pediatric laparoscopic appendectomy. Can J Surg. 2012;55:37–40. doi: 10.1503/cjs.023810. [DOI] [PMC free article] [PubMed] [Google Scholar]