

Abstract
Introduction:
Osteochondroma or exostosis is most common primary benign bony tumor comprising of more than one third of the total occurrences. Osteochondromas are considered as an aberration in the normal physial growth plate and originate from the metaphysis of long bone with more than third (35-46%) of cases affecting the bone around the knee (lower end femur> upper end tibia), 10% cases involve the small bones of the hand and 5% involve the pelvis and flat bones like scapula (4-6%) are least involved. These tumors usually affect the growing skeleton and cease to increase in size after skeletal maturity. These are usually painless but may become painful due to neurovascular entrapment/compression, fracture at the stalk, bursal inflammation or malignant transformation.
Case Presentation :
This article presents a case of osteochondroma on superior angle of scapula in a 23-year-old male presented with pseudo winging and snapping of scapula, crepitus on scapulothoracic motion and occasional pain since 5 years. However, there was no increase in size of the swelling or local and systemic signs of malignant transformation. X-ray demonstrated a pedunculated exophytic mass on supero medial aspect of the right scapula. The findings were confirmed on CT and excision of the lesion was done. The patient demonstrated full painless range of motion after 1 month and no recurrence was demonstrated during 1 year follow up.
Conclusion:
Scapular osteochondroma is a relatively rare condition. Usually a patient presents in early to late childhood, however, in some cases it may be presented in adults. Growth after maturity is indicative of a metastatic transformation. So an excision of the same should be accompanied with histopathological examinations.
Keywords: Scapular exostosis, delayed presentation osteochondroma, pseudowinging scapula
What to Learn from this Article?
Scapular osteochondroma is a relatively rare condition. Usually a patient presents in early to late childhood however in some cases it may be presented in adults. Growth after maturity is indicative of a metastatic transformation. So an excision of the same should be accompanied with Histopathological examinations.
Introduction
Osteochondroma is the most common primary benign bone tumor that most of tenoccursnear the end of long bone usually solitary (90%), may be multiple in the form of hereditary multiple exostosis (HME) in about 10% of cases [1]. This tumor rarely involves flat bones like scapula [2]. However, this is the most common benign primary bone tumor affecting scapula. A scapular osteochondroma may be symptomatic mainly due to its mass effect as it may cause scapular pseudo winging and crepitus and snapping on scapulothoracic motion [3]. Winging of scapula is defined as prominence of medial border or vertebral border of scapula [3, 4]. It can be attributed to many causes but most commonly due to paralysis of serratus anterior muscle which needs to be ruled out. These tumors usually affect the growing skeleton and cease to increase in size after skeletal maturity. Any increase in swelling of an asymptomatic swelling turning symptomatic should raise the suspicion of amalignancy. Herein, we describe a case of a 23-year-old patient who presented with a swelling on superomedial aspect of right scapula since 5 years. Diagnostic work up and management along with clinical pictures are included in the case report.
Case Presentation
A 23 year old male patient presented to the orthopaedic clinic with complaints of an isolated scapular swelling (right) since 5 years (Figure 1). The swelling was also associated with crepitus and snapping of the right shoulder and slight restriction and pain on abduction. The patient reported no increase in size of the swelling over the years and demonstrated no increase in symptoms as well. There was no history of antecedent trauma, weight loss, loss of appetite or any other constitutional symptom. The patient wanted the swelling to be removed due to cosmetic reasons mainly as he was about to get married. Local examination of the swelling revealed increased prominence of superior angle of scapula. The skin overlying the same was normal. There were no signs of inflammation etc present. The swelling was non painful on touch. However, snapping and crepitus/grating could be demonstrated on scapulothoracic movements and restriction in abduction was evident. An antero posterior skiagram of the right shoulder revealed a pedunculated mass arising from the supero medial angle of the scapula (Figure 2).
Figure 1.

showing swelling over medial border of Rt. Scapula
Figure 2.
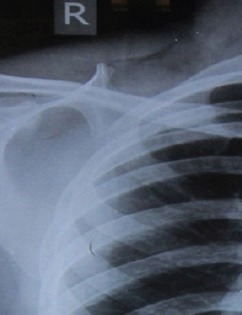
shows the anteroposterior view of right shoulder with an exostosis arising from the superior angle of scapula
CT scan and MRI revealed a mushroom shaped exostosis over the superior angle of scapula (Figure 3).
Figure 3.
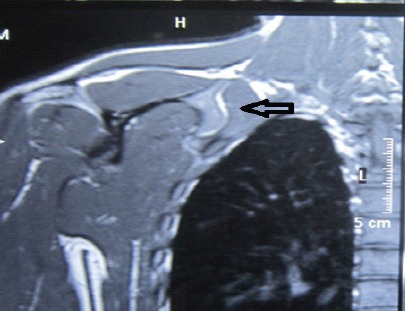
shows the anteroposterior view of right shoulder with an exostosis arising from the superior angle of scapula
The swelling diagnosed as ventral osteochondroma was excised. A laparoscopic resection of the same has been described, however, we performed an open excision of the swelling.
An incision was used along the medial border of scapula wherein it was most prominent (Figure 4).
Extra periosteal resection of the swelling was performed and sent for biopsy. HPE analysis confirmed our diagnosis and ruled out any malignant transformation. Post operative course was uneventful and patient was able to perform full range of motion at his right shoulder after 1 month (Figures 5,6). Follow up was done till 1 year and no recurrence of the swelling was reported.
Discussion
Osteochondroma is the most common benign tumor affecting the metaphysis of long bones, rarely involving the flat bones like scapula [1]. However, it is the most common benign tumor affecting the scapula. Usually the swelling is painless, however, symptoms may be detected when the swelling becomes large in size due to sheer bulk of the same. Symptoms are usually attributed to neurovascular compression, bursal thickening, fracture through the stalk and rarely malignancy. However in case of scapula, symptoms may include snapping, grating / crepitus on scapulothoracic movements [2, 3, 4] and on and off pain etc may be present. Ventral swellings may cause most of these symptoms and may also lead to untoward prominence of medial border which remains so even on pushing against a wall, hence called pseudowinging as opposed to winging which increases on performing this maneuver. Snapping occurs when the normal smooth gliding of the concave portion of the anterior scapula over the convex thorax is disrupted. Scapulo thoracic crepitus may also be produced by an abnormal shape of the scapula which interferes with scapulo-thoracic motion as can be expected in ventral swellings. Sometimes ventral swellings may impinge on thoracic cage and restrict abduction which is again a feature of such swellings.
Conclusion
Usually this condition is benign however, growth in size after skeletal maturity, asymptomatic swelling turning symptomatic and other constitutional and local symptoms/signs may raise the suspicion of malignancy and other radiographic assessment modules need to relied upon like an MRI or a CT scan which will clearly demonstrate the margins and cartilage cap thickness (> 2cm signifies malignancy, <1 cm benign and 1-2 cm questionable). In our case, the patient with scapular swelling demonstrated no increase in size or other features of malignancy. But we still opted for radiological assessment as it helped both in the surgical approach as well as ruled out any malignant transformation and hence malignancy. It is mandatory to get a biopsy for HPE analysis no matter how benign the swelling appears to rule out any traces of malignancy. Open surgical excision is a safe and definitive procedure. However, proponents of arthroscopic excision claim that there is slow functional recovery and cosmetic disadvantage due to the larger incision. Many authors have advocated arthroscopic excision for ventral mass, however it has risks of incomplete removal and recurrence.
Clinical Message.
Scapular osteochondroma is a relatively rare condition. Usually a patient presents in early to late childhood however in some cases it may be presented in adults. Growth after maturity is indicative of a metastatic transformation. So an excision of the same should be accompanied with Histopathological examinations.
Biography

Footnotes
Conflict of Interest: Nil
Source of Support: None
References
- 1.Edelman RR, Hesselink JR, Zlatkin MB. Clinical magnetic resonance imaging. Philadelphia: Saunders Elsevier; 2006. [Google Scholar]
- 2.Tomo H, Ito Y, Aono M, et al. Chest wall deformity associated with osteochondroma of the scapula:a case report and review of the literature. J Shoulder Elbow Surg. 2005;14:103–6. doi: 10.1016/j.jse.2004.03.007. [DOI] [PubMed] [Google Scholar]
- 3.Lazar MA, Kwon YW, Rokito AS. Snapping scapula syndrome. J Bone Joint Surg. 2009;91A(9):2251–2262. doi: 10.2106/JBJS.H.01347. [DOI] [PubMed] [Google Scholar]
- 4.Okada K, Terada K, Sashi R, et al. Largebursa formation associated with osteochondroma of the scapula:a case reporight and review of the literature. Jpn J ClinOncol. 1999;29(7):256–260. doi: 10.1093/jjco/29.7.356. [DOI] [PubMed] [Google Scholar]
- 5.Kumar N, Ramakrishnan V, Johnson GV, Southern S. Endoscopicallyassisted excision of scapular osteochondroma. ActaOrighthopScand. 1999;70:394–396. doi: 10.3109/17453679908997832. [DOI] [PubMed] [Google Scholar]
- 6.Fukunaga S, Futani H, Yoshiya S. Endoscopically assisted resection of a scapular osteochondroma causing snapping scapula syndrome. World J SurgOncol. 2007;5:37. doi: 10.1186/1477-7819-5-37. [DOI] [PMC free article] [PubMed] [Google Scholar]