

Abstract
Introduction:
Non-or partial weight bearing is frequently the standard treatment after peri-articular lower extremity fractures. Displaced talar neck fractures are severe injuries compromising vascularity of the corpus and consequently are at risk for non-union and avascular necrosis, the main reason to restrict weight bearing for up to three months according to most literature.
Case presentation:
We report a case of a 31-year old male with a high impact car accident. His pelvic ring and Hawkins II talar fracture were treated by open reduction and internal fixation. Rehabilitation was based on permissive weight bearing following wound healing. His fractures healed uneventfully and he was able to run freely, without any discomfort within 8 weeks. Radiological evaluation of the talus showed complete bone healing without signs of avascular necrosis. At one year follow-up, the patient is free of the symptoms.
Conclusion:
We might consider changing the restricted or non-weight bearing protocol in surgically treated talar neck fractures at our centre and allow early weight bearing, based on body awareness and the creation of a safe environment during the rehabilitation phase.
Keywords: talar fracture, talar neck fracture, displaced talar neck fracture, trauma
What to Learn from this Article?
Early mobilization guided by body awareness may be accelerate recovery and lower the risk of avascular necrosis after ORIF surgery in a patient with a talus fracture.
Introduction
There is currently no consensus among surgeons worldwide with regard to early versus late weight bearing in fractures of the lower extremities. As an example displaced talar neck fractures requiring open reduction, internal fixation (ORIF) are usually rehabilitated with 10-15 kg (partial) weight bearing for at least 2-3 months after surgery [1].
Although talus fractures comprise approximately 0.1 to 0.85 % of all fractures [1], disturbed fracture healing frequently results in significant loss of motion and function. The incidence of avascular necrosis in surgically treated talar neck fractures is according to a recent systematic review up to 33% [4]. Early weight bearing after surgery in case of cartilage damage of the talus has been found to be beneficial on pain relief and ankle-hind-foot mobility [6, 7]. We hypothesize that it might also lower the risk of avascular necrosis through increased revascularization.
In this case report, we present a patient with a Hawkins II talus fracture treated by open reduction and early mobilization, leading to remarkable quick clinical improvement.
Case Presentation
A 31-year-old patient who had a high impact trauma (car against a tree)was diagnosed with a pelvic ring fracture, a Hawkins II talar neck fracture of the right foot (Fig. 1) and a MTP [2, 3, 4] fracture of the left foot. Assessment by Advanced Trauma Life Support survey showed no additional injuries. There was no distal neurovascular deficit and no evidence of compartment syndrome. The talus fracture was initially treated by casting (8 days), followed by an open reduction (bilateral approach) and internal fixation (ORIF) by plate and screw osteosynthesis and cannulated screws (Fig. 2).
Figure 1.

Initial injury radiograph. Lateral view
Figure 2.

Lateral view postreduction demonstrating a Hawkins 2 talar fracture.
Figure 3.
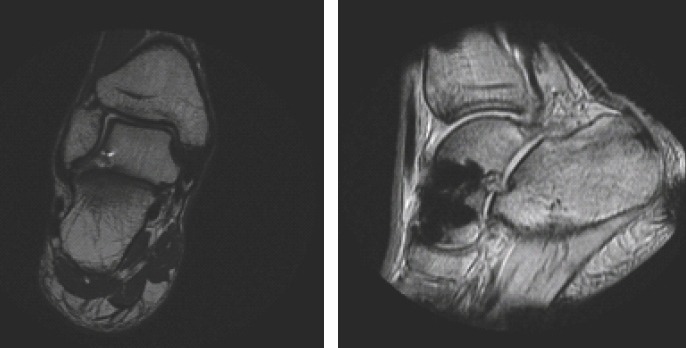
MRI follow up after one year (T1w). Hypo intense region corresponding to artefacts due to osteosynthesis material.
After 10 days of hospitalization, the patient was signed up for intensive rehabilitation at a specialized unit. Rehabilitation comprised of early weight bearing, based on body awareness technique, mobilizing according to pain, and hydrotherapy. The recovery was surprisingly fast and within 7 weeks postoperatively, the patient could mobilize completely unaided and was even able to run (see video).
At one year follow-up, patient did not experience any pain or functional disabilities. Follow-up X-ray did not demonstrate any mechanical failure and an MRI scan one year after surgery showed complete bone healing without signs of avascular necrosis.
Discussion
Several biomechanical and human studies demonstrate that early weight bearing in talus fractures is beneficial on osteogenic healing, new vessel formation [5] and on pain relief and ankle-hind foot mobility [6, 7, 8]. However, talus fracture protocols in the Netherlands as well as most countries worldwide prescribe a non-weight bearing short-leg cast for six weeks with maximum weight bearing allowance of 10-15 kg, followed by gradual weight-bearing in a cast boot for two to four weeks, and finally a gradual return to full weight bearing after 3 months [1]. The question one is faced with is if nonweight bearing enhances bone healing and/or revascularization of the subchondral bone and thereby improved cartilage recovery or might be even detrimental [2].
This case is an interesting and unique illustration that early mobilization guided by body awareness may be beneficial not only on pain relief and increased mobility but also accelerates recovery and lower the risk of avascular necrosis after ORIF surgery patients with a talus fracture. Important is to mention that this is an observation and certainly no policy recommendation until further evidence is provided to support this case.
Conclusion
In an aftercare treatment scheme, both over and under-loading may lead to prolonged and complicated recovery. Patients with surgically treated talar neck fractures might benefit from an early weight bearing protocol, based on body awareness and the creation of a safe environment during the rehabilitation phase.
Clinical Message.
High-quality studies comparing weight-bearing protocols after talar neck fractures are not readily available. The exact timing and subgroups of patients that might benefit from early weight bearing therefore needs further clarification.
Biography




Footnotes
Conflict of Interest: Nil
Source of Support: None
References
- 1.Hak DJ, Lin S. ‘Management of talar neck fractures’. Orthopedics. 2011;32:9–721. doi: 10.3928/01477447-20110714-16. [DOI] [PubMed] [Google Scholar]
- 2.Kuner EH, Lindenmaier HL, Munst P. Talus fractures. In: Tscherne H, Schatzker J, editors. Major fractures of the pilon, the talus, and the calcaneus:current concepts of treatment. Berlin: Springer; 1993. pp. 71–85. [Google Scholar]
- 3.Rammelt S, Zwipp H. ‘Talar neck and body fractures’. Injury. 2009;40(2):120–135. doi: 10.1016/j.injury.2008.01.021. [DOI] [PubMed] [Google Scholar]
- 4.Halvorson JJ, Winter SB, Teasdall RD. ‘Talar Neck Fractures:A Systematic Review of the Literature’. The Journal of Foot and Ankle Surgery. 2013;52(1):56–61. doi: 10.1053/j.jfas.2012.10.008. [DOI] [PubMed] [Google Scholar]
- 5.Moore DC, Leblanc CW, Muller R. ‘Physiologic weight-bearing increases new vessel formation during distraction osteogenesis:a microtomographic imaging study’. Journal of Orthopaedic Research. 2003;21:489–496. doi: 10.1016/S0736-0266(02)00234-6. [DOI] [PubMed] [Google Scholar]
- 6.Cala M, Barreiro K, Jeffry H. ‘Early mobilization in bilateral talar fractures’. The Foot and Ankle OnlineJournal. 2014;7(2):9. [Google Scholar]
- 7.Dong-Hyun Lee, Keun-Bae Lee, Sung-Taek Jung. ‘Comparison ofEarly Versus Delayed Weight bearing Outcomes After Microfracture for Small to Midsized Osteochondral Lesions of the Talus’. Am J Sports Med. 2012;40:2023–2028. doi: 10.1177/0363546512455316. [DOI] [PubMed] [Google Scholar]
- 8.Lasanianos NG, Lyras DN, Mouzopoulos G, et al. ‘Early mobilization after uncomplicated medial subtalar dislocation provides successful functional results’. J Orthop Traumatol. 2011;12(1):37–43. doi: 10.1007/s10195-011-0126-2. [DOI] [PMC free article] [PubMed] [Google Scholar]