

Abstract
Introduction:
Femur fractures as a result of birth trauma can still occur during the C/S, in spite of recent developments of surgical and anesthetic techniques. In this study, we aimed to present a rare case of a newborn with myelomeningocele who delivered by cesarean section due to breech presentation and sustained bilateral fracture of femoral shaft.
Case Presentation:
A 2690 g female newborn with myelomeningocele sustained bilateral femoral shaft fractures during cesarean section. Complete healing was obtained without sequelae after 21 days ofimmobilization with long leg splints.
Conclusion:
Despite the development of early diagnosis and treatment modalities, there is a probability of significant birth traumas. The C/S with accurate technique and gentle obstetrical maneuvers is seemed to be the most important factor for preventing such incidents and considerable complications during abnormal delivery.
Keywords: newborn, femur fracture, myelomeningocele
What to Learn from this Article?
Clinicans should be aware of poor bone quality during labor in a newborn with neurological disorders, in order to prevent undesirable complications.
Introduction
Cesarean section (C/S) is a common and safe procedure for the delivery of fetuses with breech presentation. This procedure prevents trauma and decreases the risk of head entrapment, however femur fractures as a result of birth trauma can still occur during the C/S [1,2]. Alexander et al. reported 0.02% of long bone fracture and 1.1% fetal injury at cesarean section. Moreover, it is reported that the incidence offemur fracture [3] would increase during C/S in the fetus with risk factors such as low-birth weight, macrosomia and neuromuscular disorders [4], thus requiring more attention during labor. Here, we report a newborn with myelomeningocele who was delivered by cesarean section for breech presentation and sustained bilateral fracture of femoral shaft.
Case Presentation
A healthy 18-year-old woman and thirty-nine-week pregnant woman suffered sudden onset of severe pain and was admitted to the obstetrics clinic. Myelomeningocele and breech presentation was previously diagnosed in fetus. In the ultrasonographic (USG) examination; fetal stress and hydrocephaly were determined and urgent cesarean was planned. A 2690 g. female baby was delivered with Apgar scores between seven to eight at an hour and five minutes. Swelling was determined on both her thighs in routine neonatal evaluation few minutes after the delivery. The neonate seemed irritated with the palpation of thighs. She was consulted to our department immediately. Antero-posterior and lateral radiographs of each femur were taken which revealed displaced femur shaft fractures on both sides (Fig.1). At first a pelvipedal cast was thought, however to avoid the lesion irritation on the lumbar skin, long leg splints were performed on both lower limbs for three weeks. The fractures healed uneventfully after three weeks (Fig. 2). The follow-ups were continued at obstetric clinic during hospitalization. Myelomeningocele was repaired by plastic surgeons and neuro-surgeons ten days after her discharge from obstetric department.
Figure 1.
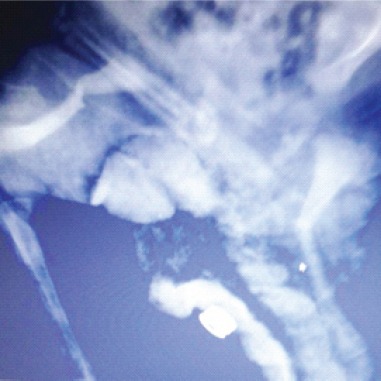
Radiograph of the thighs revealed bilateral shaft fracture of the femur.
Figure 2.
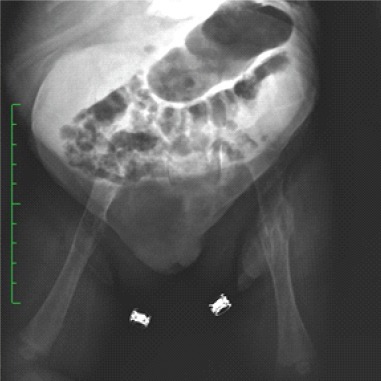
Good callus formation after three weeks.
Discussion
The risk ofbirth traumas increases at abnormal deliveries and presentations such as breech and prolonged delivery, forceps application, multiple pregnancy and preterm labor. Breech presentation is one of the most common risk factor of perinatal mortality and morbidity, accounts for 3-4% of the deliveries [5]. Additionally, fetal anomalies increase the incidence of injuries significantly.. Most of them can be managed with simple interventions, however, on rare occasions, they can be serious and life threatening [3].
Recently, obstetricians take precautions against undesirable complications. The risk of mortality and morbidity has been significantly reduced with C/S performed by accurate techniques and gentle obstetrical maneuvers [6]. Giampiero et al. defined some rules to prevent this complication as; adequate analgesia, extraction by exercising gentle traction, sufficiently wide incision of skin and uterus to allow for a smooth extraction [7]. Nevertheless, the birth trauma risks have been ongoing especially in deliveries with fetal anomalies despite these prevention efforts. The increasing incidence of the fracture due to birth trauma is considered as fetal osteoporosis due to neuromuscular disorder.
Femur fractures can be present as the third most common fracture after clavicula and humerus fractures at birth where the fracture site is the diaphysis with the proximal femoral part in flexion and abduction due to the action of the adjacent muscles [8]. In patients younger than 2 years, surgery is unusual and common options of treatment includes posterior splitting, pavlic harness and pelvipedal casting [8-10].
In this report, the baby had an unusual presentation with breech delivery and fetal anomaly of myelomeningocele where bilateral femur shaft fractures had occurred as a part of clinical situation despite a special care in ceaserean delivery. Pelvipedal casting was impossible to apply also for the necessity to avoid lumbosacral irritation of the lesion (Fig. 3).
Figure 3.

Lesion on the lumbar skin due to neuromuscular disorder
To our knowledge, this is the first case with myelomeningocele sustained bilateral femur shaft fractures during caesarean section. Moreover, the state of the myelomeningocele has been thought to be as suggestive of the osteoporosis, which could have led to femur fracture.
Conclusion
Femoral fractures following abnormal deliveries, especially the baby had neuromuscular disorders with, should be looked out for, in caesarean sections. Thorough clinical examination and immediate orthopaedic consultation in the event of doubtful presentation would help. These fractures have a very good prognosis with an easy intervention.
Clinical Message.
In case of abnormal deliveries with neuromuscular disorders, clinicians must be vigilant regarding obstetric maneuver, otherwise they may experience unpleasant complications such as femur fracture.
Biography



Footnotes
Conflict of Interest: Nil
Source of Support: None
References
- 1.Cebesoy FB, Cebesoy O, Incebiyik A. Bilateral femur fracture in a newborn:an extreme complication of cesarean delivery. Arch Gynecol Obstet. 2009;279(1):73–4. doi: 10.1007/s00404-008-0639-y. [DOI] [PubMed] [Google Scholar]
- 2.García García IE, de la Vega A, García Fragoso L. Long bone fractures in extreme low birth weight infants at birth:obstetrical considerations. P R Health Sci J. 2002;21(3):253–5. [PubMed] [Google Scholar]
- 3.Alexander JM, Leveno KJ, Hauth J, Landon MB, et al. Fetal injury associated with cesarean delivery. Obstet Gynecol. National Institute of Child Health Human Development Maternal-Fetal Medicine Units Network. 2006;108:885–890. doi: 10.1097/01.AOG.0000237116.72011.f3. [DOI] [PubMed] [Google Scholar]
- 4.Toker A, Perry ZH, Cohen E, Krymko H. Cesarean section and the risk of fractured femur. Isr Med Assoc J. 2009;11(7):416–8. [PubMed] [Google Scholar]
- 5.Regalia AL, Curiel P, Natale N, Galluzzi A, et al. Routine use of external cephalic version in three hospitals. Birth. 2000;27(1):19–24. doi: 10.1046/j.1523-536x.2000.00019.x. [DOI] [PubMed] [Google Scholar]
- 6.Matsubara S, Izumi A, Nagai T, Kikkawa I, et al. “Femur fracture during abdominal breech delivery.”. Archives of Gynecology and Obstetrics. 2008;278(2):195–197. doi: 10.1007/s00404-008-0655-y. [DOI] [PubMed] [Google Scholar]
- 7.Capobianco G, Virdis G, Lisai P, Cherchi C, et al. Cesarean section and right femur fracture:A rare but possible complication for breech presentation. Case reports in obstetrics and gynecology. 2013 doi: 10.1155/2013/613709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.D’Andrea L, Catena N. Femural shaft fracture in a newborn infant treated with axial external fixator:a case report. J Pediatr Orthop. 2008;28(1):17–9. doi: 10.1097/bpo.0b013e31815b4dea. [DOI] [PubMed] [Google Scholar]
- 9.Illgen R, Rodgers WB, Hresko MT, Waters PM, et al. Femur fractures in children:treatment with early sitting spica casting. J Pediatr Orthop. 1998;18(4):481–7. [PubMed] [Google Scholar]
- 10.Podeszwa DA, Mooney JF, 3rd, Cramer KE, Mendelow MJ. Comparison of Pavlik harness application and immediate spica casting for femur fractures in infants. J Pediatr Orthop. 2004;24(5):460–2. doi: 10.1097/00004694-200409000-00002. [DOI] [PubMed] [Google Scholar]