

Abstract
Sham electroacupuncture (EA) control is commonly used to evaluate the specific effects of EA in randomized-controlled trials (RCTs). However, establishing an inert and concealable sham EA control remains methodologically challenging. Here, we aimed to systematically investigate the sham EA methods. Eight electronic databases were searched from their inception to April 2015. Ten out of the 17 sham EA methods were identified from 94 RCTs involving 6134 participants according to three aspects: needle location, depth of needle insertion and electrical stimulation. The top three most frequently used types were sham EA type A, type L and type O ordinally. Only 24 out of the 94 trials reported credibility tests in six types of sham EA methods and the results were mainly as follows: sham EA type A (10/24), type B (5/24) and type Q (5/24). Compared with sham EA controls, EA therapy in 56.2% trials reported the specific effects, of which the highest positive rate was observed in type N (3/4), type F (5/7), type D (4/6) and type M (2/3). In conclusion, several sham EA types were identified as a promising candidate for further application in RCTs. Nonetheless, more evidence for inert and concealable sham EA control methods is needed.
A randomized controlled trial (RCT) has been the cornerstone of medical clinical research since the first RCT paper entitled “Streptomycin treatment of pulmonary tuberculosis: a Medical Research Council investigation” was published in 19481. By the late 20th century, RCT was recognized as the gold standard for a clinical trial2. To improve the quality of clinical research, the methodology has been refined to avoid any bias over the past several decades. The most important design techniques for avoiding bias in clinical trials are randomization and blinding. Blinding is intended to limit the occurrence of conscious and unconscious bias in clinical trials (performance bias) conduction and interpretation of outcomes (ascertainment bias)3. Blinding is crucial for treatment evaluation because lack of blinding can bias the reliable assessment of treatment effects. For RCTs, placebo is a standard control method to blind the participants and health care providers. The purpose of placebo group is to account for the placebo effect, i.e., effects from treatment that do not depend on the treatment itself. However, blinding is difficult to ensure in non-pharmacological treatment trials because fabrication of placebo such as placebo/sham acupuncture controls requires the placebo to be both inert and indistinguishable, which is relatively difficult4.
RCTs for acupuncture appeared in 1970s5. Since then, a number of RCTs on acupuncture have been published6. The “sham” acupuncture is identified as the procedure controlling for the acupuncture treatment components with the aim to blind the participants and control for non-specific placebo effects7. Since participants are to a large extent ignorant of the components of acupuncture such as needle location, depth of needle insertion, needle stimulation and patient/practitioner interactions, sham acupuncture can be considered to be therapeutically inactive. However, it is difficult to design a standard method for sham acupuncture avoiding all therapeutically active components. Thus, the methodological difficulties in designing appropriate sham acupuncture controls for RCTs remained challenging8,9,10.
Electroacupuncture (EA) is an extension technique based on traditional acupuncture combined with modern electrotherapy11,12. Owing to its accurate, reproducible and standardized intensity and duration of stimulation with simple, verifiable electrical parameters, EA has been widely used in clinical studies and basic research into underlying mechanisms of acupuncture treatment13,14. Currently, EA is being used extensively in China and elsewhere around the world. However, no systematic analyses have yet been published to describe the sham EA procedures. Thus, the objective of this study is to investigate the sham EA methods utilized in EA RCTs.
Methods
Search strategy
Eight electronic databases, including Cochrane Controlled Trials Register, PubMed, EMBASE, AMED, China National Knowledge Infrastructure (CNKI), VIP Journals Database, Wanfang database, and Chinese Biomedical Database (CBM) were searched from their inceptions to April 2015. The search terms were confined to “Electroacupuncture” AND “sham acupuncture OR placebo acupuncture” AND “randomized controlled trial (RCT)”. All searches were limited to studies on human.
Eligibility Criteria
RCTs concerning the effects of EA on any kind of diseases with at least one control group receiving sham EA were included, regardless of publication status and languages. Quasi-RCTs and non-RCTs were excluded.
The studies were eligible if EA therapy alone or adjunct therapy were given in treatment group and secondly, if sham EA or any type of faked manipulation mimicking real EA in aspects of acupoint, penetration and electro-stimulation were given in control group. There were no restrictions on needle parameters or intensity, frequency and mode of stimulation. Studies that compared EA with transcutaneous nerve electrical stimulation (TNES), another acupuncture plus sham EA or placebo medications were excluded. If three or more groups were designed in one study, only real EA versus sham EA groups were included.
Study selection and data extraction
Two authors (ZXC, YL) reviewed the titles and abstracts of the potential references independently. All the potentially relevant studies were marked and their full articles were retrieved. Further examinations were carried out to make a final selection decision. The same two authors performed the data extraction independently for the predefined items: author, year, country, EA indications, sample size, the characteristics of interventions, outcome measures, results and dropouts. The disagreements were resolved through consulting a third part (GQZ).
Risk of bias assessment
Two authors (ZXC and YL) performed the methodological quality assessment of each included trial independently based on the Cochrane Collaboration’s tool for assessing risk of bias14. The criteria consisted of the following: adequate sequence generation, allocation concealment, blinding of participants, blinding of personnel, blinding of outcome assessor, free of incomplete outcome data, free of selective reporting and free of other bias.
Description of sham EA methods
The sham EA methods used in each control group were examined and the details were extracted according to three respects: needle location, depth of needle insertion and electrical stimulation. Partially based on the previous sham acupuncture type I~V classification published by Dincer et al.8 we summarized seventeen kinds of sham EA methods: (1) Sham EA on therapeutic acupoints plus no skin penetration plus no electrical stimulation (Sham EA type A); (2) Sham EA on therapeutic acupoints plus no skin penetration plus electrical stimulation (Sham EA type B); (3) Sham EA on therapeutic acupoints plus the same depth plus no electrical stimulation (Sham EA type C); (4) Sham EA on therapeutic acupoints plus superficial insertion plus no electrical stimulation (Sham EA type D); (5) Sham EA on therapeutic acupoints plus superficial insertion plus electrical stimulation (Sham EA type E); (6) Sham EA on nonspecific acupuncture points plus the same depth plus electrical stimulation (Sham EA type F); (7) Sham EA on nonspecific acupuncture points plus the same depth plus no electrical stimulation (Sham EA type G); (8) Sham EA on nonspecific acupuncture points plus superficial insertion plus electrical stimulation (Sham EA type H); (9) Sham EA on nonspecific acupuncture points plus superficial insertion plus no electrical stimulation (Sham EA type I); (10) Sham EA on nonspecific acupuncture points plus no skin penetration plus electrical stimulation (Sham EA type J); (11) Sham EA on nonspecific acupuncture points plus no skin penetration plus no electrical stimulation (Sham EA type K); (12) Sham EA on non-acupuncture points plus the same depth plus electrical stimulation (Sham EA type L); (13) Sham EA on non-acupuncture points plus the same depth plus no electrical stimulation (Sham EA type M); (14) Sham EA on non-acupuncture points plus superficial insertion plus electrical stimulation (Sham EA type N); (15) Sham EA on non-acupuncture points plus superficial insertion plus no electrical stimulation (Sham EA type O); (16) Sham EA on non-acupuncture points plus no skin penetration plus electrical stimulation (Sham EA type P); (17) Sham EA on non-acupuncture points plus no skin penetration plus no electrical stimulation (Sham EA type Q).
Assessment of the effectiveness
Considering wildly varying outcome measures across different disease conditions, treatment efficacy was evaluated for each study according to the modified method based on a previous publication10. The results of each trial were presented by using the following primary outcome measures: “T > C” meaning that real EA treatment group was significantly superior to sham EA control group; “ND” meaning no difference between EA and sham EA groups; “T < C” meaning that real EA group was significantly inferior to sham EA group. If the efficacy of a trial was reported as “T > C” or “T < C” without between-groups comparison having been conducted, we collected the original data by reviewing the articles or contacting the corresponding author. If the original data were available, an effect-size analysis was conducted to reconfirm the between-groups difference. If the original data were not available, the efficacy results were presented as “T > C?” or “T < C?”.
The credibility of blinding
The credibility test was formally performed in validation studies to assess the blinding effect of sham acupuncture based on credibility questionnaire and statistical analysis15,16,17. The information on the credibility test was extracted to explore the relationship between the credibility of blinding and the type of sham EA method.
Results
Study selection
A total of 679 potentially relevant articles were identified. By reviewing titles and abstracts, 374 papers were excluded for at least one of following reasons: (1) not clinical trials; (2) case report, comment, review, letter, news or editorial; (3) not in contrast with sham EA; (4) lack of EA intervention. After examining the full content of the remaining 305 articles, we removed 211 records, of which 127 articles were due to lack of sham EA controls, including electro-acupuncture (14 studies), manual acupuncture (13 studies), TNES (7 studies), other treatment (69 studies) or no treatment (24 studies); 49 articles removed for lack of real EA groups, with their target intervention designed as manual acupuncture (10 studies), TNES (38 studies) or periosteal stimulation therapy (PST) (1 study); 10 articles were not RCTs; 13 articles were double publications; 12 articles were cross-over design. Ultimately, 94 studies18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111 involving 6134 participants were selected (Fig. 1).
Figure 1. Flow diagram.

Characteristics of included studies
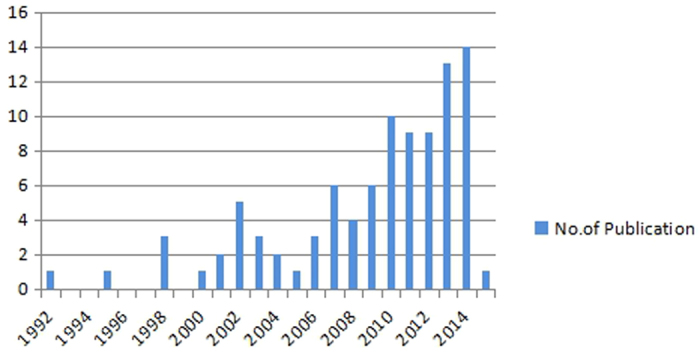
The 94 included articles were published from 1992 to 2015. Among them, 5 studies29,54,90,95,107 were published between 1992 and 1999; 33 studies22,24,25,27,30,31,38,45,47,52,53,56,57,58,67,68,71,72,73,74,77,78,81,83,84,92,93,97,104,105,106,110,111 were published between 2000 and 2010; the remaining 56 studies18,19,20,21,23,26,28,32,33,34,35,36,37,39,40,41,42,43,44,46,48,49,50,51,55,59,60,61,62,63,64,65,66,69,70,75,76,79,80,82,85,86,87,88,89,91,94,96,98,99,100,101,102,103,108,109 were reported from 2010 to 2015 (Fig. 2). Indications for EA included pain (32 studies)18,19,21,24,26,27,31,33,36,37,40,42,45,47,51,52,56,60,66,67,72,76,82,84,88,90,92,96,97,103,110,111, anesthesia (8 studies)46,50,73,74,86,89,94,102, stroke (7 studies)25,28,29,34,62,105,106, depression (6 studies)23,53,59,65,68,80, obesity (4 studies)32,49,54,70, primary dysmenorrheal/menstrual pain (4 studies)61,98,99,101, substance abuse (heroin or smoking) (3 studies)64,95,107, osteoarthritis (2 studies)22,104, migraine (2 studies)39,78, nausea and vomiting (2 studies)38,57, postoperative ileus (2 studies)35,91, insomnia (2 studies)63,81, benign prostate hyperplasia (2 studies)79,87, diabetic mellitus related diseases (2 studies)83,109, carpal tunnel syndrome (1 study)100, rheumatoid arthritis (1 study)93, whiplash-associated disorders (1 study)69, constipation (1 study)48, multiple sclerosis (1 study)41, tinnitus (1 study)20, auditory hallucination (1 study)30, attention deficit hyperactivity disorder (1 study)44, polycystic ovary syndrome (1 study)55, hot flushes (1 study)58, postpartum insufficient lactation (1 study)71, cardiac ischemia-reperfusion injury (1study)75, stress-related symptoms (1 study)108. The rest three studies43,77,85 reported the effects of EA on healthy subjects.
Figure 2. The time distribution of the included articles.
EA treatment alone was adopted in 55 trials19,20,21,22,23,24,25,26,28,29,30,31,34,35,36,37,38,39,42,43,53,55,58,60,61,66,68,69,71,72,75,77,78,79,80,83,84,85,86,87,88,89,90,91,95,98,99,100,101,103,104,107,108,110,111, while the interventions of the remaining 39 trials were a combination of EA and western conventional medicine (WCM). Four trials24,47,54,100 were designed as two groups of EA, and seven trials38,43,61,63,98,99,101 were conducted with two groups of sham EA. Compared with sham EA group, real EA group in 83 studies selected the same number of acupoints; nine studies25,46,66,89,90,105,106,108,111 used more number of acupoints; one study20 used less number of acupoints; one study52 did not report the number of acupoints. Eight studies26,49,54,76,95,96,97,110 identified acupoints by using a point detector. The “deqi” sensation was required in 65 real EA groups18,19,20,21,22,23,24,25,26,29,30,31,33,34,35,36,39,40,41,43,44,47,48,50,51,56,57,58,59,60,61,62,63,64,66,67,69,71,75,77,78,79,80,81,82,83,85,86,87,90,91,93,98,99,100,101,102,104,105,106,109,111 and 3 sham EA groups selected nonspecific acupoints61,78,101. Eight studies utilized pricking sensation to mimic needle sensation and blind participants in control group20,21,23,52,60,63,67,81. Forty-two studies19,20,21,22,26,27,28,31,32,33,34,35,37,39,40,42,43,44,46,47,50,51,58,60,61,62,64,65,66,70,71,77,78,79,83,85,89,92,100,104,105,106 applied EA at high intensity with maximum tolerance, and seventeen studies24,29,54,56,59,80,82,86,87,90,95,98,99,102,107,108,111 applied EA with low intensity below pain threshold or at a comfortable level with presence or absence of muscle contractions. The other trials were lacking in details on the intensity of stimulation. The duration of each session ranged from 5 minutes100 to 72 hours96; the total number of treatment sessions varied from 133,37,38,39,46,47,50,51,52,72,73,77,82,84,86,88,89,94,95,96,97,100,101,102,109 to 7244; the total duration of treatment ranged from 5 minutes100 to 6 months111. Ten studies27,46,72,76,77,79,89,90,97,102 did not report the duration of each session. In one study76, the total number of treatment session was not mentioned. Eight studies27,46,72,76,77,89,97,102 did not provide any information on the total duration of treatment. The characteristics of the studies were listed in Table 1.
Table 1. Characteristics of 94 included studies.
| Reference (author, year and country) | Diseases | No. of acupoint (T/C) | Sample size (T/C) | dropout (T/C) | Primary outcome measures | Difference between groups | Characteristic of sham electro-acupuncture (EA) methods |
|||
|---|---|---|---|---|---|---|---|---|---|---|
| needle location | degree of needle insertion | electrical stimulation | The type of sham EA method | |||||||
| Ntritsou et al. 2014 USA18 | Pain | 4/4 | 37/38 | 5(2/3) | NRS and SF_MPQ scores | T > C | therapeutic acupoints | no penetration | no electrical stimulation | Sham EA type A |
| Chu et al. 2012 Hong Kong19 | Pain perception in Irritable Bowel Syndrome | 6/6 | 15/15 | 0(0/0) | FMRI | T > C | therapeutic acupoints | no penetration | no electrical stimulation | Sham EA type A |
| Wang et al. 2010 Denmark20 | Tinnitus | 4/14 | 20/20 | 9(4/5) | The frequency of tinnitus occurrence and the tinnitus loudness | ND | therapeutic acupoints | no penetration | no electrical stimulation | Sham EA type A |
| Zyloney et al. 2010 USA21 | Pain | 2/2 | N/N | 29(N/N) | FMRI and MASS ratings | T > C | therapeutic acupoints | no penetration | no electrical stimulation | Sham EA type A |
| Jubb et al. 2008 UK22 | Osteoarthritis | 6/6 | 34/34 | 4(2/2) | WOMAC pain score | T > C | therapeutic acupoints | no penetration | no electrical stimulation | Sham EA type A |
| Chung et al. 2012 Hong Kong23 | Postpartum Depression | 18/18 | 10/10 | 6(5/1) | EPDS, HADS, HDRS17 and CGI scores | ND | therapeutic acupoints | no penetration | electrical stimulation | Sham EA type B |
| Barlas et al. 2006 UK24 1 | Pain | 4/4 | 12/12 | N(N/N) | Pressure pain threshold | T > C | therapeutic acupoints | no penetration | electrical stimulation | Sham EA type B |
| Barlas et al. 2006 UK24 2 | Pain | 4/4 | 12/12 | N(N/N) | Pressure pain threshold | ND | therapeutic acupoints | no penetration | electrical stimulation | Sham EA type B |
| Wayne et al. 2005 US25 | Stroke Rehabilitation | 14–22/2–3 | 16/17 | 9(3/6) | FMA score | ND | non-acupuncture points | no penetration | no electrical stimulation | Sham EA type Q |
| Sahin et al. 2010 Turkey26 | Pain | 14/14 | 15/16 | 2(2/0) | VAS scores | ND | non-acupuncture points | the same depth | electrical stimulation | Sham EA type L |
| Fanti et al. 2003 Italy27 | Pain | 10/10 | 10/10 | 0(0/0) | VAS scores | ND | non-acupuncture points | the same depth | Electrical stimulation | Sham EA type L |
| Hsing et al. 2012 Brazil28 | Stroke recovery | 11–14/11–14 | 31/31 | 0(0/0) | NIHSS, Barthel Index and modified Rankin scales scores | T > C | therapeutic acupoints | the same depth | no electrical stimulation | Sham EA type C |
| Gosman-Hedström et al. 1998 Sweden29 | Stroke | 4/4 | 37/34 | 3(2/1) | The neurological score and the Barthel and Sunnaas index scores | ND | therapeutic acupoints | superficial penetration | no electrical stimulation | Sham EA type D |
| Jing et al. 2009 China30 | Auditory hallucination | 6/6 | 30/30 | 7(4/3) | The Psychotic Symptom Rating Scales and Auditory Hallucination Subscale total score | T > C | non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Kong et al. 2009 USA31 | Pain | 2/2 | N/N | 29(N/N) | Gracely Sensory and Affective scales scores and fMRI | ND | therapeutic acupoints | no penetration | no electrical stimulation | Sham EA type A |
| Darbandi et al. 2013 Iran32 | Obesity | 4/4 | 47/47 | 8(5/3) | BW, BMI and BFM | ND | non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Yang et al. 2012 China33 | Pain | 12/12 | 40/40 | 0(0/0) | the consumption of sevoflurane and the recovery profile | T > C | therapeutic acupoints | no penetration | no electrical stimulation | Sham EA type A |
| Liu et al. 2013 China34 | Post-stroke detrusor overactivity | 10/10 | 35/36 | 5(2/3) | maximum cystometric capacity and bladder compliance | T > C | non-acupuncture points | no penetration | no electrical stimulation | Sham EA type Q |
| Zhang et al. 2014 China35 | Postoperative ileus | 2/2 | 20/20 | 1(1/0) | Time of the first bowel sounds and passage of flatus | T > C | non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Mao et al. 2014 USA36 | Aromatase Inhibitor-Related Arthralgia | 4/4 | 22/22 | 6(3/3) | BPI | ND | non-acupuncture points | no penetration | no electrical stimulation | Sham EA type Q |
| Leung et al. 2011 Hong Kong37 | Pain | 3/3 | 20/20 | 0(0/0) | the maximal tolerable pressure, VAS score and beta-endorphin level | T > C | therapeutic acupoints | no penetration | no electrical stimulation | Sham EA type A |
| Rusy et al. 2002 USA38 a | Postoperative Nausea and Vomiting | 1/1 | 40/40 | 0(0/0) | occurrence of nausea and vomiting, and use of antiemetic rescue medication | T > C | nonspecific acupuncture points | the same depth | electrical stimulation | Sham EA type F |
| Rusy et al. 2002 USA38 b | Postoperative Nausea and Vomiting | 1/1 | 40/40 | 0(0/0) | occurrence of nausea and vomiting, and use of antiemetic rescue medication | T > C | non-acupuncture points | no penetration | no electrical stimulation | Sham EA type Q |
| Yang et al. 2014 China39 | Migraine | 3/3 | 10/10 | 0(0/0) | VA S scores | ND | non-acupuncture points | the same depth | Electrical stimulation | Sham EA type L |
| Chen et al. 2013 China40 | Pancreatic cancer pain | 10/10 | 30/30 | 1(0/1) | NRS | T > C | therapeutic acupoints | no penetration | no electrical stimulation | Sham EA type A |
| Quispe-Cabanillas et al. 2012 Brazi41 | Multiple sclerosis | 9/9 | 16/15 | 0(0/0) | EDSS, pain VASscore and quality of life FAMS | T > C | non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Aranha et al. 2015 Brazil42 | Pain | 7–8/7–8 | 24/23 | 17(7/10) | VAS scores and cervical movements | T > C | non-acupuncture points | the same depth | no electrical stimulation | Sham EA type M |
| Yu et al. 2013 Hong Kong43 a | 2/2 | 12/12 | 0(0/0) | C-MMASS and HR, MAP | ND | non-acupuncture points | the same depth | Electrical stimulation | Sham EA type L | |
| Yu et al. 2013 Hong Kong43 b | 2/2 | 12/12 | 0(0/0) | C-MMASS and HR, MAP | T > C | therapeutic acupoints | superficial penetration | no electrical stimulation | Sham EA type D | |
| Li et al. 2010 Chin44 | Attention deficit hyperactivity disorder | 15–16/15–16 | 92/88 | 10(6/4) | relapse rate | T > C | therapeutic acupoints | the same depth | no electrical stimulation | Sham EA type C |
| Zheng et al. 2007 Australia45 | Chronic pain | 4/4 | 17/18 | 12(8/4) | the dosage reduction of OLM, the incidence of side effect, and VAS score | ND | non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Li et al. 2013 China46 | General anesthesia | 10/6 | 9/10 | 0(0/0) | the levels of TNF-α, IL-8 and IL-10 | ND | non-acupuncture points | the same depth | Electrical stimulation | Sham EA type L |
| Lin et al. 2002 Taiwan47 1 | Postoperative pain | 2/2 | 25/25 | 0(0/0) | VAS score | ND | therapeutic acupoints | the same depth | no electrical stimulation | Sham EA type C |
| Lin et al. 2002 Taiwan47 2 | Postoperative pain | 2/2 | 25/25 | 0(0/0) | VAS score | ND | therapeutic acupoints | the same depth | no electrical stimulation | Sham EA type C |
| Chen et al. 2013 Taiwan48 | Constipation | 6/6 | 30/30 | 30 (16/14) | the defecation rate | T > C | non-acupuncture points | the same depth | Electrical stimulation | Sham EA type L |
| Schukro et al. 2014 Austria49 | Obesity | 3/3 | 28/28 | 14(7/7) | the relative reduction of body weight | T > C | therapeutic acupoints | the same depth | no electrical stimulation | Sham EA type C |
| Yu et al. 2014 China50 | General anesthesia | 2/2 | 20/20 | 0(0/0) | The serum cortisol and ACTH | T > C ? | non-acupuncture points | the same depth | Electrical stimulation | Sham EA type L |
| Xie et al. 2014 China51 | Postoperative pain | 2/2 | 20/20 | 0(0/0) | VAS score, Total Doses of Sufentanil and Dezocine | T > C | therapeutic acupoints | the same depth | no electrical stimulation | Sham EA type C |
| Sim et al. 2002 Singapore52 | Intraoperative pain | N/N | 30/30 | 0(0/0) | The total intraoperative usage of alfentanil, The total morphine consumption and VAS score | ND | non-acupuncture points | no penetration | no electrical stimulation | Sham EA type Q |
| Song et al. 2009 China53 | Depression | 2/2 | 31/32 | 10(3/7) | HDRS and CGI | T > C | non-acupuncture points | the same depth | Electrical stimulation | Sham EA type L |
| Shafshak 1995 Egypt54 1 | Obesity | 2/2 | 10/10 | N(N/N) | the success rate of going on the diet trigmen | T > C | non-acupuncture points | the same depth | Electrical stimulation | Sham EA type L |
| Shafshak 1995 Egypt54 2 | Obesity | 2/2 | 10/10 | N(N/N) | the success rate of going on the diet trigmen | T > C | non-acupuncture points | the same depth | Electrical stimulation | Sham EA type L |
| Franasiak et al. 2012 USA55 | Polycystic Ovary Syndrome | 8/8 | 46/50 | 16(9/7) | Serum LH and FSH.The monthly rates of ovulation | ND | non-acupuncture points | no penetration | no electrical stimulation | Sham EA type Q |
| Naslund et al. 2002 Sweden56 | Idiopathic anterior knee pain | 6/6 | 30/28 | 1(0/1) | one leg vertical jump, functional score, daily VAS recording and skin temperature | ND | non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Shen et al. 2000 US57 | Chemotherapy–Induced Emesis | 4/4 | 37/33 | 1(1/1) | Total number of emesis episodes occurring | T > C | non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Wyon et al. 2004 Sweden58 | Hot flushes in postmenopausal women. | 6/6 | 15/15 | 7(4/3) | The number of flushes/24 h | ND | non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Zhang et al. 2012 Hong Kong59 | Depression | 12/12 | 38/35 | 10(7/3) | score of HAMD-17 and SDS | T > C | therapeutic acupoints | no penetration | electrical stimulation | Sham EA type B |
| Zheng et al. 2010 Australia60 | Pain | 2/2 | 12/12 | 0(0/0) | SPT and TST | T > C | therapeutic acupoints | no penetration | no electrical stimulation | Sham EA type A |
| Ma et al. 2010 China61 a | Menstrual Pain | 2/2 | 13/14 | 1(1/0) | VAS scores | T > C | nonspecific acupuncture points | the same depth | electrical stimulation | Sham EA type F |
| Ma et al. 2010 China61 b | Menstrual Pain | 2/2 | 13/12 | 1(1/0) | VA S scores | T > C | non-acupuncture points | the same depth | Electrical stimulation | Sham EA type L |
| Wang et al. 2014 Taiwan62 | Chronic stroke | 4/4 | 10/10 | 5(1/4) | R1, R2 and R2–R1 | T > C | therapeutic acupoint | superficial penetration | No electrical stimulation | Sham EA type D |
| Yeung et al. 2011 Hong Kong63 a | Insomnia | 8/8 | 26/26 | 7(4/3) | ISI and PSQI | ND | non-acupuncture points | superficial penetration | electrical stimulation | Sham EA type N |
| Yeung et al. 2011 Hong Kong63 b | Insomnia | 8/8 | 26/26 | 7(4/3) | ISI and PSQI | T > C | non-acupuncture points | No penetration | No electrical stimulation | Sham EA type Q |
| Chan et al. 2014 Taiwan64 | Heroin Addicts | 4/4 | 30/30 | 2(1/1) | the daily consumption of methadone | T > C | therapeutic acupoint | superficial penetration | no electrical stimulation | Sham EA type D |
| Man et al. 2014 Hong Kong65 | Post-stroke depression | 20/20 | 23/20 | 10(4/6) | HAMD-17 and CGI-S | T > C | therapeutic acupoint | No penetration | electrical stimulation | Sham EA type B |
| Oh et al. 2013 Australia66 | Pain | 16/12 | 16/16 | 3(2/1) | WOMAC, BPI-SF and FACT-G instrument | ND | therapeutic acupoint | No penetration | No electrical stimulation | Sham EA type A |
| Wong et al. 2006 Hong Kong67 | Pain | 4/4 | 13/14 | 2(0/2) | VAS pain score | ND | therapeutic acupoint | No penetration | No electrical stimulation | Sham EA type A |
| Song et al. 2007 USA68 | Depression | 2/2 | N/N | N(N/N) | 24-item HAMD and the level of G protein α subtypes in the platelet membrane | ND | non-acupuncture points | the same depth | no electrical stimulation | Sham EA type M |
| Cameron et al. 2011 Australia69 | Whiplash-associated Disorders | 8/8 | 64/60 | 8(0/8) | VAS | T > C | non-acupuncture points | the same depth | no electrical stimulation | Sham EA type M |
| Darbandi et al. 2014 Iran70 | Obesity | 4/4 | 20/20 | 0(0/0) | BMI, TFM, WC and HC | T > C | non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Wei et al. 2008 China71 | Postpartum Insufficient Lactation | 2/2 | 46/46 | 0(0/0) | total therapeutic effect, 24-hour milk secretion quantity, prolactin level | T > C | nonspecific acupuncture points | the same depth | electrical stimulation | Sham EA type F |
| Wang et al. 2007 USA72 | Pain | 4/4 | 29/27 | 0(0/0) | intraprocedural alfentanil consumption, VAS score | T > C | therapeutic acupoint | superficial penetration | no electrical stimulation | Sham EA type D |
| Kvorning et al. 2003 Sweden73 | Anaesthesia | 12/12 | 23/23 | 1(1/0) | Physiological reactions to skin incision | T > C | therapeutic acupoint | No penetration | no electrical stimulation | Sham EA type A |
| Kvorning et al. 2003 Sweden74 | Anaesthesia | 6/6 | 23/23 | 0(0/0) | The minimal alveolar concentration of sevoflurane | T < C | therapeutic acupoint | No penetration | no electrical stimulation | Sham EA type A |
| Yang et al. 2010 China75 | Cardiac ischemia-reperfusion injury | 6/6 | 30/30 | 0(0/0) | levels of serum cardiac troponin I | T > C | therapeutic acupoint | the same depth | no electrical stimulation | Sham EA type C |
| Sahmeddini et al. 2010 Iran76 | Perioperative Pain | 4/4 | 45/45 | 0(0/0) | score on VAS-100 | ND | therapeutic acupoint | no penetration | no electrical stimulation | Sham EA type A |
| Wang et al. 2007 China77 | 1/1 | 9/5 | 3(3/0) | BOLD fMRI | T > C | non-acupuncture points | the same depth | electrical stimulation | Sham EA type L | |
| Jia et al. 2009 China78 | Migraine | 2/2 | 138/138 | 1(0/1) | VAS score and the plasma 5-HT level | T > C | nonspecific acupuncture points | the same depth | electrical stimulation | Sham EA type F |
| Wang et al. 2013 China79 | Benign prostate hyperplasia | 2/2 | 50/50 | 23(9/14) | IPSS | T > C | non-acupuncture points | the same depth | electrical stimulation | Sham EA type L |
| Andreescu et al. 2011 Canada80 | Depression | 2/2 | 28/29 | 11(4/7) | HDRS score | ND | non-acupuncture points | superficial penetration | No electrical stimulation | Sham EA type O |
| Yeung et al. 2009 Hong Kong81 | Insomnia | 8/8 | 30/30 | 3(1/2) | ISI | ND | therapeutic acupoint | no penetration | no electrical stimulation | Sham EA type A |
| Chen et al. 2014 Taiwan82 | Pain | 1/1 | 25/24 | 0(0/0) | VAS scores and the dosage of opium derivative analgesic | ND | therapeutic acupoint | the same depth | no electrical stimulation | Sham EA type C |
| Wang et al. 2008 China83 | Diabetic Gastroparesis | 4/4 | 11/12 | 4(2/2) | GCSI score | T > C | non-acupuncture points | superficial penetration | electrical stimulation | Sham EA type N |
| Meissner et al. 2004 Germany84 | Pain | 6/6 | 8/8 | 0(0/0) | SEPs | T > C | therapeutic acupoint | no penetration | electrical stimulation | Sham EA type B |
| Zhou et al. 2012 China85 | 2/2 | 11/11 | 0(0/0) | MVC strength | ND | non-acupuncture points | the same depth | electrical stimulation | Sham EA type L | |
| Yeh et al. 2012 Taiwan86 | Shivering during regional anesthesia | 4/4 | 40/40 | 0(0/0) | Shivering score and tympanic temperature | T > C | non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Yu et al. 2011 Taiwan87 | Benign Prostate Hyperplasia | 6/6 | 21/21 | 5(3/2) | The change of the maximum flow rate, average flow rate, void volume | T > C | non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Ma et al. 2011 China88 | Pain | 2/2 | 116/117 | 0(0/0) | VAS score | T > C | therapeutic acupoint | no penetration | no electrical stimulation | Sham EA type B |
| Li et al. 2013 China89 | Intraoperative immunosuppression | 10/6 | 19/19 | 0(0/0) | the levels of TNFα, IL-8, IL-10, IgM, IgA, IgG and full blood count | ND | non-acupuncture points | the same depth | electrical stimulation | Sham EA type L |
| Deluze et al. 1992 Switzerland90 | Fibromyalgia | 4-10/4 | 36/34 | 15(8/7) | Pain threshold, number of analgesic tablets used, VAS score | T > C | non-acupuncture points | superficial penetration | electrical stimulation | Sham EA type N |
| Ng et al. 2013 Hong Kong91 | Postoperative ileus | 4/4 | 55/55 | 0(0/0) | Time to defecation | T > C | non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Lee and Lee 2009 Republic of Korea92 | Chronic Prostatitis / Chronic Pelvic Pain Syndrome | 6/6 | 13/13 | 5(2/3) | NIH-CPSI | T > C | Non-acupuncture points | superficial penetration | no electrical stimulation | Sham EA type O |
| Tam et al. 2007 Hong Kong93 | Rheumatoid arthritis | 6/6 | 12/12 | 5(0/5) | VAS | ND | Therapeutic acupoint | Superficial penetration | No electrical stimulation | Sham EA type D |
| Kvorning and Akeson 2010 Sweden94 | Anaesthesia | 12/12 | 22/23 | 0(0/0) | Plasma levels of adrenaline | T > C | Therapeutic acupoint | No penetration | No electrical stimulation | Sham EA type A |
| Waite and Clough 1998 UK95 | Smoking cessation | 2/2 | 40/38 | 0(0/0) | Biochemically validated total cessation of smoking | T > C | Non-acupuncture points | superficial penetration | Electrical stimulation | Sham EA type N |
| Holzer et al. 2011 Austria96 | Postoperative pain | 3/3 | 20/20 | 0(0/0) | VAS scores and the consumption of piritramide | ND | Therapeutic acupoint | No penetration | No electrical stimulation | Sham EA type A |
| Sator-Katzenschlager et al. 2006 Austria97 | Perioperative pain | 3/3 | 32/30 | 1(0/1) | VAS scores, adverse event and analgesic drug consumption | T > C | Therapeutic acupoint | No penetration | No electrical stimulation | Sham EA type A |
| Liu et al. 2011 China98 a | Primary dysmenorrhea | 1/1 | 50/50 | 5(3/2) | VAS scores | ND | Nonspecific acupuncture points | The same depth | Electrical stimulation | Sham EA type F |
| Liu et al. 2011 China98 b | Primary dysmenorrhea | 1/1 | 50/46 | 6(3/3) | VAS scores | ND | Non-acupuncture points | The same depth | Electrical stimulation | Sham EA type L |
| Liu et al. 2014 China99 a | Primary dysmenorrhea | 2/2 | 167/167 | 6(4/2) | VAS scores | T > C | Nonspecific acupuncture points | The same depth | Electrical stimulation | Sham EA type F |
| Liu et al. 2014 China99 b | Primary dysmenorrhea | 2/2 | 167/167 | 6(4/2) | VAS scores | T > C | Non-acupuncture points | The same depth | Electrical stimulation | Sham EA type L |
| Maeda et al. 2013 USA100 1 | Carpal tunnel syndrome | 2/2 | 22/19 | 0(0/0) | functional MRI, VAS scores | T > C | Non-acupuncture points | No penetration | No electrical stimulation | Sham EA type F |
| Maeda et al. 2013 USA100 2 | Carpal tunnel syndrome | 2/2 | 18/19 | 0(0/0) | functional MRI, VAS scores | T > C | Non-acupuncture points | No penetration | No electrical stimulation | Sham EA type F |
| Shi et al. 2011 China101 a | Primary dysmenorrhea | 1/1 | 10/10 | 0(0/0) | VAS scores, The plasma PGE2, PGF2a, TXB2, and 6-keto PGF1a levels | ND | Nonspecific acupuncture points | The same depth | Electrical stimulation | Sham EA type F |
| Shi et al. 2011 China101 b | Primary dysmenorrhea | 1/1 | 10/10 | 0(0/0) | VAS scores, The plasma PGE2, PGF2a, TXB2, and 6-keto PGF1a levels | ND | Non-acupuncture points | The same depth | Electrical stimulation | Sham EA type L |
| Dias et al. 2010 Brazil102 | Local anaesthesia | 8/8 | 16/17 | 0(0/0) | VAS scores | ND | Therapeutic acupoint | No penetration | No electrical stimulation | Sham EA type A |
| Zhang et al. 2013 Hong Kong103 | Chronic neck Pain | 5/5 | 103/103 | 46(19/27) | NPQ scores | ND | Therapeutic acupoint | No penetration | No electrical stimulation | Sham EA type A |
| Sangdee et al. 2002 Thailand104 | Osteoarthritis of the knee | 4/4 | 48/47 | 4(2/2) | VAS score, and Lequesne’s functional index | T > C | Therapeutic acupoint | No penetration | No electrical stimulation | Sham EA type A |
| Johansson et al. 2001 Sweden105 | Stroke rehabilitation | 9–10/4 | 48/51 | 20(11/9) | The scores of Barthel Index, the Rivermead Mobility Index and NHP, the time needed to walk 10 meters | ND | Therapeutic acupoint | No penetration | Electrical stimulation | Sham EA type B |
| Hopwood et al. 2008 UK106 | Stroke recovery | 8–10/6 | 57/48 | 13(10/3) | The scores of Barthel Index | ND | Therapeutic acupoint | No penetration | No electrical stimulation | Sham EA type A |
| White et al. 1998 England107 | Tobacco addiction | 2/2 | 38/38 | 24 (11/13) | VAS score | ND | Non-acupuncture points | No penetration | No electrical stimulation | Sham EA type Q |
| Dias et al. 2014 Brazil108 | Stress-related symptoms | 13/8 | 33/20 | 5(3/2) | The scores of MSQ, PSQI and MBI-SS | T > C | Therapeutic acupoint | No penetration | No electrical stimulation | Sham EA type A |
| Lin et al. 2013Taiwan109 | Insulin Resistance | 2/2 | 16/15 | 1(1/0) | Plasma glucose | ND | Therapeutic acupoint | No penetration | No electrical stimulation | Sham EA type A |
| Michalek-Sauberer et al. 2007 Austria110 | Perioperative pain | 3/3 | 76/36 | 24(16/8) | 5-point verbal rating scale, Time and amount of analgesic intake | ND | Therapeutic acupoint | No penetration | No electrical stimulation | Sham EA type A |
| Carlsson and Sjolund 2001 Sweden111 | Chronic Low Back Pain | 4/2 | 16/16 | 0(0/0) | VAS scores, Intake of analgesics, Sleep quality and level of activity | T > C? | Non-acupuncture points | No penetration | No electrical stimulation | Sham EA type Q |
T, treatment group/real EA group; C, control group/sham EA group; NS, not stated; T > C, EA treatment group was significantly superior to sham EA control group; ND, no difference between EA and sham EA group; T < C, real EA group was significantly inferior to sham EA group; T > C?, the efficacy result of trial was reported as “T > C” without conducting the between-group analysis and with the original data not available; NRS, Numerical Rating Scale; SF_MPQ, Short-Form McGill Scale; FMRI, Functional magnetic resonance imaging; MASS, the Massachusetts General Hospital Acupuncture Sensation Scale; WOMAC, The Western Ontario and McMaster University Osteoarthritis Index; EPDS, Edinburgh Postnatal Depression Scale; HADS, Hospital Anxiety and Depression Scale; HDRS17, 17-item Hamilton Rating Scale for Depression; CGI, Clinical Global Impression; FMA, Fugl-Meyer Assessment; VAS, Visual Analog Scale; NIHSS, the National Institutes of Health Stroke Scale. BW, body weight; BMI, body mass index; BFM, body fat mass; BPI, Brief Pain Inventory; EDSS, Expanded Disability Status Scale; FAMS, Functional Assessment of multiple Sclerosis; C-MMASS, Modified Massachusetts General Hospital Acupuncture Sensation Scale – Chinese version; HR, Heart rate; MAP, mean arterial blood pressure; OLM, opioid-like medication; TNF-α, tumor necrosis factor-α; IL-8, interleukin-8; IL-10, interleukin-10; HDRS, Hamilton Depression Rating Scale; HAMD-17, the 17-item Hamilton Rating Scale for Depression; SDS, the Chinese-version Self-rating Depression Scale; SPT, single pain threshold; TST, temporal summation thresholds; R1, angle of muscle reaction; R2, passive range of motion; R2–R1, dynamic component; ISI, The Insomnia Severity Index; PSQI, the Pittsburgh Sleep Quality Index; CGI-S, the Clinical Global Impression - Severity scale; BPI-SF, Brief Pain Inventory Short Form; FACT-G instrument, the Functional Assessment of Cancer Therapy-General instrument; 24-item HAMD, the 24-item Hamilton Depression Rating Scale; TFM, Trunk Fat Mass; WC, Waist Circumference; HC, Hip Circumference; VAS-100, a 100-mm visual analogue scale; BOLD fMRI, blood oxygen level dependent functional magnetic resonance imaging; IPSS, the International Prostate Symptom Score; GCSI, the Gastroparesis Cardinal Symptom Index; SEPs, somatosensory evoked potentials; MVC, maximal voluntary contraction; NIH-CPSI, NIH-Chronic Prostatitis Symptom Index; NPQ, the Northwick Park Neck Pain Questionnaire; NHP, the Nottingham Health Profile; MSQ, Mini-Sleep Questionnaire; MBI-SS, the Maslach Burnout Inventory—Student Survey.
Note: Sham EA type A: sham EA on therapeutic acupoints plus no penetration plus no electrical stimulation; Sham EA type B: sham EA on therapeutic acupoints plus no penetration plus electrical stimulation; Sham EA type C: sham EA on therapeutic acupoints plus the same depth plus no electrical stimulation; Sham EA type D: sham EA on therapeutic acupoints plus superficial penetration plus no electrical stimulation; Sham EA type F: sham EA on nonspecific acupuncture points plus the same depth plus electrical stimulation; Sham EA type L: sham EA on non-acupuncture points plus the same depth plus electrical stimulation; Sham EA type M: sham EA on non-acupuncture points plus the same depth plus no electrical stimulation; Sham EA type N: sham EA on non-acupuncture points plus superficial penetration plus electrical stimulation; Sham EA type O: sham EA on non-acupuncture points plus superficial penetration plus no electrical stimulation; Sham EA type Q: sham EA on non-acupuncture points plus no penetration plus no electrical stimulation.
Characteristics of sham EA
Ten different types of sham EA methods used in the trials were identified as follows: (1) sham EA type A were used in twenty-six control groups18,19,20,21,22,31,33,37,40,60,66,67,73,74,76,81,94,96,97,102,103,104,106,108,109,110; (2) sham EA type B were used in seven control groups23,24,59,65,84,88,105; (3) sham EA type C were used in seven control groups28,44,47,49,51,75,82; (4) sham EA type D were used in six control groups29,43,62,64,72,93; (5) sham EA type F were used in seven control groups38,61,71,78,98,99,101; (6) sham EA type L were used in seventeen control groups26,27,39,43,46,48,50,53,54,61,77,79,85,89,98,99,101; (7) sham EA type M were used in three control groups42,68,69; (8) sham EA type N were used in four control groups63,83,90,95; (9) sham EA type O were used in fourteen control groups30,32,35,41,45,56,57,58,70,80,86,87,91,92; and (10) sham EA type Q were used in ten control groups25,34,36,38,52,55,63,100,107,111.
For the needle location, 48 sham EA groups25,26,27,30,32,34,35,36,38,39,41,42,43,45,46,48,50,52,53,54,55,56,57,58,61,63,68,69,70,77,79,80,83,85,86,87,89,90,91,92,95,98,99,100,101,107,111 chose non-acupoints that were either located away from the therapeutic acupoints with a distance ranging from 1 cm to 40 cm or devised in advance to avoid any known meridian or extra-point. Seven sham EA groups38,61,71,78,98,99,101 received nonspecific acupuncture points which were thought to be ineffective for treating the diseases. For the depth of needle insertion, 34 sham EA groups26,27,28,38,39,42,43,44,46,47,48,49,50,51,53,54,61,68,69,71,75,77,78,79,82,85,89,98,99,101 conducted the needle insertion to the same depth as corresponding real EA groups. Twenty-four sham EA groups29,30,32,35,41,43,45,56,57,58,62,63,64,70,72,80,83,86,87,90,91,92,93,95 performed either superficial or subcutaneous needle insertion with depth varying from 0.5 mm to 2 cm, whereas one study93 retracted the needle after superficial penetration. The remaining 43 sham EA groups had sham EA without skin penetration. Forty-one out of 43 trials did not apply any needle insertion by using Streitberger needles21,23,25,31,36,55,59,63,65,66,81, contractible placebo needles with dull tips and tubes24,37,52, placebo needles with blunted tips19,20,40,60,67,100, verum needles fixed by tapes or rings without piercing18,22,34, leading wires alone without needles33,38,76,97 and mock laser pen103 or electrodes73,74,94,96,102,104,105,106,107,108,109,110,111. Two sham EA groups84,88 did not describe any details on the sham needles. For electrical stimulation, 35 sham EA groups23,24,26,27,38,39,43,46,48,50,53,54,59,61,63,65,71,77,78,79,83,84,85,88,89,90,95,98,99,101,105 used electrical stimulation, whereas two sham EA groups stimulated with current just at the beginning of sham procedure. The other sham EA groups18,19,20,21,22,25,28,29,30,31,32,33,34,35,36,37,38,40,41,42,43,44,45,47,49,51,52,55,56,57,58,60,62,63,64,66,67,68,69,70,72,73,74,75,76,80,81,82,86,87,91,92,93,94,96,97,100,102,103,104,106,107,108,109,110,111 did not receive any electrical stimulation through inactivated EA device or disconnected cables. The details of sham EA were described in Table S1.
Risk of bias assessment
The number of items complied with the criteria varied from 3/8 to 7/8 with the average of 5.2. All 94 studies declared randomization and 63 studies reported the details. Among them, 49 studies18,19,22,23,24,25,27,29,35,36,37,38,42,43,44,45,47,49,51,55,59,60,61,62,63,64,65,66,67,70,71,72,81,88,90,91,92,93,96,97,98,99,102,106,107,108,109,110,111 described a computer-generated randomization; 11 studies32,40,41,50,52,57,69,73,74,85,86 were based on random number Table; 3 studies83,87,101 used the lot. Adequate allocation concealment was found in 43 studies18,19,20,23,25,29,30,35,36,37,43,44,45,55,57,58,60,61,63,64,65,66,67,69,71,72,76,79,81,84,86,88,90,91,93,98,99,105,106,107,109,110,111 with sequentially numbered, opaque, sealed envelopes or independent administrator. The remaining 51 studies did not provide the details on allocation concealment. Blinding of participant was described in all 94 studies. Among these, 23 studies22,23,25,34,36,45,52,57,59,60,63,65,72,81,88,97,102,103,105,106,107,108,110 proved their success of blinding by credibility test, while one study66 failed in blinding of participant after testing by statistical analysis. No study mentioned blinding of acupuncturists. Ninety-two out of the 94 studies reported blinding of assessor, whereas one study54 did not contain any information on assessor blinding and another study66 was sorted as “no” due to its unsuccessful assessor blinding. Eighteen studies25,30,45,60,65,69,79,80,91,92,93,97,98,99,103,105,106,107 conducted intention-to-treat analysis. Seventy-five studies18,19,20,21,22,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,43,44,46,47,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,70,71,72,73,74,75,76,77,78,79,81,82,83,84,85,86,87,88,89,90,91,92,94,95,96,97,100,101,102,103,104,105,108,109,110,111 were free of incomplete outcome data; eleven studies23,42,45,48,69,80,93,98,99,106,107 assessed as “no” due to high dropout rate or statistically significant differences between groups in withdrawals from the treatment. The rest were unclear due to lack of information on this aspect. Sixteen studies36,39,41,42,44,59,63,64,75,79,80,86,91,93,98,99 were free of selective reporting; one study65 was sorted as “no” due to an incomplete outcome measurement report that had been registered in protocol; the others were unclear because such details were not found. Of the 91 trials that provided the information on other bias, 77 studies18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,60,61,62,63,64,65,66,67,68,70,72,73,74,75,76,79,80,83,84,85,86,87,88,89,91,92,93,94,95,96,97,99,101,103,104,105,109,111 were free of other bias; 14 studies57,58,59,69,78,81,82,90,98,102,106,107,108,110 were assessed as “no” due to the statistical differences in baseline variables regarding as the most important prognosis. The details on the risk of bias studies were summarized in Table 2.
Table 3. Summary of effect result within different type of sham electro-acupuncture methods and electro-acupuncture indications.
| electro-acupuncture (EA) indications | The type of sham EA method |
The NO. of reference included | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sham EA type A 26 control groups | Sham EA type B 7 control groups | Sham EA type C 7 control groups | Sham EA type D 6 control groups | Sham EA type F 7 control groups | Sham EA type L 17 control groups | Sham EA type M 3 control groups | Sham EA type N 4 control groups | Sham EA type O 14 control groups | Sham EA type Q 10 control groups | ||
| Pain 32 RCTs | T > C 8 comparisons ND 7 comparisons | T > C 3 comparisons ND 1 comparison | T > C 1 comparison ND 3 comparisons | T > C 1 comparison | ND 2 comparisons | T > C 1 comparison | T > C 1 comparison | T > C 1 comparison ND 2 comparisons | ND 2 comparisons T > C? 1 comparison | T > C 16 ND 17 T > C? 1 | |
| Obesity 4 RCTs | T > C 1 comparison | T > C 2 comparisons | T > C 1 comparison ND 1 comparison | T > C 4 ND 1 | |||||||
| Anesthesia 8 RCTs | T > C 2 comparisons ND 1 comparison T < C 1 comparison | ND 2 comparisons T > C? 1 comparison | T > C 1 comparison | T > C 3 ND 3 T < C 1 T > C? 1 | |||||||
| Stroke 7 RCTs | ND 1 comparison | ND 1 comparison | T > C 1 comparison | T > C 1 comparison ND 1 comparison | T > C 1 comparison ND 1 comparison | T > C 3 ND 4 | |||||
| Depression 6 RCTs | T > C 2 comparisons ND 1 comparison | T > C 1 comparison | ND 1 comparison | ND 1 comparison | T > C 3 ND 3 | ||||||
| Primary dysmenorrhea and (or) Menstrual Pain 4 RCTs | T > C 2 comparisons ND 2 comparisons | T > C 2 comparisons ND 2 comparisons | T > C 4 ND 4 | ||||||||
| Substance abuse 3 RCTs | T > C 1 comparison | T > C 1 comparison | ND 1 comparison | T > C 2 ND 1 | |||||||
| Healthy 3 RCTs | T > C 1 comparison | T > C 1 comparison ND 2 comparisons | T > C 2 ND 2 | ||||||||
| Osteoarthritis 2 RCTs | T > C 2 comparisons | T > C 2 | |||||||||
| Migraine 2 RCTs | T > C 1 comparison | ND 1 comparison | T > C 1 ND 1 | ||||||||
| Nausea and Vomiting 2 RCTs | T > C 1 comparison | T > C 1 comparison | T > C 1 comparison | T > C 3 | |||||||
| Postoperative ileus 2 RCTs | T > C 2 comparisons | T > C 2 | |||||||||
| Insomnia 2 RCTs | ND 1 comparison | ND 1 comparison | T > C 1 comparison | T > C 1 ND 2 | |||||||
| benign prostate hyperplasia 2 RCTs | T > C 1 comparison | T > C 1 comparison | T > C 2 | ||||||||
| Diabetic mellitus 2 RCTs | ND 1 comparison | T > C 1 comparison | T > C 1 ND 1 | ||||||||
| Carpal tunnel syndrome 1 RCTs | T > C 2 comparisons | T > C 2 | |||||||||
| Rheumatoid arthritis 1 RCTs | ND 1 comparison | ND 1 | |||||||||
| Whiplash-associated disorders 1 RCTs | T > C 1 comparison | T > C 1 | |||||||||
| Constipation 1 RCTs | T > C 1 comparison | T > C 1 | |||||||||
| Multiple sclerosis 1 RCTs | T > C 1 comparison | T > C 1 | |||||||||
| Tinnitus 1 RCTs | ND 1 comparison | ND 1 | |||||||||
| Auditory hallucination 1 RCTs | T > C 1 comparison | T > C 1 | |||||||||
| ADHD (Attention deficit hyperactivity disorder) 1 RCTs | T > C 1 comparison | T > C 1 | |||||||||
| PCOS (Polycystic Ovary Syndrome) 1 RCTs | ND 1 comparison | ND 1 | |||||||||
| hot flushes in postmenopausal women 1 RCTs | ND 1 comparison | ND 1 | |||||||||
| Postpartum Insufficient Lactation 1 RCTs | T > C 1 comparison | T > C 1 | |||||||||
| Cardiac ischemia-reperfusion injury 1 RCTs | T > C 1 comparison | T > C 1 | |||||||||
| Stress-related symptoms 1 RCTs | T > C 1 comparison | T > C 1 | |||||||||
| The positive rate of efficacy result | T > C 13 ND 12 T < C 1 T > C? 0 53.8% (14/26 comparisons) | T > C 5 ND 3 62.5% (5/8 comparisons) | T > C 5 ND 3 62.5% (5/8 comparisons) | T > C 4 ND 2 66.7% (4/6 comparisons) | T > C 5 ND 2 71.4% (5/7 comparisons) | T > C 8 ND 9 T > C? 1 44.4% (8/18 comparisons) | T > C 2 ND 1 66.7% (2/3 comparisons) | T > C 3 ND 1 75% (3/4 comparisons) | T > C 9 ND 5 64.3% (9/14 comparisons) | T > C 5 ND 5 T > C? 1 45.5% (5/11 comparisons) | T > C 59 ND 43 T < C 1 T > C? 2 57.1% (60/105 comparisons) |
NOTE: T > C, EA treatment group was significantly superior to sham EA control group; ND, no difference between EA and sham EA group; T < C, real EA group was significantly inferior to sham EA group; T > C?, the efficacy result of trial was reported as “T > C” without conducting the between-group analysis and with the original data not available.
Table 2. Risk of bias of included studies.
| Reference (author, year and country) | A | B | C | D | E | F | G | H |
|---|---|---|---|---|---|---|---|---|
| Ntritsou et al. 2014 USA18 | + | + | + | − | + | + | ? | + |
| Chu et al. 2012 Hong Kong19 | + | + | + | − | + | + | ? | + |
| Wang et al. 2010 Denmark20 | + | + | + | − | + | + | ? | + |
| Zyloney et al. 2010 USA21 | + | − | + | − | + | ? | ? | + |
| Jubb et al. 2008 UK22 | + | − | + | − | + | + | ? | + |
| Chung et al. 2012 Hong Kong23 | + | + | + | − | + | − | ? | + |
| Barlas et al. 2006 UK24 | + | − | + | − | + | ? | ? | + |
| Wayne et al. 2005 US25 | + | + | + | − | + | + | ? | + |
| Sahin et al. 2010 Turkey26 | + | + | + | − | + | + | ? | + |
| Fanti et al. 2003 Italy27 | + | − | + | − | + | + | ? | + |
| Hsing et al. 2012 Brazil28 | + | − | + | − | + | + | ? | + |
| Gosman-Hedström et al. 1998 Sweden29 | + | + | + | − | + | + | ? | + |
| Jing et al. 2009 China30 | + | + | + | − | + | + | ? | + |
| Kong et al. 2009 USA31 | + | − | + | − | + | ? | ? | + |
| Darbandi et al. 2013 Iran32 | + | ? | + | − | + | ? | ? | + |
| Yang et al. 2012 China33 | + | ? | + | − | + | + | ? | + |
| Liu et al. 2013 China34 | + | + | + | − | + | + | ? | + |
| Zhang et al. 2014 China35 | + | + | + | − | + | + | ? | + |
| Mao et al.2014 USA36 | + | + | + | − | + | + | + | + |
| Leung et al. 2011 Hong Kong37 | + | + | + | − | + | + | ? | + |
| Rusy et al. 2002 USA38 | + | ? | + | − | + | + | ? | + |
| Yang et al. 2014 China39 | + | ? | + | − | + | + | + | + |
| Chen et al. 2013 China40 | + | ? | + | − | + | + | ? | + |
| Quispe-Cabanillas et al. 2012 Brazil41 | + | ? | + | − | + | + | + | + |
| Aranha et al. 2015 Brazil42 | + | ? | + | − | + | − | + | + |
| Yu et al. 2013 Hong Kong43 | + | + | + | ? | + | + | ? | + |
| Li et al. 2010 China44 | + | + | + | − | + | + | + | + |
| Zheng et al. 2007 Australia45 | + | + | + | − | + | − | ? | + |
| Li et al. 2013 China46 | + | ? | + | ? | + | + | ? | + |
| Lin et al. 2002 Taiwan47 | + | ? | + | ? | + | + | ? | + |
| Chen et al. 2013 Taiwan48 | + | ? | + | − | + | − | ? | + |
| Schukro et al. 2014 Austria49 | + | ? | + | ? | + | + | ? | + |
| Yu et al. 2014 China50 | + | ? | + | − | + | + | ? | + |
| Xie et al. 2014 China51 | + | ? | + | ? | + | + | ? | + |
| Sim et al. 2002 Singapore52 | + | ? | + | − | + | + | ? | + |
| Song et al. 2009 China53 | + | ? | + | ? | + | ? | ? | + |
| Shafshak 1995 Egypt54 | + | ? | + | ? | ? | ? | ? | + |
| Franasiak et al. 2012 USA55 | + | + | + | − | + | + | ? | + |
| Naslund et al. 2002 Sweden56 | + | ? | + | − | + | ? | ? | + |
| Shen et al. 2000 US57 | + | + | + | − | + | + | ? | − |
| Wyon et al. 2004 Sweden58 | + | + | + | − | + | + | ? | − |
| Zhang et al. 2012 Hong Kong59 | + | ? | + | − | + | + | + | − |
| Zheng et al. 2010 Australia60 | + | + | + | − | + | + | ? | + |
| Ma et al. 2010 China61 | + | + | + | − | + | + | ? | + |
| Wang et al. 2014 Taiwan62 | + | ? | + | − | + | + | ? | + |
| Yeung et al. 2011 Hong Kong63 | + | + | + | − | + | + | + | + |
| Chan et al. 2014 Taiwan64 | + | + | + | − | + | + | + | + |
| Man et al. 2014 Hong Kong65 | + | + | + | − | + | + | − | + |
| Oh et al. 2013 Australia66 | + | + | − | − | − | + | ? | + |
| Wong et al. 2006 Hong Kong67 | + | + | + | − | + | + | ? | + |
| Song et al. 2007 USA68 | + | ? | + | ? | + | ? | ? | + |
| Cameron et al. 2011 Australia69 | + | + | + | − | + | − | ? | − |
| Darbandi et al. 2014 Iran70 | + | ? | + | − | + | + | ? | + |
| Wei et al. 2008 China71 | + | + | + | ? | ? | + | ? | ? |
| Wang et al. 2007 USA72 | + | + | + | − | + | + | ? | + |
| Kvorning et al. 2003 Sweden73 | + | ? | + | − | + | + | ? | + |
| Kvorning et al. 2003 Sweden74 | + | ? | + | − | + | + | ? | + |
| Yang et al.2010 China75 | + | ? | + | − | + | + | + | + |
| Sahmeddini et al.2010 Iran76 | + | + | + | ? | + | + | ? | + |
| Wang et al. 2007 China77 | + | ? | + | − | + | + | ? | ? |
| Jia et al. 2009 China78 | + | ? | + | ? | + | + | ? | − |
| Wang et al. 2013 China79 | + | + | + | − | + | + | + | + |
| Andreescu et al. 2011 Canada80 | + | ? | + | − | + | + | + | + |
| Yeung et al. 2009 Hong Kong81 | + | + | + | − | + | + | ? | − |
| Chen et al. 2014 Taiwan82 | + | ? | + | ? | + | + | ? | + |
| Wang et al. 2008 China83 | + | ? | + | − | + | + | ? | + |
| Meissner et al. 2004 Germany84 | + | + | + | − | + | + | ? | + |
| Zhou et al. 2012 China85 | + | ? | + | − | + | + | ? | + |
| Yeh et al. 2012 Taiwan86 | + | + | + | − | + | + | + | + |
| Yu et al. 2011 Taiwan87 | + | ? | + | − | + | + | ? | + |
| Ma et al. 2011 China88 | + | + | + | − | + | + | ? | + |
| Li et al. 2013 China89 | + | ? | + | ? | + | + | ? | + |
| Deluze et al. 1992 Switzerland90 | + | + | + | − | + | + | ? | − |
| Ng et al. 2013 Hong Kong91 | + | + | + | − | + | + | + | + |
| Lee and Lee 2009 Republic of Korea92 | + | ? | + | − | + | + | ? | + |
| Tam et al. 2007 Hong Kong93 | + | + | + | − | + | − | + | + |
| Kvorning and Akeson 2010 Sweden94 | + | ? | + | − | + | + | ? | + |
| Waite and Clough 1998 UK95 | + | ? | + | ? | + | + | ? | + |
| Holzer et al. 2011 Austria96 | + | ? | + | − | + | + | ? | + |
| Sator-Katzenschlager et al. 2006 Austria97 | + | ? | + | − | + | + | ? | + |
| Liu et al. 2011 China98 | + | + | + | − | + | + | + | − |
| Liu et al. 2014 China99 | + | + | + | − | + | + | + | + |
| Maeda et al. 2013 USA100 | + | ? | + | − | + | + | ? | ? |
| Shi et al. 2011 China101 | + | ? | + | ? | + | + | ? | + |
| Dias et al. 2010 Brazil102 | + | ? | + | ? | + | + | ? | − |
| Zhang et al. 2013 Hong Kong103 | + | ? | + | ? | + | + | ? | + |
| Sangdee et al. 2002 Thailand104 | + | ? | + | − | + | + | ? | + |
| Johansson et al. 2001 Sweden105 | + | + | + | − | + | + | ? | + |
| Hopwood et al. 2008 UK106 | + | + | + | − | + | − | ? | − |
| White et al. 1998 England107 | + | + | + | − | + | − | ? | − |
| Dias et al. 2014 Brazil108 | + | ? | + | − | + | + | ? | − |
| Lin et al. 2013Taiwan109 | + | + | + | − | + | + | ? | + |
| Michalek-Sauberer et al. 2007 Austria110 | + | + | + | − | + | + | ? | − |
| Carlsson and Sjolund 2001 Sweden111 | + | + | + | − | + | + | ? | + |
Note: A, Adequate sequence generation; B, Allocation Concealment; C, Blinding (participants); D, Blinding (personnel); E, Blinding (outcome assessor); F, Incomplete outcome data addressed; G, Free of selective reporting; H, Free of other bias. +, Yes; −, No; ?, Unclear.
Credibility of blinding
Only 24 out of the 94 studies reported the credibility of blinding in participants by conducting the creditability test in six types of sham EA methods. Twenty-three studies22,23,25,34,36,45,52,57,59,60,63,65,72,81,88,97,102,103,105,106,107,108,110 proved to be successful and one study66 proved to be failure. All six types of sham EA methods were claimed to be successful in blinding. They are sham EA type A (10/24 with 1 failure)22,60,66,81,97,102,103,106,108,110, type B (5/24)23,59,65,88,105, type Q (5/24)25,34,36,52,107, sham EA type O (2/24)45,57, sham EA type D (1/24)72, and sham EA type N (1/24)63.
Efficacy results of the included studies
All 94 studies involving 105 comparisons of real and sham EA groups provided the information for between-groups analyses. Among them, 59 real EA groups18,19,21,22,24,28,30,33,34,35,37,38,40,41,42,43,44,48,49,51,53,54,57,59,60,61,62,63,64,65,69,70,71,72,73,75,77,78,79,83,84,86,87,88,90,91,92,94,95,97,99,100,104,108 reported significant superiority over corresponding sham EA groups; forty-three real EA groups were not statistically better than sham EA groups; one study74 showed that sham EA group was superior to the real EA group; the remaining two studies50,111 lacked original data for between-groups analyses and were stated as “T > C?”. The efficacy results of the studies are listed in Table 1 and summarized in Table 3 according to different types of sham EA methods and EA indications.
Compared with sham EA controls, EA therapy in about 56.2% (59/105 comparisons) of comparisons reported the specific effect. Correspondingly, the real EA was superior to sham EA for type N (75%, 3/4 comparisons), type F (71.4%, 5/7 comparisons), type D (66.7%, 4/6 comparisons) and type M (66.7%, 2/3 comparisons). The lowest percentage of positive efficacy result was 44.4% (8/18 comparisons) in sham EA type L. The positive rate of efficacy for the three most often used sham EA methods were 50% (13/26 comparisons) for sham EA type A, 44.4% (8/18 comparisons) for sham EA type L and 64.3% (9/14 comparisons) for sham EA type O.
The type of sham EA methods varied across different EA indications. The sham EA type A was most commonly used in RCTs for pain, anesthesia and osteoarthritis. The sham EA type D and sham EA type Q were applied mainly in stroke studies. The sham EA type B was commonly applied to RCTs on depression. The sham EA type L and sham EA type O were commonly performed in trials on obesity. The sham EA type F and sham EA type L were commonly used in studies on primary dysmenorrhea.
Discussion
To our knowledge, this is the first systematic analysis to address sham EA methods in RCTs. The numbers of publications and sham EA methods have been increasing every decade. We summarized seventeen kinds of sham EA methods according to three aspects as needle location, depth of needle insertion and electrical stimulation, whereas only ten types of sham EA methods were identified from 94 included RCTs involving 6134 participants. The three predominant types of sham EA methods used were sham EA type A, type L and type O ordinally. Only 24 out of 94 trials reported credibility test with the results of 23 success and 1 failure using six types of sham EA methods mainly as follows: sham EA type A (10/24 with 1 failure), type B (5/24) and type Q (5/24). The remaining 3 sham EA methods were only tested in 4 trials. About 56.2% of comparisons provided the evidence of specific effect of EA therapy, and the four types of Sham EA controls with highest positive rate of efficacy result were type N (75%, 3/4 comparisons), type F (71.4%, 5/7 comparisons), type D (66.7%, 4/6 comparisons) and type M (66.7%, 2/3 comparisons) ordinally. However, all types of Sham EA controls were used in a small number of trials. Thus, the evidence was insufficient to recommend any type of sham EA control despite of the high positive rate. The sham EA control was frequently used in RCTs for pain, anesthesia, stroke, depression, obesity and primary dysmenorrheal/menstrual pain, suggesting that these diseases are particularly worthy of further EA RCTs.
The ideal design of sham acupuncture method remains methodologically challenging112. Consequently, a great variety of emerging sham acupuncture methods have found their ways into present RCTs by using non-traditional Chinese medicine acupoint26,27,113, no or superficial penetration29 and no or suboptimal stimulation28. The sham procedures in acupuncture RCTs were previously summarized by He et al.9 as seven types. A previous review by Dincer et al.8 reported the classification of sham acupuncture as sham type I~V based on three respects as needle location, insertion and stimulation. In the present study, we focused on the sham EA methods according to three aspects as needle location, depth of needle insertion and electrical stimulation, and summarized seventeen types of sham EA methods. Ten types of sham EA methods were actually used in the included RCTs.
The main purpose of RCTs on EA is to evaluate its specific effect. An optimal sham acupuncture technique must be biologically inactive and psychologically credible114. A lot of practice has been done to make the sham components of EA less perceptually and operationally distinguishable from real EA intervention for the purpose of keeping the blinding status of the participants. Streitberger needles, blunted needles and verum needles were frequently used with foam, tape or tube for hiding acupuncture loci from subjects18,19,21,22. Furthermore, a pricking sensation was elicited by dull tips for concealing the perceptual differences20,21,23,52,60,63,67,81. The sham EA device was often accompanied by indicator light or with sound signals for confusing the participants18,22,37. In the present study, six types of sham EA method were tested as concealable control in terms of blinding of participants.
The top three types of sham EA methods used were sham EA type A, type L and type O. The most frequently applied sham EA method was type A, accounting for a popular belief in its inertness based on its absence of key EA components as needle stimulation and electrical stimulation as well as its indistinguishable manipulation on same therapeutic acupoints. In the present study, the validation of credible participant blinding of this sham EA type was reported by most credibility tests. The debate emerged over the past decades over the inertness of non-penetrating procedure since the slight acupressure effects and physiological activity might be evoked by the tactile stimulation from blunt needle tips even without skin penetration112,115. Takayama et al.116 argued that non-penetrating placebo needle is at least clinically inert for pain alleviation based on their cross-over study reporting no analgesic effects of the skin-touch placebo needle over that of the no-touch placebo or that of the no-treatment control. However, conclusive evidence are out of our awareness up to now whether non-penetrating but skin-touch placebo needle plays a specific therapeutic role in other medical condition. Thus, the sham EA type A may be an promising candidate control for further RCTs on analgesic effects of EA and relative further researches are called for in aspect of any other conditions.
Sham EA type Q is deemed to be the most inert type of sham EA control because it avoids all therapeutic components, which also probably makes this sham method perceptually and operationally distinguishable from real EA intervention and to some extent results in problematic credibility of blinding in participant. In the present study, the credibility of participant blinding of this sham EA type was endorsed by five studies with credibility test25,34,36,52,107. However, mechanical non-penetration can evoke brain responses in healthy subjects. Thus, controversy raised regarding whether this type of sham EA method is physiologically inert control117. Moreover, four-fifth of the studies were conducted on acupuncture naïve participants. There is a possibility that previous experience of acupuncture treatments might have an impact on present perception of verum and sham EA intervention, which should be rigorously controlled in EA RCTs to avoid bias from unblinding. With the informed consent lack of explicit information on the sham method, debates emerged over ethical acceptability of the study.
The second commonly used sham EA method was type L. It was found that the differential effects of real EA and sham EA, which were attributed to point location, was not consistent across studies and conditions within this sham EA type, suggesting that EA on non-acupoints might be efficacious as EA on therapeutic acupoints. Furthermore, the improvements from baseline were also observed by Sahin et al.26, Li et al.46 and Yu et al.43 The similar findings were previously presented by Moffet et al.118 showing that sham acupuncture at non-acupoints was as efficacious as true acupuncture. It seemed that in the above studies the specificity of acupoints does not exit and to some extent were in violation of traditional acupuncture theories. Li et al.46 stated that the specificity of acupoints was not present in EA treatment. However, Wang et al.79 argued for the specificity of acupoints in EA treatment based on the better effects of EA at acupoints than that at non-acupoints on certain clinical outcomes. From the heterogeneous evidence of acupoint specificity, no definitive conclusion could be drawn based on the paucity of available high-quality clinical trials119. The main issue in this sham EA type might lie in the accurate identification of non-acupoint rather than a rough location nearby traditional acupoint that might be responsible for specific effects, which rises the challenge of conducting appropriate sham control in EA clinical trials especially in the presence or absence of the mechanism of acupoint specificity and the consistency in finding actual point across the different practitioners. Nevertheless, it is unclear whether this type is a concealable control for participant blinding since this sham EA tested credibility in the present study. Therefore, it demonstrates that sham EA type L might not be adequately controlled from inert or concealable perspective only if the mechanisms of acupoints were explicitly explored or the validation of so-called non-acupoint was verified by further researches. Cautions should be taken for eliminating bias from this sham EA control type.
The third commonly used sham EA was type O. During the procedure, the shallow insertion was applied to simulate deep skin penetration and to ensure the blinding of participant. In the present study, the validation of participant blinding of this sham EA type was endorsed by two studies45,57. As for the issue of inertness, a few studies reported that sham EA control improved baseline in certain clinical parameters compared with conventional group32,46,56,57,58. Moffet et al.118 stated that shallow needling at non-acupoints might be as efficacious as real acupuncture. Lund et al.120 reported that minimal acupuncture based on superficial insertion was not a valid control from a physiological perspective. Hróbjartsson et al.121 held the view that sham EA type was not inert control from Chinese medicine perspective. A sham EA procedure with superficial needling at non-acupoints might have subliminal effects since the locations of points was nearby true acupoints or myotome. Moreover, it is likely that the superficial insertion was not consistently applied since the needling depth varied across differentacupoints on different body parts and the relatively deep insertions might be conducted for taking the weight of the attached electrodes. Thus, this sham EA type may be concealable control but far from inert control in RCTs for EA, unless the extent to which the sham procedure could be regarded as physiologically inert has been clarified.
In the present study, six types of sham EA method were reported as successful in blinding. However, further investigations are needed for confirmation, since half of the tested types of sham EA controls were reported in a small number of trials. It should be noted that studies included did not provide sufficient evidence of blinding in acupuncturist. Vase et al.122 stated that it was hard to get acupuncture intervention fully double-blinded. Although non-penetrating needle was previously reported as potential sham control to mask both participants and practitioners in acupuncture research123,124,125, a previous review demonstrated that the acupuncture intervention was not fully double-blinded122. New strategies should be implemented for the development of double-blind sham EA control in terms of both participants and acupuncturists.
RCTs are generally recognized as the gold standard for the efficacy of clinical interventions by excluding the non-specific effect via a placebo control126. However, one study reported that the effect of EA therapy was merely the non-specific effect63. In the present study, the number of real EA group with superiority to, no difference from and inferiority to corresponding sham EA group was 59, 43 and 1, respectively. Thus, more than half comparisons demonstrated that EA therapy existed specific effects. Within all types of sham EA methods, the highest effective rate were type N (75% 3/4 comparisons), type F (71.4%, 5/7 comparisons), type D (66.7%, 4/6 comparisons) and type M (66.7%, 2/3 comparisons) successively. Considering the small number of included studies within corresponding sham EA type, the evidence are still insufficient to recommend any type of sham EA control despite of the high positive rate.
In the present study, 43/105 comparisons reported that EA has no specific effects compared with sham EA controls20,23,24,25,26,27,29,31,32,36,39,43,44,45,46,47,52,55,56,58,63,66,67,68,76,80,81,82,85,89,93,96,98,101,102,103,105,106,107,109,110. For a reason, the extent to which the individual component of EA intervention plays its therapeutic influences on the final outcomes is not clear during clinical treatment7. The debate consequently emerges regarding the therapeutic inactivity of sham EA control which is partially comprised of real EA components, such as suboptimal manual or electrical stimulation110. The probability in the specific effects of EA may be reduced by the potential activity produced by sham EA control. On the other hand, EA is a complex intervention method. Its therapeutic effects consist of specific effects from needling and stimulation components as well as moderately large nonspecific effects, which means that the efficacy results of RCTs for EA are more likely to be influenced by a variety of factors, such as patient/practitioner interaction and patient expectations127,128. In the clinical use, EA may be more effective than manual acupuncture in some situations such as when strong, continued stimulation is required, and when treating pain, anesthesia, stroke, depression, obesity and primary dysmenorrhea/menstrual pain, suggesting that further RCTs with appropriate sham EA control are in need to verify the specific effects on above conditions.
There are several weaknesses in the present study. Firstly, the search and screen procedure were limited to randomized, parallel-controlled trials published in English. Thus, those trials with cross-over design or published in other than English language were omitted. Secondly, with the aim of evaluating the sham method in RCTs on EA, a generous criterion was established to select eligible studies. Therefore, it was not easy to examine the specific effect of EA by data synthesis from different outcomes and indications because of the heterogeneity of trials. Finally, the reported credibility test addressed blinding effects in participant rather than in both participant and acupuncturist. The credibility tests were not reported in all studies and the number of studies using sham EA types was small, and therefore the conclusion should be interpreted with cautions.
Conclusion
Ten types of sham EA methods were identified based on our scheme classification. Generally, sham EA type A, type L and type O were frequently used. Yet, further clinical trials are recommended to maintain standard methodology of concealable and inert placebo EA techniques. Only 24 out of 94 trials were reported as positive credibility test in six types of sham EA methods, where sham EA type A, type B and type Q were highly practiced. It is worthy to study further about the importance of concealable sham EA types. EA therapy in approximately, 56.2% of comparisons provided the specific effects. The four types of sham EA (N, F, D and M respectively) represented the highest positive rate of efficacy results. However, progressive evidences on specific effects are mandatory. The sham EA control was observed frequently in pain, anesthesia, stroke, depression, obesity and primary dysmenorrhea RCTs. Also, broader studies in these predominant diseases are advised.
Additional Information
How to cite this article: Chen, Z. et al. Sham Electroacupuncture Methods in Randomized Controlled Trials. Sci. Rep. 7, 40837; doi: 10.1038/srep40837 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Material
Acknowledgments
This project is supported by grant of the National Natural Science Foundation of China (81573750/81473491/81173395/H2902), the Young and Middle-Aged University Discipline Leaders of Zhejiang Province, China (2013277); Zhejiang Provincial Program for the Cultivation of High-level Health talents (2015).
Footnotes
Author Contributions Z.-X.C., Y.L., X.-G.Z., S.C., W.-T.Y., X.-W.Z. and G.-Q.Z. participated in its design, searched databases, extracted and assessed studies and drafted the manuscript. Z.-X.C., Y.L., X.-G.Z., S.C., W.-T.Y., and X.-W.Z. analyzed data and carried out the statistical analysis. G.-Q.Z. acted as an arbitrator in the review. G.-Q.Z. conceived and designed the article, supervised the study and contributed to finalize the manuscript. All authors reviewed the manuscript.
References
- Medical Research Council (1948). Streptomycin Treatment of Pulmonary Tuberculosis. Br. Med. J. 2, 769–782 (1948). [PMC free article] [PubMed] [Google Scholar]
- Meldrum M. L. A brief history of the randomized controlled trial. From oranges and lemons to the gold standard. Hematol. Oncol. Clin. North. Am. 14, 745–760 (2000). [DOI] [PubMed] [Google Scholar]
- Guidance for Industry Statistical Principles for Clinical Trials ICH Topic E9. (2003). Available at: http://www.hc-sc.gc.ca/dhp-mps/prodpharma/applic-demande/guide-ld/ich/efficac/e9-eng.php#fnb1-ref. (Accessed: 6th November 2015).
- Boutron I. et al. Reporting methods of blinding in randomized trials assessing nonpharmacological treatments. PLoS Med. 4, e61 (2007). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gaw A. C., Chang L. W. & Shaw L. C. Efficacy of acupuncture on osteoarthritic pain. A controlled, double-blind study. N. Engl. J. Med. 293, 375–378 (1975). [DOI] [PubMed] [Google Scholar]
- Hammerschlag R. et al. Randomized Controlled Trials of Acupuncture (1997–2007): An Assessment of Reporting Quality with a CONSORT- and STRICTA-Based Instrument. Evid. Based Complement. Alternat. Med. 2011, 183910 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Langevin H. M. et al. Paradoxes in acupuncture research: strategies for moving forward. Evid. Based Complement. Alternat. Med. 2011, 180805 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dincer F. & Linde K. Sham interventions in randomized clinical trials of acupuncture–a review. Complement. Ther. Med. 11, 235–242 (2003). [DOI] [PubMed] [Google Scholar]
- He W. et al. Review of controlled clinical trials on acupuncture versus sham acupuncture in Germany. J. Tradit. Chin. Med. 33, 403–407 (2013). [DOI] [PubMed] [Google Scholar]
- Zhang C. S., Yang A. W., Zhang A. L., May B. H. & Xue C. C. Sham control methods used in ear-acupuncture/ear-acupressure randomized controlled trials: a systematic review. J. Altern. Complement. Med. 20, 147–161 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu A. J. et al. Electroacupuncture for Acute Ischemic Stroke: A Meta-Analysis of Randomized Controlled Trials. Am. J. Chin. Med. 43, 1541–1566 (2015). [DOI] [PubMed] [Google Scholar]
- Wang W. W., Xie C. L., Lu L. & Zheng G. Q. A systematic review and meta-analysis of Baihui (GV20)-based scalp acupuncture in experimental ischemic stroke. Sci. Rep. 4, 3981 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mayor D. An exploratory review of the electroacupuncture literature: clinical applications and endorphin mechanisms. Acupunct. Med. 31, 409–415 (2013). [DOI] [PubMed] [Google Scholar]
- Fukazawa Y., Maeda T. & Kishioka S. The pharmacological mechanisms of electroacupuncture. Curr. Opin. Investig. Drugs. 10, 62–69 (2009). [PubMed] [Google Scholar]
- Kreiner M., Zaffaroni A., Alvarez R. & Clark G. Validation of a simplified sham acupuncture technique for its use in clinical research: a randomised, single blind, crossover study. Acupunct. Med. 28, 33–36 (2010). [DOI] [PubMed] [Google Scholar]
- Tough E. A., White A. R., Richards S. H., Lord B. & Campbell J. L. Developing and validating a sham acupuncture needle. Acupunct. Med. 27, 118–122 (2009). [DOI] [PubMed] [Google Scholar]
- Lee H. et al. Non-penetrating sham needle, is it an adequate sham control in acupuncture research? Complement. Ther. Med. 19 Suppl 1, S41–48 (2011). [DOI] [PubMed] [Google Scholar]
- Ntritsou V. et al. Effect of perioperative electroacupuncture as an adjunctive therapy on postoperative analgesia with tramadol and ketamine in prostatectomy: a randomised sham-controlled single-blind trial. Acupunct. Med. 32, 215–222 (2014). [DOI] [PubMed] [Google Scholar]
- Chu W. C. et al. Does acupuncture therapy alter activation of neural pathway for pain perception in irritable bowel syndrome?: a comparative study of true and sham acupuncture using functional magnetic resonance imaging. J. Neurogastroenterol. Motil. 18, 305–316 (2012). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang K., Bugge J. & Bugge S. A randomised, placebo-controlled trial of manual and electrical acupuncture for the treatment of tinnitus. Complement. Ther. Med. 18, 249–255 (2010). [DOI] [PubMed] [Google Scholar]
- Zyloney C. E. et al. Imaging the functional connectivity of the Periaqueductal Gray during genuine and sham electroacupuncture treatment. Mol. Pain. 6, 80 (2010). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jubb R. W. et al. A blinded randomised trial of acupuncture (manual and electroacupuncture) compared with a non-penetrating sham for the symptoms of osteoarthritis of the knee. Acupunct. Med. 26, 69–78 (2008). [DOI] [PubMed] [Google Scholar]
- Chung K. F. et al. Randomized non-invasive sham-controlled pilot trial of electroacupuncture for postpartum depression. J. Affect. Disord. 142, 115–121 (2012). [DOI] [PubMed] [Google Scholar]
- Barlas P., Ting S. L., Chesterton L. S., Jones P. W. & Sim J. Effects of intensity of electroacupuncture upon experimental pain in healthy human volunteers: a randomized, double-blind, placebo-controlled study. Pain 122, 81–89 (2006). [DOI] [PubMed] [Google Scholar]
- Wayne P. M. et al. Acupuncture for upper-extremity rehabilitation in chronic stroke: a randomized sham-controlled study. Arch. Phys. Med. Rehabil. 86, 2248–2255 (2005). [DOI] [PubMed] [Google Scholar]
- Sahin N., Ozcan E., Sezen K., Karatas O. & Issever H. Efficacy of acupunture in patients with chronic neck pain–a randomised, sham controlled trial. Acupunct. Electrother. Res. 35, 17–27 (2010). [DOI] [PubMed] [Google Scholar]
- Fanti L. et al. Electroacupuncture analgesia for colonoscopy. a prospective, randomized, placebo-controlled study. Am. J. Gastroenterol. 98, 312–316 (2003). [DOI] [PubMed] [Google Scholar]
- Hsing W. T., Imamura M., Weaver K., Fregni F. & Azevedo Neto R. S. Clinical effects of scalp electrical acupuncture in stroke: a sham-controlled randomized clinical trial. J. Altern. Complement. Med. 18, 341–346 (2012). [DOI] [PubMed] [Google Scholar]
- Gosman-Hedstrom G. et al. Effects of acupuncture treatment on daily life activities and quality of life: a controlled, prospective, and randomized study of acute stroke patients. Stroke 29, 2100–2108 (1998). [DOI] [PubMed] [Google Scholar]
- Jing C. et al. Electro-acupuncture versus sham electro-acupuncture for auditory hallucinations in patients with schizophrenia: a randomized controlled trial. Clin. Rehabil. 23, 579–588 (2009). [DOI] [PubMed] [Google Scholar]
- Kong J. et al. An fMRI study on the interaction and dissociation between expectation of pain relief and acupuncture treatment. NeuroImage 47, 1066–1076 (2009). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Darbandi S. et al. Effects of body electroacupuncture on plasma leptin concentrations in obese and overweight people in Iran: a randomized controlled trial. Altern. Ther. Health Med. 19, 24–31 (2013). [PubMed] [Google Scholar]
- Yang C., An L., Han R., Kang X. & Wang B. Effects of combining electroacupuncture with general anesthesia induced by sevoflurane in patients undergoing supratentorial craniotomy and improvements in their clinical recovery profile & blood enkephalin. Acupunct. Electrother. Res. 37, 125–138 (2012). [DOI] [PubMed] [Google Scholar]
- Liu Y., Liu L. & Wang X. Electroacupuncture at points Baliao and Huiyang (BL35) for post-stroke detrusor overactivity. Neural. Regen. Res. 8, 1663–1672 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang Z. et al. Electroacupuncture at ST36 accelerates the recovery of gastrointestinal motility after colorectal surgery: a randomised controlled trial. Acupunct. Med. 32, 223–226 (2014). [DOI] [PubMed] [Google Scholar]
- Mao J. J. et al. Electroacupuncture for fatigue, sleep, and psychological distress in breast cancer patients with aromatase inhibitor-related arthralgia: a randomized trial. Cancer 120, 3744–3751 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung W. W., Jones A. Y., Ng S. S., Wong C. Y. & Lee J. F. Electroacupuncture in reduction of discomfort associated with barostat-induced rectal distension–a randomized controlled study. J. Gastrointest. Surg. 15, 660–666 (2011). [DOI] [PubMed] [Google Scholar]
- Rusy L. M., Hoffman G. M. & Weisman S. J. Electroacupuncture prophylaxis of postoperative nausea and vomiting following pediatric tonsillectomy with or without adenoidectomy. Anesthesiology 96, 300–305 (2002). [DOI] [PubMed] [Google Scholar]
- Yang M. et al. Electroacupuncture stimulation at sub-specific acupoint and non-acupoint induced distinct brain glucose metabolism change in migraineurs: a PET-CT study. J. Transl. Med. 12, 351 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen H. et al. Electroacupuncture treatment for pancreatic cancer pain: a randomized controlled trial. Pancreatology 13, 594–597 (2013). [DOI] [PubMed] [Google Scholar]
- Quispe-Cabanillas J. G. et al. Impact of electroacupuncture on quality of life for patients with Relapsing-Remitting Multiple Sclerosis under treatment with immunomodulators: a randomized study. BMC Complement. Altern. Med. 12, 209 (2012). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aranha M. F., Muller C. E. & Gaviao M. B. Pain intensity and cervical range of motion in women with myofascial pain treated with acupuncture and electroacupuncture: a double-blinded, randomized clinical trial. Braz. J. Phys. Ther. 19, 34–43 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yu D. T. & Jones A. Y. Physiological changes associated with de qi during electroacupuncture to LI4 and LI11: a randomised, placebo-controlled trial. Acupunct. Med. 31, 143–150 (2013). [DOI] [PubMed] [Google Scholar]
- Li S. et al. Randomized-controlled study of treating attention deficit hyperactivity disorder of preschool children with combined electro-acupuncture and behavior therapy. Complement. Ther. Med. 18, 175–183 (2010). [DOI] [PubMed] [Google Scholar]
- Zheng Z. et al. The effect of electroacupuncture on opioid-like medication consumption by chronic pain patients: a pilot randomized controlled clinical trial. Eur. J. Pain 12, 671–676 (2008). [DOI] [PubMed] [Google Scholar]
- Li G., Li S., Wang B. & An L. The effect of electroacupuncture on postoperative immunoinflammatory response in patients undergoing supratentorial craniotomy. Exp. Ther. Med. 6, 699–702 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lin J. G. et al. The effect of high and low frequency electroacupuncture in pain after lower abdominal surgery. Pain 99, 509–514 (2002). [DOI] [PubMed] [Google Scholar]
- Chen C. Y. et al. The influence of electro-acupuncture stimulation to female constipation patients. Am. J. Chin. Med. 41, 301–313 (2013). [DOI] [PubMed] [Google Scholar]
- Schukro R. P., Heiserer C., Michalek-Sauberer A., Gleiss A. & Sator-Katzenschlager S. The effects of auricular electroacupuncture on obesity in female patients–a prospective randomized placebo-controlled pilot study. Complement. Ther. Med. 22, 21–25 (2014). [DOI] [PubMed] [Google Scholar]
- Yu J. B. et al. Effect of electroacupuncture at Zusanli (ST36) and Sanyinjiao (SP6) acupoints on adrenocortical function in etomidate anesthesia patients. Med. Sci. Monit. 20, 406–412 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xie Y. H., Chai X. Q., Wang Y. L., Gao Y. C. & Ma J. Effect of electro-acupuncture stimulation of Ximen (PC4) and Neiguan (PC6) on remifentanil-induced breakthrough pain following thoracal esophagectomy. J. Huazhong Univ. Sci. Technolog. Med. Sci. 34, 569–574 (2014). [DOI] [PubMed] [Google Scholar]
- Sim C. K., Xu P. C., Pua H. L., Zhang G. & Lee T. L. Effects of electroacupuncture on intraoperative and postoperative analgesic requirement. Acupunct. Med. 20, 56–65 (2002). [DOI] [PubMed] [Google Scholar]
- Song C., Halbreich U., Han C., Leonard B. E. & Luo H. Imbalance between pro- and anti-inflammatory cytokines, and between Th1 and Th2 cytokines in depressed patients: the effect of electroacupuncture or fluoxetine treatment. Pharmacopsychiatry 42, 182–188 (2009). [DOI] [PubMed] [Google Scholar]
- Shafshak T. S. Electroacupuncture and exercise in body weight reduction and their application in rehabilitating patients with knee osteoarthritis. Am. J. Chin. Med. 23, 15–25 (1995). [DOI] [PubMed] [Google Scholar]
- Pastore L. M., Williams C. D., Jenkins J. & Patrie J. T. True and sham acupuncture produced similar frequency of ovulation and improved LH to FSH ratios in women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 96, 3143–3150 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Naslund J., Naslund U. B., Odenbring S. & Lundeberg T. Sensory stimulation (acupuncture) for the treatment of idiopathic anterior knee pain. J. Rehabil. Med. 34, 231–238 (2002). [DOI] [PubMed] [Google Scholar]
- Shen J. et al. Electroacupuncture for control of myeloablative chemotherapy-induced emesis: A randomized controlled trial. J. A. M. A. 284, 2755–2761 (2000). [DOI] [PubMed] [Google Scholar]
- Wyon Y., Wijma K., Nedstrand E. & Hammar M. A comparison of acupuncture and oral estradiol treatment of vasomotor symptoms in postmenopausal women. Climacteric 7, 153–164 (2004). [DOI] [PubMed] [Google Scholar]
- Zhang Z. J. et al. Dense cranial electroacupuncture stimulation for major depressive disorder–a single-blind, randomized, controlled study. PloS One 7, e29651 (2012). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zheng Z. et al. Acupuncture analgesia for temporal summation of experimental pain: a randomised controlled study. Eur. J. Pain 14, 725–731 (2010). [DOI] [PubMed] [Google Scholar]
- Ma Y. X. et al. A comparative study on the immediate effects of electroacupuncture at Sanyinjiao (SP6), Xuanzhong (GB39) and a non-meridian point, on menstrual pain and uterine arterial blood flow, in primary dysmenorrhea patients. Pain Med. 11, 1564–1575 (2010). [DOI] [PubMed] [Google Scholar]
- Wang B. H. et al. Selection of acupoints for managing upper-extremity spasticity in chronic stroke patients. Clin. Interv. Aging 9, 147–156 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yeung W. F. et al. Electroacupuncture for residual insomnia associated with major depressive disorder: a randomized controlled trial. Sleep 34, 807–815 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chan Y. Y. et al. Clinical efficacy of acupuncture as an adjunct to methadone treatment services for heroin addicts: a randomized controlled trial. Am. J. Chin. Med. 42, 569–586 (2014). [DOI] [PubMed] [Google Scholar]
- Man S. C. et al. A pilot controlled trial of a combination of dense cranial electroacupuncture stimulation and body acupuncture for post-stroke depression. BMC Complement. Altern. Med. 14, 255 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oh B. et al. Acupuncture for treatment of arthralgia secondary to aromatase inhibitor therapy in women with early breast cancer: pilot study. Acupunct. Med. 31, 264–271 (2013). [DOI] [PubMed] [Google Scholar]
- Wong R. H. et al. Analgesic effect of electroacupuncture in postthoracotomy pain: a prospective randomized trial. Ann. Thorac. Surg. 81, 2031–2036 (2006). [DOI] [PubMed] [Google Scholar]
- Song Y., Zhou D., Fan J., Luo H. & Halbreich U. Effects of electroacupuncture and fluoxetine on the density of GTP-binding-proteins in platelet membrane in patients with major depressive disorder. J. Affect. Disord. 98, 253–257 (2007). [DOI] [PubMed] [Google Scholar]
- Cameron I. D., Wang E. & Sindhusake D. A randomized trial comparing acupuncture and simulated acupuncture for subacute and chronic whiplash. Spine 36, E1659–1665 (2011). [DOI] [PubMed] [Google Scholar]
- Darbandi M. et al. Auricular or body acupuncture: which one is more effective in reducing abdominal fat mass in Iranian men with obesity: a randomized clinical trial. J. Diabetes Metab. Disord. 13, 92 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wei L., Wang H., Han Y. & Li C. Clinical observation on the effects of electroacupuncture at Shaoze (SI 1) in 46 cases of postpartum insufficient lactation. J. Tradit. Chin. Med. 28, 168–172 (2008). [DOI] [PubMed] [Google Scholar]
- Wang S. M., Punjala M., Weiss D., Anderson K. & Kain Z. N. Acupuncture as an adjunct for sedation during lithotripsy. J. Altern. Complement. Med. 13, 241–246 (2007). [DOI] [PubMed] [Google Scholar]
- Kvorning N., Christiansson C. & Akeson J. Acupuncture facilitates neuromuscular and oculomotor responses to skin incision with no influence on auditory evoked potentials under sevoflurane anaesthesia. Acta Anaesthesiol. Scand. 47, 1073–1078 (2003). [DOI] [PubMed] [Google Scholar]
- Kvorning N., Christiansson C., Beskow A., Bratt O. & Akeson J. Acupuncture fails to reduce but increases anaesthetic gas required to prevent movement in response to surgical incision. Acta Anaesthesiol. Scand. 47, 818–822 (2003). [DOI] [PubMed] [Google Scholar]
- Yang L. et al. Cardioprotective effects of electroacupuncture pretreatment on patients undergoing heart valve replacement surgery: a randomized controlled trial. Ann. Thorac. Surg. 89, 781–786 (2010). [DOI] [PubMed] [Google Scholar]
- Sahmeddini M. A., Farbood A. & Ghafaripuor S. Electro-acupuncture for pain relief after nasal septoplasty: a randomized controlled study. J. Altern. Complement. Med. 16, 53–57 (2010). [DOI] [PubMed] [Google Scholar]
- Wang W. et al. Study on the regulatory effect of electro-acupuncture on hegu point (LI4) in cerebral response with functional magnetic resonance imaging. Chin. J. Integr. Med. 13, 10–16 (2007). [DOI] [PubMed] [Google Scholar]
- Jia C. S. et al. Electroacupuncture at Qiuxu (GB 40) for treatment of migraine–a clinical multicentral random controlled study. J. Tradit. Chin. Med. 29, 43–49 (2009). [DOI] [PubMed] [Google Scholar]
- Wang Y. et al. Electroacupuncture for moderate and severe benign prostatic hyperplasia: a randomized controlled trial. PloS One 8, e59449 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andreescu C., Glick R. M., Emeremni C. A., Houck P. R. & Mulsant B. H. Acupuncture for the treatment of major depressive disorder: a randomized controlled trial. J. Clin. Psychiatry 72, 1129–1135 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yeung W. F., Chung K. F., Zhang S. P., Yap T. G. & Law A. C. Electroacupuncture for primary insomnia: a randomized controlled trial. Sleep 32, 1039–1047 (2009). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen W. T., Chang F. C., Chen Y. H. & Lin J. G. An Evaluation of Electroacupuncture at the Weizhong Acupoint (BL-40) as a Means of Relieving Pain Induced by Extracorporeal Shock Wave Lithotripsy. Evid. Based Complement. Alternat. Med. 2014, 592319 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang C. P., Kao C. H., Chen W. K., Lo W. Y. & Hsieh C. L. A single-blinded, randomized pilot study evaluating effects of electroacupuncture in diabetic patients with symptoms suggestive of gastroparesis. J. Altern. Complement. Med. 14, 833–839 (2008). [DOI] [PubMed] [Google Scholar]
- Meissner W. et al. Acupuncture decreases somatosensory evoked potential amplitudes to noxious stimuli in anesthetized volunteers. Anesth. Analg. 98, 141–147 (2004). [DOI] [PubMed] [Google Scholar]
- Zhou S. et al. Bilateral effects of 6 weeks’ unilateral acupuncture and electroacupuncture on ankle dorsiflexors muscle strength: a pilot study. Arch. Phys. Med. Rehabil. 93, 50–55 (2012). [DOI] [PubMed] [Google Scholar]
- Yeh B. Y. et al. Effect of electroacupuncture in postanesthetic shivering during regional anesthesia: a randomized controlled trial. BMC Complement. Altern. Med. 12, 233 (2012). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yu J. S., Shen K. H., Chen W. C., Her J. S. & Hsieh C. L. Effects of electroacupuncture on benign prostate hyperplasia patients with lower urinary tract symptoms: a single-blinded, randomized controlled trial. Evid. Based Complement. Alternat. Med. 2011, 303198 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ma W. et al. Effects of Sanyinjiao (SP6) with electroacupuncture on labour pain in women during labour. Complement. Ther. Med. 19 Suppl 1, S13–18 (2011). [DOI] [PubMed] [Google Scholar]
- Li G., Li S., An L. & Wang B. Electroacupuncture alleviates intraoperative immunosuppression in patients undergoing supratentorial craniotomy. Acupunct. Med. 31, 51–56 (2013). [DOI] [PubMed] [Google Scholar]
- Deluze C., Bosia L., Zirbs A., Chantraine A. & Vischer T. L. Electroacupuncture in fibromyalgia: results of a controlled trial. B. M. J. 305, 1249–1252 (1992). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ng S. S. et al. Electroacupuncture reduces duration of postoperative ileus after laparoscopic surgery for colorectal cancer. Gastroenterology 144, 307–313.e301 (2013). [DOI] [PubMed] [Google Scholar]
- Lee S. H. & Lee B. C. Electroacupuncture relieves pain in men with chronic prostatitis/chronic pelvic pain syndrome: three-arm randomized trial. Urology 73, 1036–1041 (2009). [DOI] [PubMed] [Google Scholar]
- Tam L. S., Leung P. C., Li T. K., Zhang L. & Li E. K. Acupuncture in the treatment of rheumatoid arthritis: a double-blind controlled pilot study. BMC Complement. Altern. Med. 7, 35 (2007). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kvorning N. & Akeson J. Plasma adrenaline increases in anesthetized patients given electro-acupuncture before surgery. Pain Med. 11, 1126–1131 (2010). [DOI] [PubMed] [Google Scholar]
- Waite N. R. & Clough J. B. A single-blind, placebo-controlled trial of a simple acupuncture treatment in the cessation of smoking. Br. J. Gen. Pract. 48, 1487–1490 (1998). [PMC free article] [PubMed] [Google Scholar]
- Holzer A. et al. Auricular acupuncture for postoperative pain after gynecological surgery: a randomized controlled trail. Minerva Anestesiol. 77, 298–304 (2011). [PubMed] [Google Scholar]
- Sator-Katzenschlager S. M. et al. Auricular electro-acupuncture as an additional perioperative analgesic method during oocyte aspiration in IVF treatment. Hum. Reprod. 21, 2114–2120 (2006). [DOI] [PubMed] [Google Scholar]
- Liu C. Z. et al. Immediate analgesia effect of single point acupuncture in primary dysmenorrhea: a randomized controlled trial. Pain Med. 12, 300–307 (2011). [DOI] [PubMed] [Google Scholar]
- Liu C. Z. et al. A randomized controlled trial of single point acupuncture in primary dysmenorrhea. Pain Med. 15, 910–920 (2014). [DOI] [PubMed] [Google Scholar]
- Maeda Y. et al. Acupuncture-evoked response in somatosensory and prefrontal cortices predicts immediate pain reduction in carpal tunnel syndrome. Evid. Based Complement. Alternat. Med. 2013, 795906 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shi G. X. et al. Effects of acupuncture at Sanyinjiao (SP6) on prostaglandin levels in primary dysmenorrhea patients. Clin. J. Pain 27, 258–261 (2011). [DOI] [PubMed] [Google Scholar]
- Dias M. et al. Effects of electroacupuncture on local anaesthesia for inguinal hernia repair: a randomised placebo-controlled trial. Acupunct. Med. 28, 65–70 (2010). [DOI] [PubMed] [Google Scholar]
- Zhang S. P., Chiu T. T. & Chiu S. N. Long-term efficacy of electroacupuncture for chronic neck pain: a randomised controlled trial. Hong Kong Med. J. 19 Suppl 9, 36–39 (2013). [PubMed] [Google Scholar]
- Sangdee C. et al. Electroacupuncture versus diclofenac in symptomatic treatment of osteoarthritis of the knee: a randomized controlled trial. BMC Complement. Altern. Med. 2, 3 (2002). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johansson B. B. et al. Acupuncture and transcutaneous nerve stimulation in stroke rehabilitation: a randomized, controlled trial. Stroke 32, 707–713 (2001). [DOI] [PubMed] [Google Scholar]
- Hopwood V., Lewith G., Prescott P. & Campbell M. J. Evaluating the efficacy of acupuncture in defined aspects of stroke recovery: a randomised, placebo controlled single blind study. J. Neurol. 255, 858–866 (2008). [DOI] [PubMed] [Google Scholar]
- White A. R., Resch K. L. & Ernst E. Randomized trial of acupuncture for nicotine withdrawal symptoms. Arch. Intern. Med. 158, 2251–2255 (1998). [DOI] [PubMed] [Google Scholar]
- Dias M., Vellarde G. C., Olej B., Teofilo Salgado A. E. & de Barros Rezende I. Effects of electroacupuncture on stress-related symptoms in medical students: a randomised placebo-controlled study. Acupunct. Med. 32, 4–11 (2014). [DOI] [PubMed] [Google Scholar]
- Lin R. T. et al. Electroacupuncture and rosiglitazone combined therapy as a means of treating insulin resistance and type 2 diabetes mellitus: a randomized controlled trial. Evid. Based Complement. Alternat. Med. 2013, 969824 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michalek-Sauberer A. et al. Perioperative auricular electroacupuncture has no effect on pain and analgesic consumption after third molar tooth extraction. Anesth. Analg. 104, 542–547 (2007). [DOI] [PubMed] [Google Scholar]
- Carlsson C. P. & Sjolund B. H. Acupuncture for chronic low back pain: a randomized placebo-controlled study with long-term follow-up. Clin. J. Pain 17, 296–305 (2001). [DOI] [PubMed] [Google Scholar]
- Lund I. & Lundeberg T. Are minimal, superficial or sham acupuncture procedures acceptable as inert placebo controls? Acupunct. Med. 24, 13–15 (2006). [DOI] [PubMed] [Google Scholar]
- Bäcker M. et al. Acupuncture in migraine: investigation of autonomic effects. Clin. J. Pain 24, 106–115 (2008). [DOI] [PubMed] [Google Scholar]
- Vickers A. J. Placebo controls in randomized trials of acupuncture. Eval. Health Prof. 25, 421–435 (2002). [DOI] [PubMed] [Google Scholar]
- Lundeberg T., Lund I., Näslund J. & Thomas M. The Emperors sham - wrong assumption that sham needling is sham. Acupunct. Med. 26, 239–242 (2008). [DOI] [PubMed] [Google Scholar]
- Takayama M. et al. Is Skin-Touch Sham Needle Not Placebo? A Double-Blind Crossover Study on Pain Alleviation. Evid. Based Complement. Alternat. Med. 2015, 152086 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dhond R. P., Witzel T., Hämäläinen M., Kettner N. & Napadow V. Spatiotemporal mapping the neural correlates of acupuncture with MEG. J. Altern. Complement. Med. 14, 679–688 (2008). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moffet H. H. Sham acupuncture may be as efficacious as true acupuncture: a systematic review of clinical trials. J. Altern. Complement. Med. 15, 213–216 (2009). [DOI] [PubMed] [Google Scholar]
- Zhang H., Bian Z. & Lin Z. Are acupoints specific for diseases? A systematic review of the randomized controlled trials with sham acupuncture controls. Chin. Med. 5, 1 (2010). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lund I., Naslund J. & Lundeberg T. Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: a physiologist’s perspective. Chin. Med. 4, 1 (2009). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hrobjartsson A. & Gotzsche P. C. Placebo interventions for all clinical conditions. Cochrane Database Syst. Rev. 1, CD003974 (2010). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vase L. et al. Can acupuncture treatment be double-blinded? An evaluation of double-blind acupuncture treatment of postoperative pain. PLoS One 10, e0119612 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Takakura N., Takayama M., Kawase A. & Yajima H. Double blinding with a new placebo needle: a validation study on participant blinding. Acupunct. Med. 29, 203–207 (2011). [DOI] [PubMed] [Google Scholar]
- Takakura N. & Yajima H. A double-blind placebo needle for acupuncture research. BMC Complement. Altern. Med. 7, 31 (2007). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Takakura N., Takayama M., Kawase A., Kaptchuk T. J. & Yajima H. Double-blind acupuncture needle: a potential tool to investigate the nature of pain and pleasure. ISRN Pain 2013 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meldrum M. L. A brief history of the randomized controlled trial. From oranges and lemons to the gold standard. Hematol. Oncol. Clin. North Am. 14, 745–760 (2000). [DOI] [PubMed] [Google Scholar]
- Linde K., Niemann K., Schneider A. & Meissner K. How large are the nonspecific effects of acupuncture? A meta-analysis of randomized controlled trials. BMC Med. 8, 75 (2010). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaptchuk T. J. et al. Components of placebo effect: randomised controlled trial in patients with irritable bowel syndrome. B. M. J. 336, 999–1003 (2008). [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.