

Abstract
INTRODUCTION:
Bicycling is one of the most enjoyable aerobic exercises recommended for the promotion of an individual's health. The Eastern Province of Saudi Arabia has seen a huge increase in the number of people who cycle. People have different goals for bicycling, but the injuries they sustain are common. Most of them relate to overuse, particularly of lower body joints. This study was conducted to determine the prevalence of knee problems and factors associated with knee pain in cyclists.
MATERIALS AND METHODS:
A cross-sectional study was conducted in October 2015, using an online self-administered questionnaire. The questionnaire was based on pertinent literature, was piloted, and validated. A web link was sent to 513 cyclists (professional and amateur) using E-mail, WhatsApp application, or SMS. Three hundred and eleven responses were received, 283 of which were included in the analysis.
RESULTS:
The overall prevalence of knee pain was 25.8%; 27.6% for amateur cyclists and 15.9% for professional cyclists. Only 17.2% knee pain was attributed to cycling, whereas in 32.8% it happened spontaneously and in 25% of cases it occurred while running. Majority of the cyclists reported pain as mild (61.6%) or moderate (28.7%); anterior knee pain accounted for 58.1% knee pain. Different goals of cycling and different bicycle types had statistically significant difference on the rate of knee pain. Of underweight cyclists, 62.2% reported knee pain. Cyclists who run more or participated in football had a higher rate of pain.
CONCLUSION:
Knee injuries are common with cyclists. Factors such as the type of the bicycle, the goal of bicycling, club type, body mass index, and participation in other sports play a significant role in the rate of knee pain.
Key words: Amateur, bicycling injuries, characteristics, knee injuries, knee pain, professional, Saudi Arabia, severity, sport injuries
Introduction
Bicycling is becoming increasingly popular as a sport worldwide. It has grown very rapidly, of late, in Saudi Arabia. Some cyclists use the bicycle as a means of transportation, others ride for recreation, and some are competitive cyclists. The repetitive movements of cycling put cyclists at a risk of overuse injuries, particularly to the leg joints (knee and ankle).[1] During 1985, about 8.36% of causalities seen in the Emergency Room of King Fahd Hospital of the University were sports related, and knee injuries accounted for 24% of those injuries.[2]
In a cross-sectional study of 224 recreational cyclists in California in1995 using mailed surveys, 85% of the cyclists reported one or more overuse injuries, 36% of which required medical attention. Knee injury accounted for 41.7% of those injuries (35.4% prevalence). Miles/week, lower number of gears, and low level of experience were associated with increased prevalence.[3] The study by Zwingenberger et al. also suggested that low experience level was associated with increased prevalence of injury.[4]
In a study by Silberman in New Jersey in professional road cyclists, 94% of them had experienced at least one overuse injury in the preceding 12 months; knee was the most common site. Many injuries were mild, resulting in limited time off the bike.[5] In another study by Clarsen et al. among seven professional teams in the USA, involving 109 professional cyclists, the prevalence of knee overuse injury was 23% and most likely resulted in time loss.[6]
Vleck and Garbutt studied the prevalence of knee injury among elite triathletes in the UK. Nearly 75% of them had overuse injury, and knee injuries accounted for 14.2%-21.9% of the injuries. Almost 62.1% of the knee injuries occurred during running and 34.5% occurred during cycling.[7] In a study conducted in London on military personnel undergoing a fitness test, it was found that obesity was associated with the increased incidence of musculoskeletal injury.[8]
Many studies suggest that the bike fit and alignment, lack of training, and inappropriate equipment are major contributory factors and that efforts should be made to control these factors to reduce the prevalence of overuse injuries and reduce time off training.[1,5,9,10,11]
The outcome of a randomized controlled trial (RCT) was favorable with respect to strengthening and stretching exercises in preventing anterior knee pain (AKP).[12] However, a systematic review showed a marked reduction (50%) in overuse injury by means of strengthening exercises, but, stretching exercises did not show any benefit.[13]
Despite the increasing popularity of cycling, to the best of our knowledge, there have been no published epidemiological studies in Saudi Arabia, and indeed, few studies have been published worldwide that describe the prevalence of knee problems of cyclists and the associated risk factors. This study was conducted to assess the prevalence and the magnitude of knee pain and other knee problems of active cyclists in the Eastern Province and to determine the factors associated with knee pain in the study population.
Materials and Methods
A cross-sectional study was conducted to assess the prevalence, magnitude, and associated factors of knee pain of active cyclists in the Eastern Province, Saudi Arabia, in 2015. The study population included all active cyclists who were members of a recognized professional or amateur cycling club in the Eastern Province of Saudi Arabia. An online link to the questionnaire was sent to 513 cyclists, 311 of whom completed the questionnaire, giving a response rate of 60.62%.
The following inclusion criteria were then used: (1) Minimum age of 18 years; (2) should have been bicycling for ≥6 months; (3) and should ride the bicycle at least once per week. The data were collected using a structured, self-administered questionnaire which had been designed by the researchers after reviewing the literature and similar questionnaires based on the objectives of the study.
The questionnaire consisted of seven parts: (1) Sociodemographic data: Age, gender, nationality, level of education, marital status, and club name; (2) chronic medical illnesses that may affect the sport or predispose to knee symptoms, smoking, height and weight; (3) participation in sport: Goal, experience, frequency, duration, warm up, stretching exercises, strengthening exercises, and rest days; (4) type of bicycle used, bicycle fitting, and clip-less pedal; (5) current knee pain and pain in the past 12 months, frequency, precipitating event, site, and associated symptoms and management.
A frequency scale comprising always, often, sometimes, seldom, and never was used. A 0–10 pain scale was used to assess severity. We tested six types of bicycles: Road bicycle (a bicycle built for traveling at speed on paved roads, time trial bicycle (a racing bicycle designed for use by an individual or team time trials on roads), mountain bicycle (a bicycle created for off-road cycling), hybrid bicycle (a blend of characteristics of a road bicycle and a mountain bicycle), and the recumbent bicycle (a bicycle on which the rider is in a laid-back position).[14]
The questionnaire was designed by the researchers, validated by four faculty, and piloted on forty cyclists (different from the target group). Based on the results, some linguistic and technical modifications were made. The questionnaire was then reviewed by the researcher and two faculty members after modification. The study was approved by the Ethical Committee of Postgraduate Saudi Board Program, Eastern Province.
All participants were sent an invitation explaining the purpose of the study, reassuring them of confidentiality and a web link to the survey in October 2015. SMS, WhatsApp application, and E-mail were used to deliver the invitations to the participants. Reminders were sent every week for 3 weeks. Completion and return of the questionnaire was considered as assent to participation in the study. Returned questionnaire that did not meet the inclusion criteria were excluded, giving a total of 283 valid questionnaires. The data were coded, entered, and analyzed using Statistical Package for Social Sciences (SPSS) version 20.0 (released in 2011 by IBM Corp., Armonk, NY).
Cyclists were classified into two groups: Professional (competitive cyclists who are registered in the Saudi Cycling Federation) and amateur (unpaid cyclists not under the umbrella of the Saudi Cycling Federation). The term “bicycle fitting” was used for a process whereby an expert adjusts the bicycle dimensions to suit those of the cyclist's body. The term “clip-less pedal” was a system comprising special pedals and cleats, devices on the pedals that attach to the soles of clip-less cycling shoes.[15] The term “triathlon” is used for a multiple-stage competition involving swimming, cycling, and running in immediate succession over various distances.[16]
Body mass index (BMI) was classified into six categories according to the World Health Organization classification: <18.5 as underweight, 18.5–24.9 as normal weight, 25–29.9 as overweight, 30–34.9 as obesity Class I, 35–39.9 as obesity Class II, and ≥40 as obesity class III. The Numeric Rating Scale (11) was used to categorize pain: mild (1–3), moderate (4–6), and severe (7–10). Age was classified into four groups: teenage (18–19.99), young adult (20–39.99), middle aged (40–64.99), and elderly (≥65).
Data were presented using descriptive statistics in the form of frequencies and percentages for categorical variables and mean and standard deviation for quantitative variables. Chi-square test was used to test for association. Mann-Whitney test was used to compare median ranks between different pain category groups.
Results
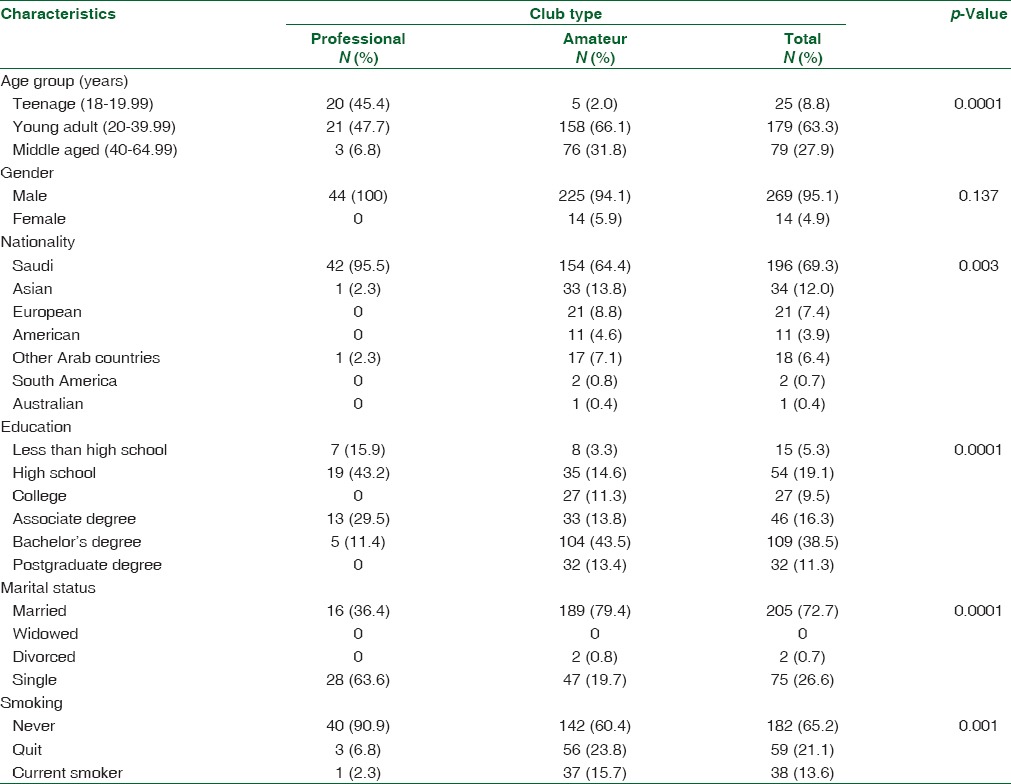
Out of 513, a total of 311 cyclists responded to the survey (60.6% response rate). Only 283 respondents met the inclusion criteria and were included in the analyses. Majority of the participants were male (95.1%), and young adults (63.3%). Teenagers constituted 45.4% of the professional teams and 2% of the amateur teams (P = 0.0001). Almost two-thirds (69.3%) were Saudi, 12% were Asians, while the remainder were of various other nationalities. Half of them had a bachelor's degree or higher, and about three-fourths (72.7%) were married.
Concerning smoking, 13.6% of the participants smoked tobacco products, 21.1% had quit, and 65.2% had never smoked. Amateur cyclists had higher smoking rates (15.7%) compared to professional cyclists (2.3%) (P = 0.001) [Table 1].
Table 1.
Distribution of active cyclists according to sociodemographic characteristics, Eastern Province, Saudi Arabia, 2015.
The overall prevalence of knee pain was 25.8%. The second most common symptom in relation to the knee joint was popping (6.7%) followed by swelling of the knee (5.0%). The 12-month prevalence of knee pain was higher in amateur cyclists (27.6%) compared to professional cyclists (15.9%), but that was not statistically significant [Figure 1].
Figure 1.
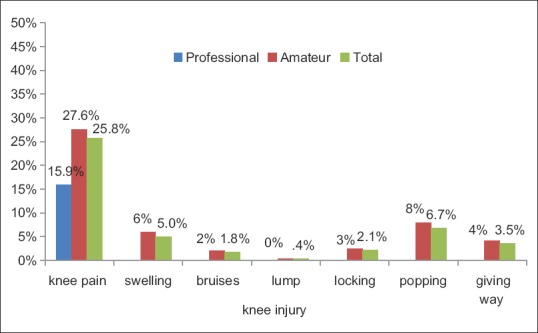
Distribution of knee symptoms among active cyclists by club type, Eastern Province, Saudi Arabia, 2015
The distribution did not statistically vary among the different studied sociodemographic categories or smoking status.
As regards cyclists with knee pain, 39.7% of the cyclists seldom experienced knee pain, 39.7% experienced it sometimes, while almost 18.5% often or always experienced knee pain. Knee pain occurred spontaneously with no obvious cause in 32.8% of cases, for 25%, it was precipitated by running, and for 17.2%, it was precipitated by cycling. Anterior aspect of the knee was the most common location of the pain, accounting for 58.1%; 21% were above the patella, 27.4% were below the patella, and 9.7% were behind the patella [Table 2].
Table 2.
Characteristics of the knee pain among active cyclists, Eastern Province, Saudi Arabia, 2015. (n=75)
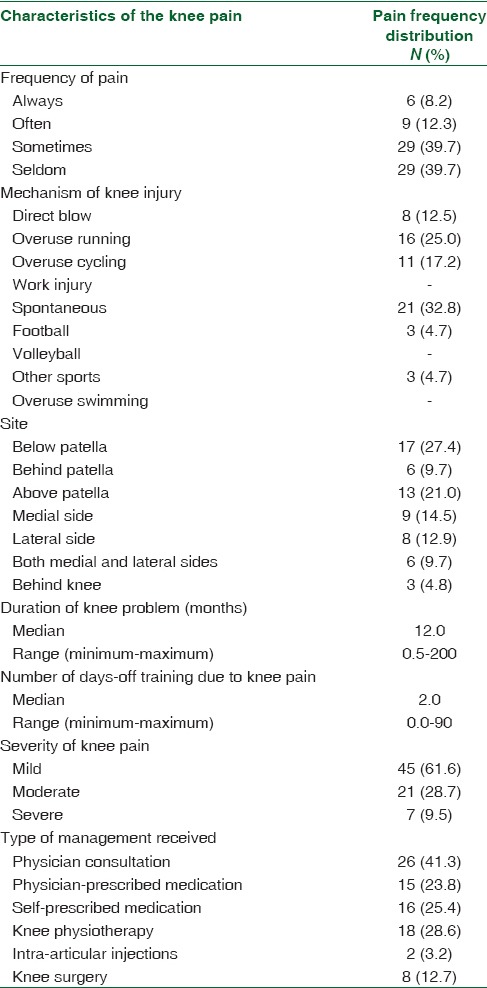
The average duration of knee pain was 12 months that was higher than other knee symptoms such as swelling, locking, popping, and giving way. The average days-off training because of the knee problems was 2 days. Swelling and the presence of a lump were associated with a higher average of days-off training. More than half (61.6%) of knee pain was mild, 28.7% was moderate, and 9.5% was severe pain [Table 2].
Of cyclists with knee pain, only 41.3% consulted a physician for the problem. The rate increased when there was an associated symptom with the knee pain. About half of those with knee pain (49.2%) used medications for their pain, 28.6% underwent physiotherapy, and 12.7% underwent knee surgery. Only two cases (3.17%) had an intra-articular injection [Table 2].
The highest prevalence of knee pain was found in road racers (50%) followed by cyclists who rode for fitness and weight loss (29.2%). The lowest prevalence of knee pain was found in those who used cycling as a mean of transportation (16.7%) (P = 0.020) [Table 3].
Table 3.
Frequency distribution of various cycling and other sports-related factors among active cyclists by knee pain, Eastern Province, Saudi Arabia, 2015.
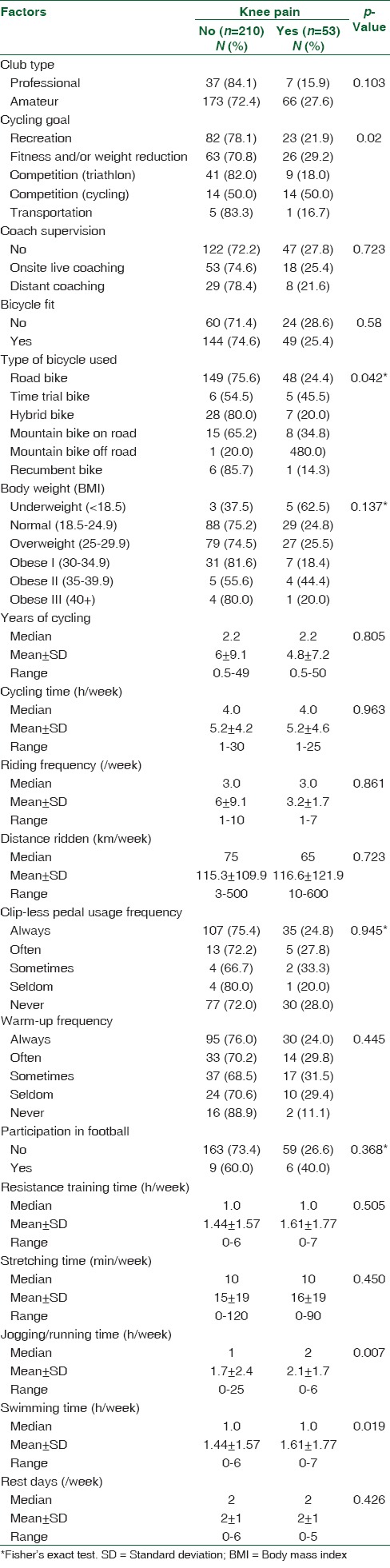
The distribution was much higher among cyclists who used to ride mountain bikes off road (80%), followed by those who used to ride time trial bikes (45.5%) and cyclists who rode mountain bikes on road (34.8%). The lowest prevalence of knee pain was found in those who rode recumbent bikes (14.3%) (P = 0.042) [Table 3].
The prevalence was higher in underweight cyclists (62.5%) and surprisingly lower in obese cyclists (23%), but this was not statistically significant (P = 0.137). The prevalence was higher in cyclists who participated in football games (40%) compared to cyclists who did not (26.6%) (P = 0.368) [Table 3].
The average jogging hours was higher among cyclists with knee pain (2 h) compared to cyclists who had no knee pain (1 h) (P = 0.007). Moreover, the average of swimming hours among cyclists with knee pain was higher as well (1 h) (P = 0.019) [Table 3].
When preventive measures were tested, there were no statistically significant differences between cyclists with knee pain and cyclists with no knee pain. The measures included a professional bike fit, coach supervision, clip-less pedal usage, warm up, strength training, and stretching exercises [Table 3].
There was no statistically significant difference in the average of years of cycling, cycling hours per week, riding frequency per week, kilometers ridden per week, and rest days between cyclists who had knee pain and cyclists who had no knee pain [Table 3].
Discussion
Knee pain, common in active cyclists in the Eastern Province of Saudi Arabia, has an overall 12-month prevalence of 25.8%. Professional cyclists had a lower prevalence of knee pain than the amateur cyclists, suggesting that experience is protective. However, the results show no difference in the average years of the experience. Professional cyclists undergo a high-quality bike fitting on a regular basis and get trained under direct coach supervision, in which an emphasis is put on the correct technique necessary in preventing injuries. Berkovich et al. also posited the importance of coaching techniques in preventing knee injuries in cyclists.[1]
Many researchers have also suggested that the appropriate bicycle configuration and saddle height are protective.[9,11] However, the results of this study did not show any difference in the prevalence of injury between cyclists who had a professional bike fit and cyclists who did not.
The 12-month prevalence in amateur cyclists of this study was higher than the 18-month prevalence in the UK adventure racing cyclists (21.9%).[17] This is probably because the cyclists in the UK were more physically fit and experienced, based on years of cycling. The 12-month prevalence was higher in Japanese triathletes (33.0%),[18] but lower than what was found in recreational cyclists in California (41.7%).[3]
The prevalence of knee pain in this study was higher than the prevalence in the residents of Al-Qassim, the KSA, with clinical knee osteoarthritis (13%),[19] but close to the prevalence of knee pain for non-Hispanic and Mexican-American males aged 60–74 years (26.1%).[20]
Most cyclists attributed their knee pain to causes other than bicycling itself; only 17.2% thought that their pain was due to cycling. This is close to the conclusion drawn by Deakon, which imputed 20% of injuries during triathlon to cycling.[10] This is because bicycling is a low-impact sport. A large percentage of injuries occurred spontaneously (32.8%), suggesting insidious causes of knee pain rather than acute injuries. Many cyclists attributed their knee pain to running (25.0%). This conclusion is supported by the fact that the average running time was double in cyclists with knee pain. Vleck and Garbutt concluded that injuries that occur during running were almost twice than those of injuries that occur during the bicycling part of the triathlon events.[7] Zwingenberger also concluded that running was associated with more injuries during triathlon events.[4]
The most common site of the knee pain was anterior knee (58.1%). AKP affected 14.9% of cyclists in this study compared to 36% of the USA professional cyclists as described by Clarsen et al.[6] This suggests that patellofemoral pain syndrome, patellar tendenopathy, patella chondromalacia, fat pad impingement, or patellar bursitis are the possible etiologies of the knee pain in the studied population.[5,21,22,23] By the same token, the average duration was 12 months, suggesting that the most likely causes were chronic. Most knee pains were mild or moderate (62.1% and 28.8%; respectively) and were not frequent; more serious injuries were most likely to be associated with more severe and frequent pain. Nevertheless, 41.3% of the cyclists consulted physicians. This percentage is higher than the findings by Clarsen et al. (19.0%)[6] and Wilber (36%).[3] About half of them used medications and 28.6% underwent physiotherapy. Only a small percentage needed surgery or an intra-articular injection (12.7% and 3.2%, respectively).
The highest prevalence of knee pain (50.0%) was in road racers, but the lowest was in commuters (16.7%), suggesting that the volume and intensity of training are the important risk factors for knee pain. However, there were no differences in the average bicycling hours per week, kilometers ridden per week, riding times per week, or rest days per week, which means that high-intensity training was a key factor. Contrary to the conclusion drawn by Fordham et al., there is a positive correlation between the hours spent cycling per week and rest days per week and the number of injuries.[17] Moreover, there was a relatively higher prevalence in cyclists who rode for fitness and weight loss. This may be explained by the low fitness level and high BMI of this group of cyclists as suggested by Taanila et al.[24,25,26]
In this study, warm up, strength training, and stretching exercises did not show a significant difference on the prevalence of knee pain. However, an RCT by Coppack et al. showed that strength and stretching exercises reduced the incidence of AKP by 75%. A systematic review by Herman et al. also showed that proper neuromuscular warm-up strategies decreased the risk of injury.[27] A systematic review showed that strengthening is protective but stretching is not.[13]
Prevalence in underweight cyclists (62.5%) was higher than obese and normal weight cyclists. This confirms the finding that being underweight was a risk factor of musculoskeletal overuse injuries.[26] The rate of greater knee pain was not higher in the obese than in those with normal weight. However, Cowan et al. and Taanila et al. suggested that obesity was associated with increased risk of musculoskeletal injuries in military trainees.[8,26]
Smoking rate among amateur cyclists (15.7%) was higher than what prevailed in the general population of Saudi Arabia (12.2%).[28] Though it was not associated with higher rate of knee pain in this study, it is well documented that smoking increased the risk for musculoskeletal injuries.[29,30]
We recommend clinical trials to evaluate the effect of the above-mentioned preventive measures on performance and injuries. There should be an annual survey to assess injury patterns, especially among professional cyclists. Clinicians should be involved in increasing the awareness of the importance of bike fit, proper cycling and running techniques, and the right fit of footwear. Emphasis should also be put on the importance of cessation of smoking, the maintenance of ideal body weight, and the avoidance of over training.
The data were collected using a self-administered questionnaire, which may have been subject to recall bias. There may have been nonresponse bias as response rate was low (60.6%). A simple short survey was used for preventive measures, but a prospective study is necessary for a better assessment. The number of cyclists in Saudi Arabia is still low. Therefore, the study population was low. Nevertheless, this first study of the population surveyed has highlighted the problem of knee pain in cyclists in Saudi Arabia and emphasized the need for health education about this problem and ways to prevent injuries.
Conclusion
Knee pain was common in our study population, especially in amateur cyclists. Most of the pain noted was mild and moderate AKP. Running, football participation, and being underweight were associated with higher rates of knee pain. The rate of knee pain in road racers and mountain cyclists was higher, probably because their knees were susceptible to overuse. There was no association with bicycle fitting, coaching, using clip-less pedals, warming up average years of cycling, average distance ridden in a week, resistance training, strength training, and average rest days in a week.
The study underpins the importance of ensuring that athletes use the appropriate technique in cycling, running, and swimming, use appropriate footwear, and ensure that the increase in the training load is gradual in trial to prevent knee pain in cyclists, especially amateur cyclists.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Berkovich Y, Nierenberg G, Falah M, Soudry M. Knee injury in cyclers. Harefuah. 2010;149:726–8, 748. [PubMed] [Google Scholar]
- 2.Sadat-Ali M, Sankaran-Kutty M. Sports injuries in Saudi Arabia. Br J Sports Med. 1985;19:28–9. doi: 10.1136/bjsm.19.1.28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wilber CA, Holland GJ, Madison RE, Loy SF. An epidemiological analysis of overuse injuries among recreational cyclists. Int J Sports Med. 1995;16:201–6. doi: 10.1055/s-2007-972992. [DOI] [PubMed] [Google Scholar]
- 4.Zwingenberger S, Valladares RD, Walther A, Beck H, Stiehler M, Kirschner S, et al. An epidemiological investigation of training and injury patterns in triathletes. J Sports Sci. 2014;32:583–90. doi: 10.1080/02640414.2013.843018. [DOI] [PubMed] [Google Scholar]
- 5.Silberman MR. Bicycling injuries. Curr Sports Med Rep. 2013;12:337–45. doi: 10.1249/JSR.0b013e3182a4bab7. [DOI] [PubMed] [Google Scholar]
- 6.Clarsen B, Krosshaug T, Bahr R. Overuse injuries in professional road cyclists. Am J Sports Med. 2010;38:2494–501. doi: 10.1177/0363546510376816. [DOI] [PubMed] [Google Scholar]
- 7.Vleck VE, Garbutt G. Injury and training characteristics of male elite, development squad, and club triathletes. Int J Sports Med. 1998;19:38–42. doi: 10.1055/s-2007-971877. [DOI] [PubMed] [Google Scholar]
- 8.Cowan DN, Bedno SA, Urban N, Yi B, Niebuhr DW. Musculoskeletal injuries among overweight army trainees: Incidence and health care utilization. Occup Med (Lond) 2011;61:247–52. doi: 10.1093/occmed/kqr028. [DOI] [PubMed] [Google Scholar]
- 9.Wanich T, Hodgkins C, Columbier JA, Muraski E, Kennedy JG. Cycling injuries of the lower extremity. J Am Acad Orthop Surg. 2007;15:748–56. doi: 10.5435/00124635-200712000-00008. [DOI] [PubMed] [Google Scholar]
- 10.Deakon RT. Chronic musculoskeletal conditions associated with the cycling segment of the triathlon; prevention and treatment with an emphasis on proper bicycle fitting. Sports Med Arthrosc. 2012;20:200–5. doi: 10.1097/JSA.0b013e3182688fa0. [DOI] [PubMed] [Google Scholar]
- 11.Bini R, Hume PA, Croft JL. Effects of bicycle saddle height on knee injury risk and cycling performance. Sports Med. 2011;41:463–76. doi: 10.2165/11588740-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 12.Coppack RJ, Etherington J, Wills AK. The effects of exercise for the prevention of overuse anterior knee pain: A randomized controlled trial. Am J Sports Med. 2011;39:940–8. doi: 10.1177/0363546510393269. [DOI] [PubMed] [Google Scholar]
- 13.Lauersen JB, Bertelsen DM, Andersen LB. The effectiveness of exercise interventions to prevent sports injuries: A systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2014;48:871–7. doi: 10.1136/bjsports-2013-092538. [DOI] [PubMed] [Google Scholar]
- 14.Koeppel D. Flight of the Pigeon, Bicycling. Vol. 48. Emmaus, Pennsylvania, USA: Rodale, Inc; 2007. pp. 60–6. [Google Scholar]
- 15.Eric A. Sampson, Denver, Colo. Integrated Bicycle Pedal with Self Centering and Lateral Release Capabilities Sampson Sports, Inc. 1989 [Google Scholar]
- 16.Garrett WE, Donald T. Exercise and Sport Science. Philadelphia, USA: Lippincott Williams and Wilkins; 2000. [Google Scholar]
- 17.Fordham S, Garbutt G, Lopes P. Epidemiology of injuries in adventure racing athletes. Br J Sports Med. 2004;38:300–3. doi: 10.1136/bjsm.2002.003350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Manninen JS, Kallinen M. Low back pain and other overuse injuries in a group of Japanese triathletes. Br J Sports Med. 1996;30:134–9. doi: 10.1136/bjsm.30.2.134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Al-Arfaj AS, Alballa SR, Al-Saleh SS, Al-Dalaan AM, Bahabry SA, Mousa MA, et al. Knee osteoarthritis in Al-Qaseem, Saudi Arabia. Saudi Med J. 2003;24:291–3. [PubMed] [Google Scholar]
- 20.Nguyen US, Zhang Y, Zhu Y, Niu J, Zhang B, Felson DT. Increasing prevalence of knee pain and symptomatic knee osteoarthritis: Survey and cohort data. Ann Intern Med. 2011;155:725–32. doi: 10.1059/0003-4819-155-11-201112060-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Claes T, Claes S, De Roeck J, Claes T. Prepatellar Friction Syndrome: A common cause of knee pain in the elite cyclist. Acta Orthop Belg. 2015;81:614–9. [PubMed] [Google Scholar]
- 22.Hiemstra LA, Kerslake S, Irving C. Anterior knee pain in the athlete. Clin Sports Med. 2014;33:437–59. doi: 10.1016/j.csm.2014.03.010. [DOI] [PubMed] [Google Scholar]
- 23.Rothermich MA, Glaviano NR, Li J, Hart JM. Patellofemoral pain: Epidemiology, pathophysiology, and treatment options. Clin Sports Med. 2015;34:313–27. doi: 10.1016/j.csm.2014.12.011. [DOI] [PubMed] [Google Scholar]
- 24.Taanila H, Hemminki AJ, Suni JH, Pihlajamäki H, Parkkari J. Low physical fitness is a strong predictor of health problems among young men: A follow-up study of 1411 male conscripts. BMC Public Health. 2011;11:590. doi: 10.1186/1471-2458-11-590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Taanila H, Suni J, Pihlajamäki H, Mattila VM, Ohrankämmen O, Vuorinen P, et al. Aetiology and risk factors of musculoskeletal disorders in physically active conscripts: A follow-up study in the Finnish Defence Forces. BMC Musculoskelet Disord. 2010;11:146. doi: 10.1186/1471-2474-11-146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Taanila H, Suni JH, Kannus P, Pihlajamäki H, Ruohola JP, Viskari J, et al. Risk factors of acute and overuse musculoskeletal injuries among young conscripts: A population-based cohort study. BMC Musculoskelet Disord. 2015;16:104. doi: 10.1186/s12891-015-0557-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Herman K, Barton C, Malliaras P, Morrissey D. The effectiveness of neuromuscular warm-up strategies, that require no additional equipment, for preventing lower limb injuries during sports participation: A systematic review. BMC Med. 2012;10:75. doi: 10.1186/1741-7015-10-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Moradi-Lakeh M, El Bcheraoui C, Tuffaha M, Daoud F, Al Saeedi M, Basulaiman M, et al. Tobacco consumption in the Kingdom of Saudi Arabia, 2013: Findings from a national survey. BMC Public Health. 2015;15:611. doi: 10.1186/s12889-015-1902-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Eriksen WB, Brage S, Bruusgaard D. Does smoking aggravate musculoskeletal pain? Scand J Rheumatol. 1997;26:49–54. doi: 10.3109/03009749709065664. [DOI] [PubMed] [Google Scholar]
- 30.Teyhen DS, Shaffer SW, Butler RJ, Goffar SL, Kiesel KB, Rhon DI, et al. What risk factors are associated with musculoskeletal injury in US army rangers? A prospective prognostic study. Clin Orthop Relat Res. 2015;473:2948–58. doi: 10.1007/s11999-015-4342-6. [DOI] [PMC free article] [PubMed] [Google Scholar]