

Abstract
Background
Having a regular primary care provider (i.e., family physician or nurse practitioner) is widely considered to be a prerequisite for obtaining healthcare that is timely, accessible, continuous, comprehensive, and well-coordinated with other parts of the healthcare system. Yet, 4.6 million Canadians, approximately 15% of Canada’s population, are unattached; that is, they do not have a regular primary care provider. To address the critical need for attachment, especially for more vulnerable patients, six Canadian provinces have implemented centralized waiting lists for unattached patients. These waiting lists centralize unattached patients’ requests for a primary care provider in a given territory and match patients with providers. From the little information we have on each province’s centralized waiting list, we know the way they work varies significantly from province to province. The main objective of this study is to compare the different models of centralized waiting lists for unattached patients implemented in six provinces of Canada to each other and to available scientific knowledge to make recommendations on ways to improve their design in an effort to increase attachment of patients to a primary care provider.
Methods
A logic analysis approach developed in three steps will be used. Step 1: build logic models that describe each province’s centralized waiting list through interviews with key stakeholders in each province; step 2: develop a conceptual framework, separate from the provincially informed logic models, that identifies key characteristics of centralized waiting lists for unattached patients and factors influencing their implementation through a literature review and interviews with experts; step 3: compare the logic models to the conceptual framework to make recommendations to improve centralized waiting lists in different provinces during a pan Canadian face-to-face exchange with decision-makers, clinicians and researchers.
Discussion
This study is based on an inter-provincial learning exchange approach where we propose to compare centralized waiting lists and analyze variations in strategies used to increase attachment to a regular primary care provider. Fostering inter-provincial healthcare systems connectivity to improve centralized waiting lists’ practices across Canada can lever attachment to a regular provider for timely access to continuous, comprehensive and coordinated healthcare for all Canadians and particular for those who are vulnerable.
Electronic supplementary material
The online version of this article (doi:10.1186/s12913-017-2007-8) contains supplementary material, which is available to authorized users.
Keywords: Primary health care, Health services accessibility, Comparative study, Waiting lists, Physicians, General practitioners, Physician patient relationship, Unattached patients
Background
Attachment, a formal or informal affiliation to a regular provider such as a nurse practitioner or family physician [1], is widely considered to be a prerequisite for primary healthcare that is accessible, continuous, comprehensive, and well-coordinated with other levels (e.g., secondary, tertiary) or types (e.g., social, community-based) of care [2–14]. There is strong evidence in the scientific literature that suggests that patients who are attached to a primary care provider benefit from better care coordination [15–17], chronic disease management [18, 19] and receive more preventative care [20, 21], use emergency services less frequently [22–24] and have better health outcomes [25, 26].
Compared to other OECD countries, Canada ranks low in terms of access to a primary care provider [27]. Thus, attachment to a primary care provider is an especially important issue in Canada because this is most often the first point of contact to the rest of the healthcare system. For example, patients need a referral from a family physician or need to go through the emergency department to access specialized care. Canadian primary care providers’ role goes beyond providing primary healthcare and preventive care [28] as the structure of healthcare systems positions them as the “gatekeepers” to secondary and tertiary care [29–31]. Access to healthcare for unattached patient is therefore limited in Canada [32].
Several Canadian commissions on healthcare have recommended that primary healthcare be reinforced to guarantee access to a primary care provider to every Canadian [33–38]. Yet, 4.6 million Canadians, approximately 15% of Canada’s population, do not have a regular primary care provider [39]. Moreover, in Canada, vulnerable patients, those with multiple intersecting determinants of health including complex physical and mental health and healthcare needs, being young or a recent immigrant, having a low income level, living in a rural or remote area, and those with low social support are less likely to be attached to a primary care provider [40, 41] despite being the ones who would benefit most from access to comprehensive and continuous primary care [42, 43].
Centralized waiting lists for unattached patients
To address the critical need for attachment, six provinces have implemented centralized waiting lists to coordinate the supply of primary care providers and demand of patients for attachment (see Table 1). These waiting lists generally aim to centralize unattached patients’ requests for a primary care provider in a given jurisdiction and to match unattached patients with providers, based on availability of primary care workforce and, in some cases, medical need [32, 44].
Table 1.
Centralized waiting lists for unattached patients implemented across Canada
| Province | Program Name | Implementation Year |
|---|---|---|
| Prince Edward Island | Patient Registry Program | 1998 |
| Quebec | Guichets d’accès à un médecin de famille | 2008 |
| Ontario | Health Care Connect | 2009 |
| Manitoba | Family Doctor Finder | 2013 |
| New-Brunswick | Patient Connect NB | 2013 |
| British Columbia | A GP for Me | 2015 |
In Canada, the provinces and territories administer and deliver most health care services [45]. The roles of the provinces/territories include administration of their health insurance plans; planning and funding of services in hospitals and other health facilities as well as of services provided by doctors and other health professionals and planning and implementing health promotion and public health initiatives. Therefore, initiatives such as centralized waiting lists for unattached patients may be quite different in each province or territory. Moreover, there is limited knowledge exchange between provinces regarding such initiatives.
Wide variations in centralized waiting lists for unattached patients across Canada
From the little information available, we know there are wide variations between provinces in the way centralized waiting lists for unattached patients work [46]. Each province’s waiting list has distinct characteristics. This study will lead to a better understanding of the components of each of the six centralized waiting lists. A few examples of variations are described below.
Guidelines for the centralized waiting lists
Patient eligibility for registering in a centralized waiting list differs from one province to another. In Ontario, patients who already have a primary care provider are not eligible to register in the centralized waiting list, while in New Brunswick, patients who have a provider, but wish to change providers are allowed to register on the list [47, 48]. The level of governance of centralized waiting lists is also variable. In Ontario, the program is managed at a provincial level with a delegation of management to the Community Care Access Centers at a regional level; while in Quebec, the program is managed at a local level by the Integrated Centers for Health and Social Services with some provincial oversight.
Incentives to providers to attach new patients
Incentives to providers to attach new patient differ from one province to another. In Quebec, primary care providers receive a one-time financial incentive to attach a new patient. These incentives are more substantial if the patient is attached via a centralized waiting list. For these patients, the presence of specific types of vulnerabilities determines the amount physicians will receive: CAD $23 to attach a “non-vulnerable patient” (i.e., healthy patient), CAD$150 to attach a “vulnerable patient” (i.e., with at least one chronic disease or over 70 years old), and CAD$300 to attach a “super vulnerable patient” (i.e., suffering from mental illness or substance abuse) [49]. In Ontario, family physicians receive a one-time payment of CAD$350 for attaching a new “complex-vulnerable patient” from the centralized waiting list [50].
Structure to receive & follow-up requests for a provider from patients
The structure for receiving requests for primary care providers varies quite a bit between provinces. In New Brunswick, for example, unattached patients contact Tele-care 8-1-1, a pre-existing health advice and information line, to register on the centralized waiting list [51]. In Quebec, requests for a family physician can be made through a website hosted by the provincial health insurance. Additionally, each local health network has a nurse and administrative assistant who are available to assist patients fill out a request [44, 52]. In Ontario and Manitoba, this part of the process is outsourced to a third party.
Identifying & prioritising vulnerable patients
Moreover, there seems to be significant differences in how vulnerable patients are defined and how they are prioritized when being attached to a primary care provider. In Quebec, patients are prioritized into five priority categories (A to E) at a local level based on the urgency of their need for a primary care provider [52, 53]. The urgency of need is assessed based on the self-reported presence of specific types of vulnerabilities (e.g., diabetes, mental illness, cancer, HIV/AIDs) or being over 70 years old. Patients may also request a health assessment by a nurse, which is done over the phone. There are provincially recommended wait times for each priority category: ≤7 days for A, ≤14 days for B, ≤21 days for C, ≤1 month for D and ≤3 months for E. In Ontario, “complex-vulnerable patients” are defined as having one or more co-morbidities, or being frail based on self-assessed health status, chronic conditions or health problems, activity limiting disability, mental health status and body mass index [54]. Priority is then given to those with the greatest need for a primary care provider. In New Brunswick, patients are asked to answer a health screening questionnaire regarding long term health conditions and need for follow-up (multiple medications, history of mental illness, children under 5, etc.), but patients are assigned to a primary care provider on a first-come, first serve basis [48].
Matching patients to providers
The way patients are matched with providers is different in each province. In Manitoba, patients are asked about their provider preferences (type of provider, language spoken by provider, provider gender, and distance they are willing to travel) [55]. Conversely, in Quebec, no questions are asked about patients’ preferences, the only consideration is geographic distance to the clinic [52, 56]. In addition, provinces such as Ontario and Manitoba offer attachment to a nurse practitioner or family physician, while Quebec, for instance, only offers attachment to family physicians. Provinces also have varying processes in place to match providers and patients. In Ontario, nurses called Care Connectors are locally mandated to help patients find a primary care provider and are the patients’ main contact during their time on the waiting list [57]. In Quebec, physicians called Local Medical Coordinators are mandated to help the centralized waiting list attach patients, but are not assigned to patients like in Ontario.
Impacts of centralized waiting lists
Currently, we have access to very little information that allows us to compare the impacts of centralized waiting lists across provinces. However, we know that the volume of patients attached to primary care providers varies significantly. For instance, in Manitoba, around 30 000 patients have been attached through Family Doctor Finder since its implementation in 2013 [58]. In comparison, the guichets d’accès aux médecins de famille in Quebec has attached over 800 000 patients since its implementation in 2008 [53]. We also know that, over the last year, the effectiveness of the centralized waiting list in attaching complex patients has been heterogeneous. Ontario has successfully attached 85% of what they identified as being “complex-vulnerable patients” [59]; while Quebec has attached only 20% of the patients identified as being “vulnerable”.
British Columbia: a special case
Most centralized waiting lists in the other five provinces were mandated at a provincial level and implemented more or less uniformly across the province with slight variations in local practices. However, for the “A GP for Me” initiative in British Columbia, each division analyzed their needs and implemented various strategies to improve attachment according to those needs. Therefore, only a handful of divisions implemented some type of centralized waiting list for unattached patients. The case of British Columbia, although different from the other provinces, is especially interesting because of the variety of innovative strategies combined with centralized waiting lists to improve attachment. Therefore, we will identify common characteristics at a provincial level, but will also conduct an in-depth analysis of some divisions.
Study objective
The main objective of this study is to compare the different models of centralized waiting lists for unattached patients implemented in six provinces of Canada to each other and to available scientific knowledge to make recommendations on ways to improve their design in an effort to increase attachment of patients to a primary care provider.
Methods
Overall study design
We will conduct a logic analysis to compare, analyze and identify improvement strategies for the centralized waiting lists for unattached patients across Canada. All six provinces that have implemented a centralized waiting list for unattached and complex patients will be included in this study.
Logic analysis is a theory-based evaluation that tests the adequacy between the intended outcomes of an intervention and the actions undertaken to achieve those outcomes [60, 61]. It assesses the validity of the intervention’s theory by identifying the main characteristics of the program and the key contextual factors that may affect the intervention’s effectiveness to produce intended outcomes [61, 62].
There are several benefits of using a logic analysis to evaluate an intervention. First, because it examines the fit between actual activities and strategies of the intervention, and those that should be implemented to achieve the intended outcomes, the use of a logic analysis may reveal gaps in logic [63]. Second, testing the program’s theory can provide important insights into the intervention’s strengths and weaknesses while mobilizing various stakeholders in a valuable reflection process [60]. It can therefore provide stakeholders with a rapid feedback on the validity of their intervention and on the ways they can improve the effectiveness of their intervention. Finally, it allows for the identification of adequate performance indicators based on data that is relevant to the intervention’s components.
A logic analysis is conducted in three steps: 1) building logic models of the interventions, 2) developing a conceptual framework based on scientific knowledge (literature and expert views), and 3) comparing the logic models to the conceptual framework [60].
Step 1: Build logic models that describes each province’s centralized waiting list
The logic models will be elaborated based on Mitchell & Lewis’s Manual to Guide the Development of Local Evaluation Plans [63]. This particular model offers a simple diagram of the main components of a unique intervention and is widely used in research on primary healthcare interventions in Canada. For instance, Mitchell & Lewis’ model is currently being used by the 12 research programs in the Canadian Institutes of Health Research's signature initiative on community based primary healthcare [64]. It is therefore relevant to use this model to evaluate complex, multilevel and multifaceted interventions such as centralized waiting lists for unattached patients.
This model assumes that inputs/strategies of the intervention will influence the processes and structures, which will then influence the impacts, which will in turn lead to the intended outcomes of the intervention. It aims to identify every component involved in the desired change, indicators to measure these components, as well as gaps in the intervention’s logic. Six categories of components must be included in the model.
Action areas: the focus area of the intervention;
Outcomes: intended changes in health and wellbeing of targeted population;
Inputs/strategies: resources, strategies and activities needed to launch the intervention;
Processes and structures: mechanisms and characteristics of services, systems or activities that have to be maintained over time to achieve impacts;
Impacts: changes that are crucial to achieving intended outcomes;
Contextual factors: political, cultural, socioeconomic and geographic factors that might affect the intervention’s effectiveness in producing intended outcomes.
We have provided below an example of how the logic model will be used to map out the different components of centralized waiting lists for unattached patients (see Fig. 1).
Fig. 1.
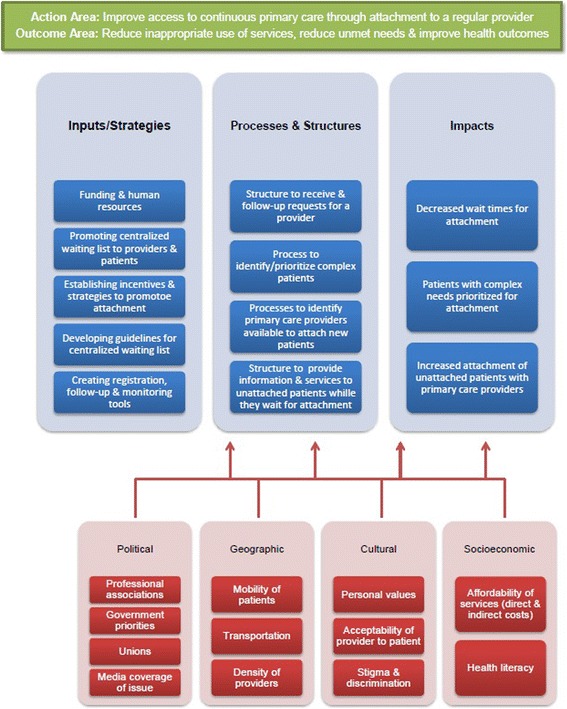
Logic model template
In each of the six cases, a variety of data sources will be used. First, we will review the grey literature to identify the main characteristics of each centralized waiting list. The grey literature will be reviewed using search engines such as Google and Google Scholar as well as specific sources such as websites from health institutions, national and provincial government, provincial and local newspapers [65]. We will also use the grey literature to identify key stakeholders in each province (professional associations, decision-makers, clinicians, etc.). In addition, our knowledge users will help us identify key stakeholders of the centralized waiting list in their province. We will then conduct semi-structured interviews with the key stakeholders identified and use a snowballing method to identify additional participants. The aim of these interviews is to gain an in depth understanding of the characteristics each centralized waiting list (for more details, please consult interview guide in Additional file 1). Interviews will be conducted in person, by phone or by videoconference depending on the location of the interviewee. We plan to conduct interviews in each province until we reach saturation (around eight interviews per case). All interviews will be taped and transcribed when formally authorized by respondents.
All documents and interview transcriptions will be coded using NVivo (QSR) software. A list of initial codes based on the logic model template (Fig. 1) has been established. This list details the five elements of logical analysis on centralized waiting list which are 1) the needed inputs for implementation of centralized waiting list, 2) process for requesting a family physician, 3) prioritization of patients and attachment to a primary care provider, 4) perceived outputs of the centralized waiting list and 5) elements from the contexts that might have an influence on the implementation of the centralized waiting list. This list will be modified and enhanced over the course of the analyses.
Two independent team members will code the data to ensure reproducibility and reliability. A double-coding technique will be used in order to control the coding step and to guaranty the repeatability and reliability of the method. Coding results will be compared. The codes will be refined where differences appear and then coding will be repeated. This process will be repeated until the two analysts obtain inter-coder agreement of more than 90% [66]. Codes will be grouped in the corresponding themes and also in new themes that have appeared during analysis. We will analyze transcripts for each province separately in order to better understand the how each centralized waiting list works. Coded materials will be analyzed using a thematic analysis and results will be synthetized using tables and matrices [66, 67]. Data obtained for each province will be summarized.
The characteristics of each province’s centralized waiting list will be presented in a logic model. We will then use these logic models to perform a cross-case (inter-provincial) analysis of the six centralized waiting lists. We will compare the centralized waiting lists, highlight similarities and differences between them and identify factors that can lead to an increase in attachment of patients to a primary care provider. The logic models will be presented in a graphic form. We will collaborate closely with a graphic designer to ensure the models are easy to understand. The information in each logic model will be validated by key stakeholders from the centralized waiting list in each province. A face-to-face meeting will be organized on each site between the key informants and members from our team.
Step 2: Develop a conceptual framework based on key characteristics of centralized waiting lists for unattached patients and factors influencing their implementation
Developing a conceptual framework is a core component of the logic analysis and critical to assessing an intervention’s rationale. This step consists of identifying “the best ways of doing things” [60]. This is done by analysing the centralized waiting lists’ components and identifying the optimal way to achieve the intended outcomes or by identifying alternative ways, if any, of achieving these outcomes.
In order to develop a conceptual framework, a realist review approach will be used. Based on evidence from the scientific literature and experts’ views related to the intervention [61, 68, 69], the realist review is a theory-driven approach developed in order to explore causal processes that generate outcomes within programs or interventions. This approach aims to evaluate the context, mechanism and outcomes of interventions with a heterogeneous body of evidence. Given that this study is being conducted over a 12 month period and that there is very limited literature on centralized waiting lists for unattached patients, this approach was chosen in order to assemble a body of evidence on the mechanisms of different aspects of centralized waiting lists for unattached patients.
We will use the realist review approach for three key components of centralized waiting lists for unattached patients:
What are unattached patients’ characteristics and primary care needs?
What are the best ways to manage centralized waiting lists?
What are the most effective incentives (financial or other) to increase the number of new patients attached to primary care providers?
The realist review will comprise three distinct review processes, covering the three aforementioned aspects. The primary literature searches will be performed by a member of the research team with the EBSCOhost interface through four databases: Medline, CINAHL, PsychInfo and SocIndex. The research will be limited to peer-reviewed texts in French and English published between 2000 and 2016. A Boolean search will be performed using search terms specific to each subject developed by the research team with the help of an information specialist.
A classic two-step review selection process will be conducted by two reviewers to identify the relevant articles to be included in the review. The first step of the selection process will be a review based on articles' title and abstract. Articles from the primary literature research will be reviewed by the two reviewers on the basis of potential relevance regarding the process of each research questions. Following the title and abstract screening, articles will be screened for full text review by the two reviewers based on agreement of reviewing and discussion on disagreement. Criteria for the full text review will be elaborated by main researcher and the reviewers in order to proceed to the selection of the relevant texts to be included on the studies.
To ensure the maximal selection of relevant articles, each of the selected will get their references screened and a research through Google Scholar will be done to find articles citing the article as well as similar articles. An expert in each of components studied in this review will also be contacted in order to validate the content of the selected data and ensure that important articles were not forgotten in the process.
Data will be extracted following an extraction grid developed by a member of the research team for each of the three research aspects. A second member of the research team will review the extraction to ensure all relevant information has been extracted. The research team will construct the extraction grids in order to extract all relevant information that can be linked to the research questions. The analysis of the data collected with the extraction grids will be done following a thematic analysis method.
To ensure balance between relevance and scientific rigour, papers will be assessed based on both relevance and quality. The quality appraisal will be based on the prompts outlined by Dixon & Woods [70] and will be used to determine the contribution of the data to the reviews.
Step 3: Compare the logic models to the conceptual framework to make recommendations to improve centralized waiting lists in different provinces
We will compare the logic models built in step 1 to the conceptual framework developed by consulting experts and reviewing the literature in step 2. This should produce new readings of the centralized waiting lists for unattached patients that highlight strengths and weaknesses, as well as the strength of the causal chain toward the impacts and intended outcomes [60]. Our aim is to identify the strengths and weaknesses of each centralized waiting list under study, the characteristics that seem promising to promote attachment, particularly for vulnerable patients and the contextual factors that may affect the intervention’s effectiveness in order to propose strategies to improve attachment to a primary care provider that are relevant to each province’s context.
This step will be done using a participatory approach during a one-day face-to-face meeting with the research team and key stakeholders involved in centralized waiting lists for unattached patients across the six provinces. A participative approach will create consensus on what is required to improve current practices and adapt promising strategies to different contexts, enhance the appropriation of results, and initiate the necessary changes [71].
Results’ dissemination
Promising strategies will be described in short videotaped interviews with the decision-makers of each province. The footage from these interviews will be used to put together short video clips. The video editing will be done in the multimedia laboratory at the Centre de recherche Hôpital Charles-Le Moyne. Also, the promising strategies will be summarized in a brief report. A dissemination strategy of the video clips, logic model illustrations and brief report produced will be developed in complementarity to the production of peer-reviewed scientific articles and presentations in international conferences.
Discussion
No study has compared these complex organizational models across Canada and analyzed variations in strategies used to increase attachment to a regular primary care provider, for the general population and for vulnerable populations. To our knowledge, only one study has examined the implementation and outcomes of centralized waiting lists for unattached patients and this study focuses on the province of Quebec [7] and further comparative studies are needed. The natural experimentation of centralized waiting lists for unattached patients implemented in six provinces represents a unique opportunity to better understand these different models, to learn from the different experiences and to identify promising strategies to improve the effectiveness of these centralized waiting lists. The results from this study will be useful for decision-makers of healthcare systems in Canada and countries with similar healthcare systems by providing strategies and key elements for implementing effective centralized waiting lists.
Implications for implementation
This study is based on an inter-provincial learning exchange approach where we propose to compare centralized waiting lists and analyze variations in strategies used to increase attachment to a regular primary care provider. To date, there has been very little collaboration between the decision-makers of each province’s centralized waiting lists to discuss best practices or promising strategies. Our research team has developed collaborations with key stakeholders in each province of the six provinces that have implemented a centralized waiting list for unattached patients. Comparing the six provinces’ models to the conceptual framework will allow us to understand the differences between the centralized waiting lists in the six provinces, to explain these differences according to context, and identify strategies to improve certain components and mechanisms for the six centralized waiting lists to better achieve intended outcomes. Our inter-provincial learning exchange approach will allow stakeholders from different provinces to come together to discuss the results of our study which in turn will enhance their appropriation of results, and initiate conversations about changes that could be made in each province. In addition to our integrated approach with key stakeholders, six Strategy for Patient-Oriented Research (SPOR) on Primary and Integrated Health Care Innovation Networks have agreed to provide support in connecting with additional stakeholders and disseminating results of the study within their province.
Fostering inter-provincial healthcare systems' connectivity to improve centralized waiting lists’ practices across Canada can therefore lever attachment to a regular provider for timely access to continuous, comprehensive and coordinated healthcare for all Canadians and particular for those who are vulnerable.
Acknowledgements
Key stakeholders from each province under study have accepted to collaborate actively in this project as knowledge users and collaborators. We wish to thank them for their collaboration in this study. We wish to thank all organizations that have provided financial and inkind support.
Funding
This study is funded by the Canadian Institutes of Health Research (#145183), Charles-LeMoyne Hospital Research Center, Quebec SPOR Network in Primary and Integrated and Chair in Applied Health Economics/Health Policy held by Dr. Michael Green.
Availability of data and materials
Not applicable.
Authors’ contributions
MB led the coordination and the conceptualization of the study. MB and MAS wrote the first draft and all authors critically reviewed it and provided comments to improve the manuscript. MG, SK, JSutherland, JJ, STW, JShaw, VAC, DC and AB read and commented on the final manuscript. All authors read and approved the final manuscript.
Competing interests
Sabrina T. Wong is an Associate Editor of BMC Health Services Research. The others authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Ethical approval was obtained from the research ethics board of the Centre Hospitalier Universitaire de Sherbrooke (ref. number 2017–1433), from Queen’s University Community Support Service Organizations and Community Mental Health and Addiction Agencies (ref. number 6018938), from the Office of Research Services Behavioral Research Ethics Board of University of British Columbia, (ref. number H16-01697), from the comité d’éthique de la recherche avec les êtres humains de l’Université de Moncton (ref. number 1516–081), from University of Manitoba (ref. number HS 19960 (H2016:271)) and from PEI Ethics Board from Health PEI (date of ethical approval July 21st, 2016). Those six ethical approvals cover all the settings where the research will be conducted, as we have obtained one of every province involved in the study.
Information about participation’s terms and conditions will be explain and read to all participants. Then, they will be asked to complete and sign a written consent form.
Additional files
Semi-structured interview guide. Interview guide. (PDF 183 kb)
Contributor Information
Mylaine Breton, Email: mylaine.breton@usherbrooke.ca.
Michael Green, Email: michael.green@dfm.queensu.ca.
Sara Kreindler, Email: sara.kreindler@umanitoba.ca.
Jason Sutherland, Email: jason.sutherland@ubc.ca.
Jalila Jbilou, Email: jalila.jbilou@umoncton.ca.
Sabrina T. Wong, Email: Sabrina.Wong@nursing.ubc.ca
Jay Shaw, Email: jay.shaw@wchospital.ca.
Valorie A. Crooks, Email: crooks@sfu.ca
Damien Contandriopoulos, Email: damien.contandriopoulos@umontreal.ca.
Mélanie Ann Smithman, Email: Melanie.ann.smithman@usherbrooke.ca.
Astrid Brousselle, Email: astrid.brouselle@usherbrooke.ca.
References
- 1.Karazivan P. La médecine familiale vue par les jeunes omnipraticiens: rejet de la vocation et de la continuité des soins. Montréal: Université de Montréal; 2010. [Google Scholar]
- 2.Jatrana S, Crampton P. Affiliation with a primary care provider in New Zealand: Who is, who isn’t. Health Policy. 2009;91(3):286–96. doi: 10.1016/j.healthpol.2008.12.015. [DOI] [PubMed] [Google Scholar]
- 3.Jatrana S, Crampton P, Richardson K. Continuity of care with general practionners in New Zealand: results from So-FIE-Primary care. J N Z Med Assoc. 2011;124(1329):286–96. [PubMed] [Google Scholar]
- 4.Haggerty J, Lévesque JF, Santor D, Burge F, Beaulieu C, Baouharaoui F. Accessibility from the patient perspective: comparison of primary healthcare evaluation instruments. Healthc Policy. 2011;7:94–107. [PMC free article] [PubMed] [Google Scholar]
- 5.Lévesque J-F, Haggerty JL, Burge F, Beaulieu M-D, Gass D, Pineault R, et al. Canadian experts’ views on the importance of attributes within professional and community-oriented primary healthcare models. Healthc Policy. 2011;7(Special Issue):21–30. [PMC free article] [PubMed] [Google Scholar]
- 6.Levesque J-F, Harris MF, Russell G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. 2013;12(1):18–26. doi: 10.1186/1475-9276-12-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Breton M, Brousselle A, Boivin A, Loignon C, Touati N, Dubois C-A, et al. Evaluation of the implementation of centralized waiting lists for patients without a family physician and their effects across the province of Quebec. Implement Sci. 2014;9(1):117. doi: 10.1186/s13012-014-0117-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Frenk JA. The concept and measure of accessibilty. In: White KL, Frenk JA, Ordonez C, Paganini JM, Starfield B, editors. Health services research: an anthology. Washington DC: Pan American Health Organization; 1992. p. 842-55.
- 9.Nutting P, Goodwin M, Flocke S, Zyzanski S, Stange K. Continuity of primary care: to whom does it matter and when? Ann Fam Med. 2003;1(3):149–55. doi: 10.1370/afm.63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Burge F, Haggerty J, Pineault R, Beaulieu MD, Lévesque JF, Beaulieu C, et al. Relational continuity from the patient perspective: comparison of primary healthcare evaluation instruments. Healthc Policy. 2011;7:124–38. [PMC free article] [PubMed] [Google Scholar]
- 11.Chan BTB. The declining comprehensiveness of primary care. Can Med Assoc J. 2002;166(4):429–34. [PMC free article] [PubMed] [Google Scholar]
- 12.Bazemore A, Petterson S, Peterson L, Philips RL., Jr More comprehensive care among family physicians is associated with lower costs and fewer hospitalizations. Ann Fam Med. 2015;13:206–13. doi: 10.1370/afm.1787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Brown AD, Goldacre MJ, Hicks N, Rourke JT, et al. Hospitalization for ambulatory care-sensitive conditions: a method for comparative access and quality studies using routinely collected statistics. Can J Public Health. 2001;92(2):155–9. doi: 10.1007/BF03404951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Weingarten S, Henning J, Badamgarav E, Knight K, Hasselblad V, Gano A, et al. Interventions used in disease management programmes for patients with chronic illness which ones work? Meta-analysis of published reports. BMJ. 2002;325(7370):925. doi: 10.1136/bmj.325.7370.925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Stille CJ, Jerant A, Bell D, Meltzer D, Elmore JG. Coordinating care across diseases, settings, and clinicians: a key role for the generalist in practice. Ann Intern Med. 2005;142(8):700–8. doi: 10.7326/0003-4819-142-8-200504190-00038. [DOI] [PubMed] [Google Scholar]
- 16.Bayliss EA, Edwards AE, Steiner JF, Main DS. Processes of care desired by elderly patients with multimorbidities. Fam Pract. 2008;25(4):287–93. doi: 10.1093/fampra/cmn040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fung CS, Wong CK, Fong DY, Lee A, Lam CL. Having a family doctor was associated with lower utilization of hospital-based health services. BMC Health Serv Res. 2015;15(1):1–9. doi: 10.1186/s12913-015-0705-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rothman AA, Wagner EH. Chronic illness management: what is the role of primary care? Ann Intern Med. 2003;138(3):256–61. doi: 10.7326/0003-4819-138-3-200302040-00034. [DOI] [PubMed] [Google Scholar]
- 19.Østbye T, Yarnall KSH, Krause KM, Pollak KI, Gradison M, Michener JL. Is there time for management of patients with chronic diseases in primary care? Ann Fam Med. 2005;3(3):209–14. doi: 10.1370/afm.310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Starfield B, Shi L, Machinki J. Contribution of primary care to health systems and health. Milbank Q. 2005;83:457–502. doi: 10.1111/j.1468-0009.2005.00409.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Grunfeld E, Levine MN, Julian JA, Coyle D, Szechtman B, Mirsky D, et al. Randomized trial of long-term follow-up for early-stage breast cancer: a comparison of family physician versus specialist care. J Clin Oncol. 2006;24(6):848–55. doi: 10.1200/JCO.2005.03.2235. [DOI] [PubMed] [Google Scholar]
- 22.Christakis DA, Wright JA, Koepsell TD, Emerson S, Connell FA. Is greater continuity of care associated with less emergency department utilization? Pediatrics. 1999;103(4 Pt 1):738–42. doi: 10.1542/peds.103.4.738. [DOI] [PubMed] [Google Scholar]
- 23.Christakis DA, Mell L, Koepsell TD, Zimmerman FJ, Connell FA. Association of lower continuity of care with greater risk of emergency department use and hospitalization in children. Pediatrics. 2001;107(3):524–9. doi: 10.1542/peds.107.3.524. [DOI] [PubMed] [Google Scholar]
- 24.Burge F, Lawson B, Johnston G. Family physician continuity of care and emergency department use in end-of-life cancer care. Med Care. 2003;41(8):992–1001. doi: 10.1097/00005650-200308000-00012. [DOI] [PubMed] [Google Scholar]
- 25.Oates J, Weston WW, Jordan J. The impact of patient-centered care on outcomes. Fam Pract. 2000;49:796–804. [PubMed] [Google Scholar]
- 26.Griffin SJ, Kinmonth A-L, Veltman MWM, Gillard S, Grant J, Stewart M. Effect on health-related outcomes of interventions to alter the interaction between patients and practitioners: a systematic review of trials. Ann Fam Med. 2004;2(6):595–608. doi: 10.1370/afm.142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Commonwealth Fund International Health Policy Survey. Schoen C, et al. Toward higher-performance health systems: adults’ health care experiences in seven countries, 2007. Health Aff. 2007;26(6):w717–w34. doi: 10.1377/hlthaff.26.6.w717. [DOI] [PubMed] [Google Scholar]
- 28.College of Family Physicians of Canada. Four principles of family medicine. Available from: http://www.cfpc.ca/principles/. Accessed 17 Jan 2017.
- 29.Watt D. The Family Physician: gatekeeper to the health-care system. Can Fam Physician. 1987;33:1101–4. [PMC free article] [PubMed] [Google Scholar]
- 30.Pena-Dolhun E, Grumbach K, Vranizan K, Osmond D, Bindman AB. Unlocking specialists’ attitudes toward primary care gatekeepers. J Fam Pract. 2001;50(Suppl 12):1032–7. [PubMed] [Google Scholar]
- 31.Health Council of Canada . Decisions, decisions: family doctors as gatekeepers to prescription drugs and diagnostic imaging in Canada. Toronto: Health Council; 2010. [Google Scholar]
- 32.Crooks VA, Agarwal G, Harrison A. Chronically ill Canadians’ experiences of being unattached to a family doctor: a qualitative study of marginalized patients in British Columbia. BMC Fam Pract. 2012;13:69. doi: 10.1186/1471-2296-13-69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Romanow RJ. Building on values - the future of Health Care in Canada. Final report. Commission on the Future of Health Care in Canada. Ottawa: Government of Canada; 2002.
- 34.Clair M. Les solutions émergentes: Rapport et recommandations. Commission d’étude sur les services de santé et les services sociaux. Québec: Gouvernement du Québec; 2001. [Google Scholar]
- 35.Government of Alberta. Mazankowski D. A framework for reform: Premier’s Advisory Council on Health. 2001. [Google Scholar]
- 36.Government of Ontario . Looking back, looking forward:The Ontario Health Services Restructuring Commission (1996–2000) Toronto: The Ontario Health Services Restructuring Commission; 2000. [Google Scholar]
- 37.Government of Saskatchewan . Caring for Medicare: Sustaining a Quality System. Regina: Commission on Medicare; 2001. [Google Scholar]
- 38.Kirby JL, LeBreton M. The Health of Canadians - The Federal role. Volume 6: Recommendations for Reform. Standing Senate Committee on Social Affairs, Science and Technology. Ottawa: Government of Canada; 2002.
- 39.Statistics Canada . Access to a regular medical doctor—Canadian Community Health Survey 2013. Ottawa: Statistics Canada; 2014. [Google Scholar]
- 40.Talbot Y, Fuller-Thomson E, Tudiver F, Habib Y, McIsaac WJ. Canadians without regular medical doctors. Who are they? Can Fam Physician. 2001;47:58–64. [PMC free article] [PubMed] [Google Scholar]
- 41.Hay C, Pacey M, Bains N, Ardal S. Understanding the unattached population in Ontario: evidence from the Primary Care Access Survey (PCAS) Healthc Policy. 2010;6(2):33–47. [PMC free article] [PubMed] [Google Scholar]
- 42.Loignon C, Allison P, Landry A, Richard L, Brodeur J, Bedos C. Providing humanistic care: dentists' experience in deprived areas. J Dent Res. 2010;89(9):991-5. [DOI] [PubMed]
- 43.Loignon C, Haggerty J, Fortin M, Bedos C, Allen D, Barbeau D. Physicians’ social competence in the provision of care to persons living in poverty: research protocol. BMC Health Serv Res. 2010;10(1):79. doi: 10.1186/1472-6963-10-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Breton M, Gagne J, Gankpé F. Implementing centralized waiting list for patients without family physicians across Québec. Health Reform Observer/Observatoire des Réformes de Santé. 2014;1(2):1–12. [Google Scholar]
- 45.Health Canada. Canada’s Health Care System: Gouvernment of Canada; 2012. Available from: http://www.hc-sc.gc.ca/hcs-sss/pubs/system-regime/2011-hcs-sss/index-eng.php. Accessed 14 Sept 2016.
- 46.Breton M, Ricard J, Walter N. Connecting orphan patients with family physicians: differences among Quebec’s access registries. Can Fam Physician. 2012;58(9):921–2. [PMC free article] [PubMed] [Google Scholar]
- 47.Ontario Ministry of Health and Long-Term Care. Find a family doctor or nurse practitioner: How to find or change a family doctor or nurse practitioner through Health Care Connect. 2015 [2015-11-03]. Available from: http://www.ontario.ca/page/find-family-doctor-or-nurse-practitioner#section-1. Accessed 3 Nov 2015.
- 48.Government of New Brunswick. Patient Connect NB—Frequently asked questions 2013 [2015-11-03]. Available from: https://www.gnb.ca/0217/pdf/2013/patient_connect_faq-e.pdf. Accessed 3 Nov 2015.
- 49.Fédération des médecins omnipraticien du Q, Ministère de la santé et des services s. Guide de gestion relatf à l’application de la Lettre d’entente no 245 (guichets d’accès aux clientèles orphelines). 2013 Contract No.: Report.
- 50.Primary Health Care Branch. INFOBulletin - Changes to Primary Health Care Physician Payments. 2015. Bulletin 1125. Available from: http://www.health.gov.on.ca/en/pro/programs/ohip/bulletins/11000/bul11125.pdf. Accessed 3 Nov 2015.
- 51.Salisbury C, Sampson F, Ridd M, Montgomery AA. How should continuity of care in primary health care be assessed? Br J Gen Pract. 2009;59(561):e134–e41. doi: 10.3399/bjgp09X420257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Ministère de la Santé et des Services S. Cadre de référence provincial des guichets d’accès pour la clientèle sans médecin de famille. 2016.
- 53.Breton M, Brousselle A, Boivin A, Roberge D, Pineault R, Berbiche D. Who gets a family physician through centralized waiting lists? BMC Family Practice. 2015;16(1):10. doi:10.1186/s12875-014-0220-7. [DOI] [PMC free article] [PubMed]
- 54.Ontario Ministry of Health and Long-Term Care. Public Information—Health Care Connect Program Results 2014 [2015-11-03]. Available from: http://www.health.gov.on.ca/en/ms/healthcareconnect/public/results.aspx. Accessed 3 Nov 2015.
- 55.Manitoba Health HLS. Family Doctor Finder Online Registration - Connecting Me to My Primary Care 2015 [2015-11-03]. Available from: https://www.gov.mb.ca/health/familydoctorfinder/register.html. Accessed 3 Nov 2015.
- 56.Gouvernement du Québec. Guichet d’accès à un médecin de famille. 2016. https://www4.prod.ramq.gouv.qc.ca/GRL/LM_GuichAccesMdFamCitoy/fr. Accessed 3 Nov 2015.
- 57.Ionescu-Ittu R, McCusker J, Ciampi A, Vadeboncoeur A-M, Roberge D, Larouche D, et al. Continuity of primary care and emergency department utilization among elderly people. Can Med Assoc J. 2007;177(11):1362–8. doi: 10.1503/cmaj.061615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Manitoba Health Healthy Living & Seniors. Family Doctor Finder Program Results 2015. Available from: http://www.gov.mb.ca/health/familydoctorfinder/stats.html. Accessed 3 Nov 2015.
- 59.Ontario Ministry of H, Long-Term c. Health Care Connect, Program Results. 2012.
- 60.Brousselle A, Champagne F. Program theory evaluation: logic analysis. Eval Program Plann. 2011;34(1):69-78. http://dx.doi.org/10.1016/j.evalprogplan.2010.04.001. [DOI] [PubMed]
- 61.Rey L, Brousselle A, Dedobbeleer N. Logic analysis: testing program theory to better evaluate complex interventions. In: Houle J, Dubois N, Lloyd S, Mercier C, Hartz Z, Brousselle A, editors. L’évaluation des interventions complexes. 26(3): Revue Canadienne d’Évaluation de Programme/Canadian Journal of Program Evaluation; 2012. p. 61–89. [PMC free article] [PubMed]
- 62.Newcomer KE, Hatry HP, Wholey JS. Handbook of practical evaluation: Hoboken: Wiley; 2015.
- 63.Mitchelle P, Lewis V. A Manual to Guide the Development of Local Evaluation Plans. Australian Government Department of Health and Aging. 2003. [Google Scholar]
- 64.Haggerty J, Tamblyn R, Boileau L, Levesque J, Katz A, Russell G. Building Systems-Level Evidence From The Mosaic of 12 Research Programs In The CIHR Signature Initiative On Community Based Primary Health Care. Montreal: Canadian Association of Health Services and Policy Research Conference; 2014. [Google Scholar]
- 65.Bonato S. Google scholar and scopu for finding gray literature publications. J Med Libr Assoc. 2016;104(3):252–4. doi: 10.3163/1536-5050.104.3.021. [DOI] [Google Scholar]
- 66.Maddison P, Jones J, Breslin A, Barton C, Fleur J, Lewis R, et al. Improved access and targeting of musculoskeletal services in northwest Wales: targeted early access to musculoskeletal services (TEAMS) programme. BMJ. 2004;329(7478):1325–7. doi: 10.1136/bmj.329.7478.1325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Attride-Stirling J. Thematic networks: an analytic tool for qualitative research. Qual Res. 2001;1(3):385–405. doi: 10.1177/146879410100100307. [DOI] [Google Scholar]
- 68.Wong G, Greenhalg T, Westhorp G, Buckingham J, Pawson R. RAMESES publication standards: realist syntheses. BMC Med. 2013;11(1):1. doi: 10.1186/1741-7015-11-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Greenhalgh T, Wong G, Westhorp G, Pawson R. Protocol-realist and meta-narrative evidence synthesis: evolving standards (RAMESES) BMC Med Res Methodol. 2011;11(1):115. doi: 10.1186/1471-2288-11-115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Dixon-Woods M, Cavers D, Agarwal S, Annandale E, Arthur A, Harvey J, et al. Conducting a critical interpretive synthesis of the literature on access to healthcare by vulnerable groups. BMC Med Res Methodol. 2006;6(1):1–13. doi: 10.1186/1471-2288-6-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Donaldson SI. Theory-Driven Program Evaluation in the New Millenium. In: Donaldson SI, Scriven M, editors. Evaluating Social Programs and Problems: Visions for the new millenium. Mahwah, NJ: Lawrence Erlbaum Associates; 2003. pp. 109–41. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable.