

Description
A young man was evaluated because of progressive weakness in both hands since 2 years. He played sport on a high level and experienced difficulties in catching the ball. Flexion of the neck caused paresthesias and an electric shock like sensation in both arms. He experienced muscle cramps during cold.
Neurological examination revealed almost symmetrical atrophy of the interosseous, thenar and hypothenar muscles without fasciculations and with weakness of these muscles and the distal extensor muscles, sparing the brachioradialis. There was no weakness of the proximal muscles of both arms. The reflexes were normal. There were no signs of a pyramidal syndrome. The examination of the legs, cranial nerves and sensibility was unremarkable.
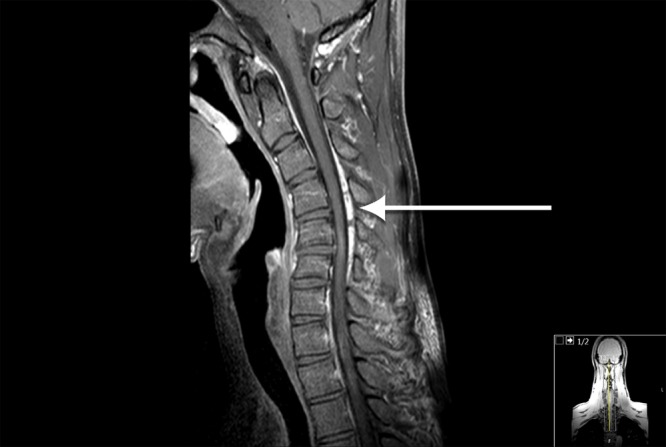
The paresthesias during flexion of the neck suggested a cervical myelopathy, but the distribution of the muscle weakness suggested a neuromuscular disorder within the differential diagnosis, an anterior horn cell disease, multifocal motor neuropathy (weakness is usually asymmetric, but relative symmetry has been described) or a distal myopathy. Extensively nerve conduction studies showed prolonged distal motor latencies of the median and ulnar nerve and spontaneous muscle activity of the small muscles of the hand and forearm on both sides. Distal sensory latencies and the sensory nerve action potentials were normal. The findings were insufficient to diagnose multifocal motor neuropathy or anterior horn cell disease. A cervical MRI was performed and showed a myelopathy and cord atrophy at the C4–C7 level (figure 1). The cause of the myelopathy was not clear. In addition, a cervical MRI in flexion was performed and showed enlarging of the epidural space with a contrast enhancing epidural mass due to loss of attachment of the posterior dura (figure 2).
Figure 1.

Myelopathy and cord atrophy at the C4–C7 level.
Figure 2.
MRI in flexion shows enlarging of the epidural space.
This MRI in flexion with enlarging of the epidural space is a classical sign for Hirayama disease, a rare cervical myelopathy, caused by spinal cord compression during flexing the neck. Owing to progression of distal weakness of both arms, the patient was referred to a neurosurgeon and underwent anterior decompression and fusion of level C5, C6 and C7. Afterwards, the patient did not have the symptoms of paresthesias while flexing the neck anymore. The weakness and atrophy in both hands stabilised.
Hirayama disease is a self-limiting disease.1 The disease progresses in a few years and usually stabilises within 5 years. In a small number of patients, the disease still progresses and in selected patients surgery may be beneficial. It is mainly reported in Asian countries, and men are more often affected than women. It is a rare cervical myelopathy mainly affecting muscles innervated by the C7, C8 and T1 spinal roots. In the majority of patients, there is a unilateral onset, bilateral symmetrical involvement, like in our patient, is less common. There are no sensory symptoms. The symptoms are due to compression of the anterior horn cells. Hirayama disease is diagnosed by a cervical MRI in flexion with gadolinium. Typical findings on MRI are anterior shifting of the posterior dura, with flattening of the spinal cord and a contrast enhancing posterior cervical epidural space as seen in our patient.2
Learning points.
In case of an unexplained cervical myelopathy, additional MRI in flexion should be performed to rule out Hirayama disease.
The clinical presentation with pure motor symptoms is suggestive for anterior horn cell disease; the usually non-progressive course and a dynamic MRI are the clue to diagnosis.
Footnotes
Contributors: MS contributed to drafting/revising the manuscript. FB involved in revising the manuscript and provided MRI images. LV drafted/revised the manuscript.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Sitt CM, Fung LW, Yuen HY et al. Hirayama disease in a 17-year-old Chinese man. Singapore Med J 2014;55:e87–9. doi:10.11622/smedj.2013253 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Foster E, Tsang BK, Kam A et al. Hirayama disease. J Clin Neurosci 2015;22: 951–4. doi:10.1016/j.jocn.2014.11.025 [DOI] [PubMed] [Google Scholar]