

Abstract
Background
The purpose of this study was to determine the clinical outcomes and objective measures of function that can be expected for patients following the Bridle procedure (modification of the posterior tibial tendon transfer) for the treatment of foot drop.
Methods
Nineteen patients treated with a Bridle procedure and 10 matched controls were evaluated. The Bridle group had preoperative and two year postoperative radiographic foot alignment measurements and completion of the Foot and Ankle Ability Measure (FAAM). At followup both groups were tested with the star-excursion test for standing balance, ankle plantarflexion and dorsiflexion isokinetic strength and the AOFAS and Stanmore outcome measures were collected only on the Bridle patients.
Results
There was no change in the radiographic foot alignment measures from pre- to postoperative. FAAM subscales of activities of daily living and sport, AOFAS and Stanmore scores were all reduced in Bridle patients compared to controls. Single limb standing balance reaching distance in the anterolateral and posterolateral directions were reduced in Bridle participants compared to controls (p<.03). Isokinetic ankle dorsiflexion and plantarflexion strength was lower in Bridle participants (2 ± 4 ft*lbs, 44± 16 ft*lbs) compared to controls (18± 13 ft*lbs, 65 ± 27 ft*lbs, p<.02). All Bridle participants reported excellent to good outcomes and would repeat the operation. No patient wore an ankle foot orthosis (AFO) for everyday activities.
Conclusion
The Bridle procedure is a successful surgery that does not restore normal strength and balance to the foot and ankle but allows individuals with foot drop and a functional tibialis posterior muscle to have significantly improved outcomes and discontinue the use of an AFO. In addition, there is no indication that loss of the normal function of the tibialis posterior muscle results in change in foot alignment 2 years after surgery.
Level of Evidence
III
Keywords: Bridle, Foot Drop, Peroneal Nerve, Tendon Transfer, Tibialis posterior Tendon
INTRODUCTION
Peroneal nerve injury is the most frequently encountered mononeuropathy in the lower extremity and a common cause of trauma induced foot drop.14 Injury to the common peroneal nerve results in loss of function of the anterior and often the lateral compartment musculature of the leg and results in foot drop and a steppage gate.26 The nerve can either be injured by direct compression or traction. Common modes of injury include fractures about the knee, significant knee ligament injuries or dislocations and compression or traction injuries as a complication of total knee or total hip surgery. Although an ankle-foot-orthosis (AFO) with a fixed ankle or dorsiflexion assist ankle joint will improve function, it is often poorly tolerated in the younger, active population.
Although there has been limited success with nerve transfer for foot drop, the current standard for operative restoration of functional dorsiflexion in individuals with a peroneal nerve palsy is dynamic tendon transposition.4 Putti, in 1914, is credited as being the first to transfer the tibialis posterior tendon anteriorly through the interosseus membrane to the dorsum of the foot to restore dorsiflexion.11 In 1954, Watkins et al. reported ‘good’ or ‘excellent’ results in 24 out of 25 patients using this technique.25 There have been many modifications of the tibialis posterior tendon transfer technique that have been subsequently described in the literature. Specifically, the Bridle procedure was designed to address under or over correction of coronal plane position resulting from the surgeon choosing a point of attachment of the tibialis posterior tendon that was either too far lateral or too far medial, especially in the individual with spasticity. By adding two additional tendons to form an anastomosis of tendons with balanced attachment points on the foot, the pull of the tibialis posterior tendon was distributed more evenly to the dorsum of the foot thereby avoiding a varus or valgus deformity from tendon overpull. This modification avoided the need for a triple arthrodesis or other procedure to stabilize the foot in neutral.
The purpose of this study is to provide a detailed description of the Bridle technique and evaluate the outcomes of the procedure for traumatic peroneal nerve injury using clinical outcome measurements and objective physical function tests and strength measures to evaluate postoperative function. Given reports of acquired deformity following tibialis posterior tendon transfer, a second aim is to determine if any postoperative deformity occurred through evaluation of standardized radiographic measurements.13,23,24,27
MATERIALS AND METHODS
This is a retrospective case-control study. Institutional review board approval and consent was obtained from all participants. Participants were included who had undergone a Bridle procedure by one of two surgeons (XXX or YYY) for the treatment of foot drop caused by a traumatic isolated peroneal nerve injury from 7/1/2005 to 4/1/2010, providing for a one year minimum followup. Exclusion criteria included a concomitant diagnosis of neuromuscular disease, a partial common peroneal nerve palsy with 3/5 (antigravity) or greater strength in ankle dorsiflexion, tibial nerve palsy with posterior tibialis muscle weakness of 4/5 or less, non-ambulatory patients or a patient that utilized a walking aid prior to peroneal nerve injury. Ten participants without a history of foot or ankle injury were enrolled as a control group and were age, gender, height and weight matched to our study participants.
All participants who met the inclusion criteria had an initial trial of nonoperative management. Some participants also underwent prior procedures such as peroneal neurolysis or nerve repair or grafting either acutely or delayed. After failure of return of nerve function, those individuals with a traumatic foot drop underwent a Bridle procedure to restore foot dorsiflexion.
Operative Procedure and Postoperative Management
The Bridle procedure performed in this group of participants was similar to the Rodgriquez modification of the original Bridle procedure as described by McCall, et al., but modified by Rodriquez in two important details.12,20 Instead of a “subcutaneous” transfer of the tibialis posterior tendon at the anterior ankle, the tendon was transferred beneath the extensor retinaculum. Secondly, the tibialis posterior tendon was secured to the 2nd cuneiform with an interference screw rather than sutures, staples or a loop through the bone.7
First, a gastrocnemius-soleus lengthening was performed through an incision on the posterior medial calf on all participants who demonstrated a lack of passive ankle joint dorsiflexion of at least 5 degrees with the knee in extension. A Silfverskiöld test was performed to determine whether the gastrocnemius and soleus or just the gastrocnemius alone required lengthening.21
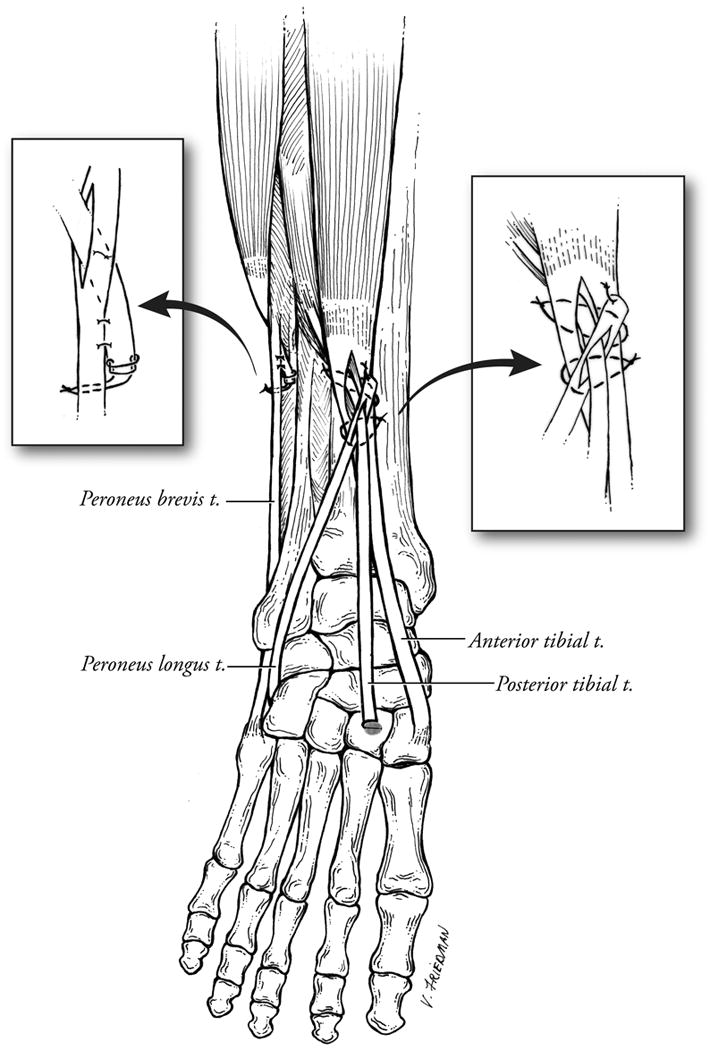
Second, the tibialis posterior tendon was detached from its insertion on the navicular tuberosity, the often bulbus distal end was trimmed to the caliber of the remaining tendon and a grasping suture applied. A third incision was made along the posterior medial border of the distal tibia to expose the tibialis posterior tendon in the deep posterior compartment. The tibialis posterior tendon was delivered into this incision. A fourth incision was made over the tibialis anterior tendon just lateral to the tibial crest and above the ankle extensor retinaculum. All the contents of the anterior compartment were retracted laterally along with the tibialis anterior tendon to expose the interosseous membrane. Using a blunt Kelly clamp the interosseous membrane was pierced and the clamp was opened to create a slit in the membrane. This slit was then extended by blunt dissection distally as far as possible and proximally at least 10 to 15 cm to allow adequate space for transfer of the posterior tibialis muscle belly. The distal end of the tibialis posterior tendon was then transferred around the posterior surface of the tibia, through the opening in the interosseus membrane and into the anterior compartment. While performing this maneuver, great care is taken to avoid incarcerating or strangulating any of the components of the posterior compartment against the tibia as the tibialis posterior tendon is pulled through the interosseous membrane. A fifth incision was made over the peroneal tendons along the lateral aspect of the distal leg. The peroneus longus tendon was transected in the distal third of the leg and the proximal end sutured into the peroneus brevis if the lateral compartment muscles were functional. If the peroneals were nonfunctional, the proximal end of the peroneus longus was allowed to retract. A sixth incision was made over the peroneus brevis tendon, proximal to the base of the 5th metatarsal. The peroneus longus tendon was located inferior to the brevis tendon and pulled distally into this wound where a grasping suture was applied to the end. The distal end of the peroneus longus tendon was passed through a slit in the distal peroneus brevis tendon and was then subcutaneously transferred in front of the fibula and under the extensor retinaculum into the anterior compartment alongside the tibialis anterior and transferred tibialis posterior tendons. A seventh incision was made over the dorsum of the foot centered over the third cuneiform. The long extensor tendons were retracted laterally and the muscle fibers of the extensor brevis were split and retracted medially along with the deep peroneal nerve and dorsalis pedis artery to expose the dorsum of the 2nd cuneiform. Using the C arm, the middle of the 2nd cuneiform is identified and a drill hole (the same diameter as the distal posterior tendon) was made from dorsal to plantar through the bone. The free distal end of the tibialis posterior tendon was passed through slits in the tibialis anterior tendon and the peroneus longus tendon before it was passed under the extensor retinaculum of the ankle and onto the dorsum of the foot into the area of the 2nd cuneiform drill hole. A straight needle was used to pass the sutures in the tibialis posterior tendon through the drill hole and out the skin on the plantar foot. The foot was then placed in neutral to slight dorsiflexion and the tibialis posterior tendon was then pulled distally into the cuneiform hole and tensioned to approximately 80% of its excursion and fixed in the 2nd cuneiform with an interference screw. Tensioning of the three tendon anastomosis was done superior to the ankle extensor retinaculum by pulling cephalad on the tibialis anterior and peroneus longus tendons to place equal tension on these medial and lateral stabilizing limbs of the transfer. Non-absorbable sutures were placed to secure these tendons to the tibialis posterior tendon and to each other where they crossed through the slits in the tendons.
Postoperatively, the patient was placed into a well-padded short-leg non-weightbearing cast holding the ankle in neutral. The cast was bi-valved in the operating room to prevent complications from swelling. Strict foot elevation was emphasized. The cast and skin sutures were removed at 10 to 14 days and the foot was held in neutral while another synthetic cast was applied. Touch weightbearing was allowed for the next four weeks. The cast was removed at 6 weeks postoperative and the patient was placed into a removable walker boot and allowed to progress to full weightbearing as tolerated. Physical therapy was begun at this time for re-education of the tibialis posterior tendon transfer with active and active assisted dorsiflexion and active plantar flexion. Precautions were given for avoidance of passive ankle joint plantarflexion until 3 months postoperative. A night splint was worn until 3 months postoperative to prevent premature stretching out of the transfer. As swelling improved, a custom molded AFO was fabricated or the patient’s former foot drop AFO was worn in an athletic shoe to allow earlier discontinuation of the walker boot. The custom AFO or walker boot was used until at least 3 months postoperative or until strength allowed discontinuation of the brace.
Outcome Variables
Patient History
Descriptive analysis of the participant sample was obtained from a chart review and history taken during testing including the following: gender, age, etiology/mechanism of injury, site of injury (hip/pelvis or knee), preoperative nerve testing (if obtained) and attempted neurolysis, associated injuries, additional or prior procedures for associated injuries (including ligament and bony reconstructions for associated injuries), manual dorsiflexion and plantarflexion strength on a scale of 0 to 5, and passive dorsiflexion range of motion. Operative records were reviewed to identify additional procedures performed on the affected foot, intraoperative or postoperative complications and the tourniquet time if used.
Outcome Measures
All participants completed a questionnaire measuring multiple outcome variables. Independent examiners administered these questionnaires. Participants completed the Foot and Ankle Ability Measure (FAAM),10 which asks perception of difficulty completing activities of daily living and sport (e.g., walking on even ground, walking up hills, stepping up and down curbs, running, cutting), the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Scale, and the Stanmore system questionnaire.28 The latter is a measure that is specific for outcome evaluation after tendon transfer.9 Participants are considered to have excellent functional results with a Stanmore score of 85 to 100, good results if their score is 70 to 84, fair results if the score is 55 to 69 and poor results if the score is less than 55.10
The patient questionnaire also assessed the current level of function and satisfaction with questions regarding: subjective current activity and pain levels using 0 to 10 point visual analogue scales (VAS), current use of AFO and any assist devices (including their frequency), and overall satisfaction with the procedure. The participants self-rated the results of the surgery on a scale of: excellent, good, fair, or poor.
Range of Motion
Passive dorsiflexion with knee extended and flexed, plantarflexion, subtalar joint inversion, subtalar joint eversion, and great toe extension range of motion were measured by a single experienced physical therapist using a universal full-circle goniometer as previously described.5 The subjects were positioned prone with the hip extended and ankles off the end of the table. Dorsiflexion range of motion with the knee extended and flexed to 90 degrees was measured with the axis of the goniometer placed over the lateral malleolus with the moveable arm aligned with the fifth metatarsal shaft and the stationary arm aligned with the fibula.2 Subtalar joint inversion and eversion were measured with the stationary arm bisecting the leg and the moveable arm aligned with the bisection of the calcaneus. Great toe extension range of motion was measured with the stationary arm bisecting the medial side of the 1st metatarsal and the moveable arm bisecting the proximal phalanx of the great toe.
Muscle Strength
Ankle dorsiflexion and plantarflexor strength was assessed using the Biodex System 3 (Biodex Medical Systems, Shirley, New York) Pro Orthopedic Testing & Rehabilitation dynamometer at 60°/sec.15 Three trials were completed and the peak torque was averaged from the three trials.
Star Excursion Balance Measure
The Star excursion for distance test was used to assess standing balance.8,18 The participant stood on the involved side and reached with the opposite leg as far as possible anterolateral, lateral, and posterolateral directions. The participant lightly touched the furthest point possible on a tape-ruled line and then returned to a bilateral stance. The distance from the center of the grid to the touch point was measured in centimeters and normalized to the participant’s leg length.
Radiographic Alignment
Standing anteroposterior (AP) and lateral ankle/foot radiographs were obtained in a standardized manner and were evaluated electronically in blinded fashion by the senior author (XXX.) using a precise and reproducible methodology previously reported.6 Sixteen of the Bridle participants had standardized standing preoperative radiographs that were compared to postoperative films. The lateral view x-rays were evaluated for sagittal plane deformity by measuring the cuboid height (distance of the plantar most aspect of the cuboid to a line joining the plantar 5th metatarsal head to the plantar calcaneus), Meary’s angle (angle between the line bisecting the talar head and neck with the line through the longitudinal axis of the 1st metatarsal, positive values representing apex dorsal), and the calcaneal pitch (angle of plantar cortex of the anterior calcaneus, not including the calcaneal tuberosity, relative to the line from the plantar surface of the calcaneus to the 5th metatarsal head). Transverse plane alignment was measured using Kite’s angle.6
Statistical Analysis
For measurements obtained for both limbs, designation of the “involved” and “uninvolved” side for the control sample was randomly selected and designed to achieve an equivalent proportion of left and right sides to that found in the Bridle group.
Participant characteristics between groups were compared using an unpaired t-test for age and Fisher’s Exact test for sex and race. An analysis of variance was performed to assess the similarity of the involved side for the Bridle and control groups for the majority of the following measures: range of motion, muscle strength, balance, and radiographic alignment. Due to violations of the assumptions required for the statistical method used, for dorsiflexion knee flexed ROM, great toe extension ROM, subtalar joint inversion and eversion, ankle dorsiflexion strength and transverse plane alignment required rank transformation prior to analysis.
Wilcoxon’s rank sum test was used as a nonparametric alternative for between group comparison of the FAAM, AOFAS and Stanmore questionnaires. Paired t-tests were performed to assess differences between preoperative and postoperative FAAM, transverse plane alignment, and Meary’s angle. A non-parametric signed rank test was used to compare the preoperative and postoperative cuboid height and calcaneal pitch.
Within the Bridle participant group, Spearman correlations and associated p-values were used to assess the association of select continuous variables with the FAAM (total percent activities of daily living (ADL) and total percent sport). The associations of certain characteristics and FAAM scores were assessed with unpaired t-tests or Wilcoxon’s test. The data analysis was generated using the SAS System (SAS Institute Inc., Cary, NC, USA). A p-value of ≤.05 was considered significant for all comparisons.
RESULTS
The Bridle procedure was performed on 42 individuals from 2005–2011, 30 of these participants met study inclusion criteria (>1 year followup and foot drop related to traumatic, isolated neurologic deficit). Nineteen Bridle participants (14 males, 5 females) and 10 matched controls (7 males, 3 females) agreed to participate and were evaluated with performance-based and self-reported measures of function at an average followup of 1.9 years (st. dev 0.8). Demographic data is presented in Table 1.
Table 1.
Demographic Data
| Bridle n=19 |
Control n=10 |
P Value | |
|---|---|---|---|
| Age | 40 ± 17 | 44 ± 22 | .61 |
| Sex (M/F) | 14/5 | 7/3 | 1.0 |
| Involved Side (Right/Left) | 10/9 | 6/4 | 1.0 |
| AFO Use Post-operatively (Yes/no) | 2/17 | 0/10 |
Descriptive Analysis
Five Bridle participants had an injury at the level of the hip, while 14 had an injury at the level of the knee. Ten of the Bridle participants required knee ligament reconstruction/stabilization secondary to the initial injury. Three participants required pelvic and/or femoral stabilization, one required isolated femoral stabilization, and one required operative tibial stabilization as a result of the initial injury. Two participants had a nerve injury as a complication of a hip arthroplasty and one participant had a nerve palsy as a complication of a Baker’s cyst removal. Two participants did not have other lower extremity reconstructive procedures and the injury was a result of a gunshot in one and stretch injury from a fall in the other. Sixteen of the nineteen Bridle participants had a previously attempted neurolysis of the peroneal nerve at the level of the knee, despite injury location.
Preoperative manual dorsiflexion strength prior to the Bridle procedure was 0 out of 5 in all participants with average passive dorsiflexion of 1 degree. Six participants had concomitant procedures at the time of their Bridle. One had hardware removal from the ankle, 2 had lateral ankle ligament reconstruction, 1 had a flatfoot reconstruction, 1 had a dorsiflexion 1st metatarsal osteotomy with valgus producing calcaneus osteotomy, 1 had a great toe inter-phalangeal joint fusion, and 1 had exostosis resection. Sixteen of the nineteen participants required a gastrocnemius-soleus lengthening during the procedure.
There were no intraoperative complications. Four months postoperatively, one participant ruptured the tibialis posterior tendon at the anterior ankle requiring revision with repair and augmentation with the peroneus tertius tendon. This participant initially had the peroneus longus tendon woven through a split in the tibialis posterior tendon which may have weakened the tibialis posterior tendon predisposing it to rupture. This occurred early in the series and the majority of participants underwent a slightly modified technique as described above where the posterior tibialis is woven through a slit in the peroneus longus.
Outcome Scores
The average postoperative FAAM activities of daily living(ADL) subsection score for the Bridle group was significantly lower than controls (87± 12% compared to 99±% for controls, p<.01). For the sport subsection, the Bridle’s scored 65±17% compared to 98% ± for controls (p<.01). Ten Bridle group participants had completed preoperative FAAM questionnaires and were compared to their postoperative scores. The ADL and sports subsection scores demonstrated a significant improvement from preoperative to postoperative (ADL: 67±17% vs 86±9% and Sports: 22±16% vs 59±18%, respectively, p<.01).
No correlation was found between FAAM scores and age, location of injury, gastroc-soleus lengthening, plantarflexor strength or dorsiflexion ROM.
The average AOFAS score was 80 ±13 for the Bridle group compared to 96 ±5 for controls (p<.01). Average Stanmore scores for the Bridle group were 78 ±14 (good result) and 98 ± 3% (excellent) for the controls (p<.01).
Subjective Outcomes
All Bridle participants reported that they were satisfied with the procedure (19 of 19). Twelve participants reported an “excellent” outcome and 7 had a “good” self-reported outcome. The average VAS pain score was 2.7. No participant required the use of an AFO for everyday activities; however, 2 participants reported use of an AFO for athletic activities.
Objective Testing
Plantarflexion range of motion was significantly reduced in the Bridle group (30 degrees ± 10) compared to controls (39 degrees ± 8, p < .01). (Table 2) Dorsiflexion and plantarflexion strength were significantly reduced in the Bridles versus the controls (dorsiflexion: 2 ± 4 vs 18 ± 13 ft. lbs, plantarflexion:(44 ± 16 vs 65 ± 27 ft. lbs, p < .02) (Table 2). Standing balance as measured by the star excursion test was reduced in Bridle participants compared to controls in all directions of reach. (p < .05) (Table 2).
Table 2.
Study Measure Comparisons (mean ± standard deviation)
| Bridle n=19 |
Control n=10 |
P Value | |
|---|---|---|---|
| Range of Motion (degrees) | |||
| Dorsiflexion Knee extended | 8 ± 5 | 8 ± 5 | .28 |
| Dorsiflexion Knee Flexed | 13 ± 4 | 14 ± 3 | .35 |
| Plantarflexion | 30 ± 10 | 39 ± 8 | .01 |
| Great Toe Extension | 50 ± 16 | 61 ± 16 | .11 |
| Subtalar Joint Eversion | 7 ± 2 | 7 ± 2 | .75 |
| Subtalar Joint Inversion | 12 ± 4 | 15 ± 4 | .07 |
| Strength (Peak Torque, ft-lbs) | |||
| Ankle Dorsiflexion | 2 ± 4 | 18 ± 13 | <.01 |
| Ankle Plantarflexion | 44 ± 16 | 65 ± 27 | .02 |
| Star Excursion Balance Test (reach distance normalized to leg length) | |||
| Antero-lateral | .77 ± .08 | .85 ±.09 | .03 |
| Lateral (out to side) | .77 ± .12 | .85 ± .09 | .05 |
| Postero-lateral | .78± .12 | .90 ± .11 | .02 |
| Radiographic Alignment (Postoperative versus Control) | |||
| Meary’s Angle (degrees) | −6 ± 7 | −3 ± 5 | .26 |
| Cuboid (mm) | 12 ± 3 | 13 ± 3 | .61 |
| Calcaneal Pitch (degrees) | 21± 5 | 24 ± 4 | .94 |
| Transverse Plane (degrees) | 2 ± 6 | 6 ± 8 | .16 |
| Radiographic Alignment (Pre- versus Postoperative Bridles) | |||
| Bridle Pre-operative n=16 |
Bridle Post-operative n=16 |
P value | |
| Meary’s (degrees) | −4 ± 8 | −6 ± 6 | .21 |
| Cuboid (mm) | 13 ± 3 | 12 ± 3 | .80 |
| Calcaneal Pitch (degrees) | 22 ± 5 | 22 ± 5 | .26 |
| Transverse Plane (degrees) | 0 ± 8 | 1 ± 7 | .48 |
Radiographic Analysis
There were no significant differences found between the pre- and postoperative radiographs. There were no differences between the postoperative measures of the Bridle participants and the controls. (Table 2)
DISCUSSION
The first clinical series of the Bridle procedure, was reported in 1991 by McCall, et al who attributed this technique to D. C. Riordan, MD and Paul Brand, MD for the treatment of the equinus and equinovarus deformities associated with cerebral palsy, Charcot Marie Tooth Disease, Guillain-Barre’ disease, lumbar myelodysplasia and peroneal nerve injury. In total, 128 Bridle procedures were performed on 101 patients. Eighty of the 101 patients had cerebral palsy and only 2 had a peroneal nerve injury. The procedure was initially described as an anterior transfer of the tibialis posterior tendon through the interosseous membrane and subcutaneous transfer of the distal stump of the peroneus longus tendon over the anterior ankle with a tri-tendon anastomosis between the tibialis posterior, tibialis anterior, and peroneus longus tendons in the distal leg above the ankle extensor retinaculum and an Achilles tendon lengthening.12 Approximately 75% of all individuals had a good or excellent result, with the cerebral palsy group faring the best with 80% good to excellent results despite only 74% of them becoming brace free postoperatively. There was an overall 21% complication rate of which a calcaneus deformity was the most common, especially in the cerebral palsy group requiring 12 re-operations. There were four cases of an acquired pes planovalgus deformity following the Bridle in the cerebral palsy group, all of which required a hindfoot arthrodesis.
The procedure was later modified by Rodriguez to include a transfer of the insertion of the tibialis posterior tendon into the second cuneiform to provide a secure tendon to bone insertion and a direct line of pull. He reported on 10 patients, all who became brace free.20 Prahinski, et al reported on 10 patients with 5 year followup who underwent the traditional Riordan technique as described by McCall and reported only 4 of 10 excellent long-term results due to problems with acute or chronic stretching out of the tendon-to-tendon connection and resultant decrease in active dorsiflexion.12,19 These previous small case series provide useful information but few details of the operative technique are reported. Clinical outcomes and objective measures are rarely discussed.
The results of this case controlled study support the use of the Bridle procedure to restore ankle dorsiflexion function and strength for treatment of traumatic foot drop in the setting of a peroneal nerve injury. The satisfaction rate was high with 100% good or excellent self- reported outcomes and 100% were brace free for normal daily activities or walking, although 2 of 19 required an AFO for athletic activities.
Using standardized weightbearing radiographs, this study is the first to confirm that there were no changes in static stance foot alignment measures 2 years postoperative. There is concern from previous reports that loss of the tibialis posterior as a support for the longitudinal arch and inverter of the foot, may lead to changes similar to those seen in adult-acquired flatfoot, exhibited by an increased calcaneal eversion, decreased plantarflexion of the forefoot, and lowering of the arch.16,17,22 Previous studies using visual appraisal and plantar pressure assessment found 6% to 30% of individuals had increases in medial plantar pressure and 8% to19% of individuals had an increase in calcaneal valgus or other alignment associated with a flatfoot.13,23,24,27 Worsening in bony alignment was not found in this study. Our findings do not support a risk for loss of arch height after this procedure.
The Bridle procedure improved both the average sports and ADL subsections of the FAAM by 19% and 37%, respectively. However, despite this improvement, the postop FAAM scores were significantly lower in the Bridle group for both ADL and sport subsection when compared to the matched controls.
There is only one prior report on the Bridle procedure using the technique described in this study which included patients with foot drop from multiple etiologies. Rodriquez reported on 11 procedures in 10 feet for various causes of foot drop.20 All were brace free at an average of 6 ½ years followup, and he found better results with regards to degree of active dorsiflexion in those patients with a traumatic etiology .20 Although Rodriguez did not report his results using validated outcome measures, objective testing or comparison with controls, the results were similar to this current study. All 19 Bridle participants in our study were brace free for their normal daily activities.
Previous reports on this procedure have described similar outcomes. In 1967, Carayon et al. reported ‘good’ or ‘excellent’ results in 22 out of 31 patients with a dual transfer (tibialis posterior tendon to tibialis anterior tendon and the flexor digitorum longus tendon to both the extensor hallucis longus and extensor digitorum longus tendons).1 Vigasio et al. recently reported on a modification of this procedure in which the tibialis anterior insertion was changed to the third cuneiform to provide an optimal traction line for maximal dorsiflexion. At 2 years followup, 81% of their patients exceeded 0 degree dorsiflexion and had a balanced foot posture and 87.5% had abandoned the use of an AFO.24 These authors also transferred the flexor digitorum longus tendon to the extensor hallucis longus and the extensor digitorum longus.24
Prahinski et al. reported on outcomes at an average 5-year followup after the Riordan procedure in 10 soldiers (8 of whom had traumatic peroneal nerve injury). They found that while 5 patients returned to running initially, only 2 were able to keep running. While 9 patients were brace-free initially, only 5 remained so at final followup. Only 3 patients returned to active duty with 2 having no detectable problems during the swing phase of walking. They concluded that while the Riordan transfer technique using a tendon to tendon anastomosis works well in patients with low demands, it may stretch out to failure in patients with high demands.19 Using a tendon to bone attachment for the tibialis posterior tendon in our technique has shown no loss of function over time, but our follow-up was shorter.
In a study by Yeap et al, which reported on 12 patients with either traumatic common peroneal or sciatic nerve injury, 11 of 12 patients had grade 4 or 5 dorsiflexion, but the torque generated by the transferred tendon was only about 30% that of the normal contralateral side. We found that our patients had 18% of torque in dorsiflexion at 60 degrees/second. While data was not presented on return to activity in this current study, Yeap, et al noted in their discussion that one patient did compete in a triathlon.27,28
Decreased plantarflexion ankle range of motion and plantarflexion strength was noted in the Bridle participants compared to controls and this has also been noted in kinematic studies following the Bridle procedure as well as following the T-SPOTT tibialis posterior tendon transfer.3,7 It is unknown whether these findings are related to a tethering effect of the posterior tibialis muscle which has a shorter excursion than the anterior tibialis, weakness of the gastroc-soleus complex following surgical lengthening, plantarflexor muscle weakness secondary to an occult tibial nerve injury that occurred at the time of the peroneal nerve injury or cast and brace immobilization or a combination of these causes. Based on these findings, we emphasize protected range of motion at 6 weeks and early calf muscle strengthening postoperatively. If the patient cannot achieve at least 5 degrees of ankle joint dorsiflexion with the knee in extension preoperatively, we encourage preoperative aggressive calf muscle stretching exercises in hopes of avoiding a gastroc-soleus muscle lengthening.
Our study is not without limitations. It is retrospective in nature and although many participants had preoperative data that was useful in evaluating the impact of this operation, not all of the participants had preoperative data for comparison. Additionally, we were only able to evaluate 19 of the 30 participants who met the inclusion criteria. Our study group was also relatively heterogeneous in nature with multiple sites of nerve injury, different mechanisms of injury and a wide age range.
Despite these limitations, we present a detailed description of the Bridle technique and a thorough postoperative evaluation of a group of participants with a difficult problem. Postoperative evaluation was standardized in all regards, and the Bridle procedure was performed by two surgeons at one site in identical fashion with a standardized postoperative treatment and rehabilitation protocol.
CONCLUSION
In conclusion, the Bridle procedure resulted in 100% satisfaction (12 excellent and 7 good) and provided a significant improvement in both the ADL and sports subsections of the FAAM without negatively impacting foot alignment measures. Despite deficits in ROM, strength, and validated outcome measures when compared to normal controls, the Bridle procedure results in a high level of function in patients with foot drop as a result of peroneal nerve injury. Postoperatively, no participant required an AFO for walking.
Figure 1.
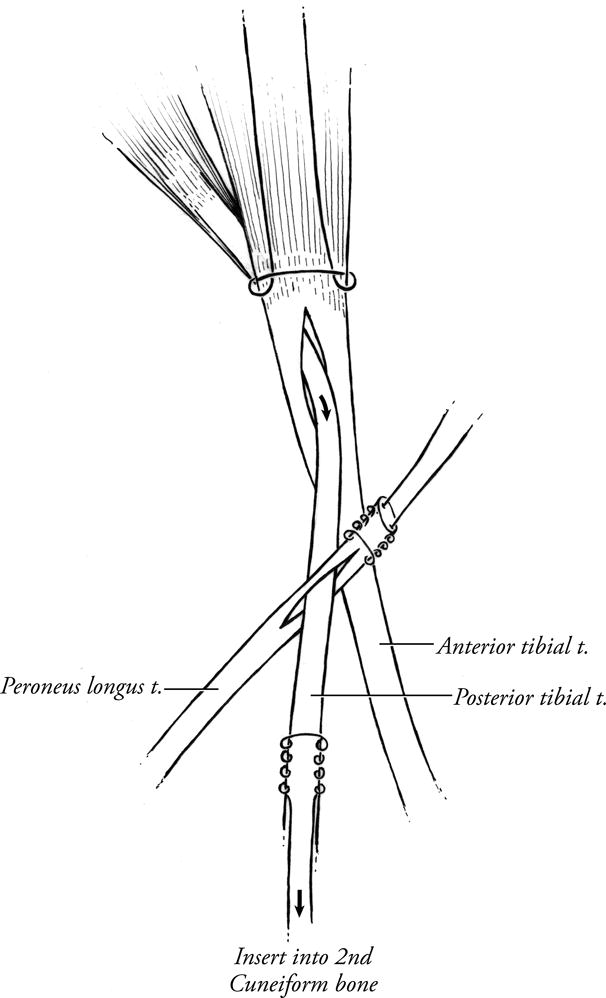


Figure 2.

Acknowledgments
SOURCE OF FUNDING
This study was supported through a grant from the Midwest Stone Institute (XXX, PI) and the National Institute of Healthy:
Contributor Information
Jeffrey E. Johnson, Department of Orthopaedic Surgery, Washington University School of Medicine in St. Louis, MO, 660 South Euclid Avenue, Campus Box 8233-OC, St Louis, Missouri 63110, Phone: 314-514-3566, Fax: 314-514-3689.
E. Scott Paxton, Brown University, University Orthopedics, 2 Dudley St, Suite 200, Providence, RI 02905, 314-960-9448.
Julienne Lippe, St. Louis Orthopedic Institute, 12855 North Forty Drive, Suite 125N, St. Louis, MO 63141, 314-484-6696.
Kay Bohnert, Washington University School of Medicine, Program in Physical Therapy, Campus Box 8502, 4444 Forest Park Blvd, Room 1101, St. Louis, MO 63108, Phone: (314) 286-1433, Fax: (314) 286-1410, Phone: 314.362.2407.
David R. Sinacore, Washington University School of Medicine, Program in Physical Therapy, Campus Box 8502, 4444 Forest Park Blvd, Room 1101, St. Louis, MO 63108, Phone: (314) 286-1433, Fax: (314) 286-1410.
Mary K Hastings, Washington University School of Medicine, Program in Physical Therapy, Campus Box 8502, 4444 Forest Park Blvd, Room 1101, St. Louis, MO 63108, Phone: (314) 286-1433, Fax: (314) 286-1410.
Jeremy J. McCormick, Department of Orthopaedic Surgery, Washington University School of Medicine in St. Louis, MO, 660 South Euclid Avenue, Campus Box 8233-OC, St Louis, Missouri 63110, Phone: 314-514-3566, Fax: 314-514-3689.
Sandra E. Klein, Department of Orthopaedic Surgery, Washington University School of Medicine in St. Louis, MO, 660 South Euclid Avenue, Campus Box 8233-OC, St Louis, Missouri 63110, Phone: 314-514-3566, Fax: 314-514-3689.
References
- 1.Carayon A, Bourrel P, Bourges M, Touze M. Dual transfer of the posterior tibial and flexor digitorum longus tendons for drop foot. Report of thirty-one cases. J Bone Joint Surg Am. 1967;49(1):144–8. [PubMed] [Google Scholar]
- 2.Diamond JE, Mueller MJ, Delitto A, Sinacore DR. Reliability of a diabetic foot evaluation. Phys Ther. 1989;69(10):797–802. doi: 10.1093/ptj/69.10.797. [DOI] [PubMed] [Google Scholar]
- 3.Dreher T, Wolf SI, Heitzmann D, et al. Tibialis posterior tendon transfer corrects the foot drop component of cavovarus foot deformity in Charcot-Marie-Tooth disease. J Bone Joint Surg Am. 2014;96(6):456–62. doi: 10.2106/JBJS.L.01749. [DOI] [PubMed] [Google Scholar]
- 4.Giuffre JL, Bishop AT, Spinner RJ, et al. Partial tibial nerve transfer to the tibialis anterior motor branch to treat peroneal nerve injury after knee trauma. Clin Orthop Relat Res. 2012;470(3):779–90. doi: 10.1007/s11999-011-1924-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hastings MK, Mueller MJ, Sinacore DR, et al. Effects of a tendo-Achilles lengthening procedure on muscle function and gait characteristics in a patient with diabetes mellitus. J Orthop Sports Phys Ther. 2000;30(2):85–90. doi: 10.2519/jospt.2000.30.2.85. [DOI] [PubMed] [Google Scholar]
- 6.Hastings MK, Sinacore DR, Mercer-Bolton N, et al. Precision of foot alignment measures in Charcot arthropathy. Foot Ankle Int. 2011;32(9):867–72. doi: 10.3113/FAI.2011.0867. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3586199/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hastings MK, Sinacore DR, Woodburn J, et al. Kinetics and kinematics after the Bridle procedure for treatment of traumatic foot drop. Clin Biomech (Bristol, Avon) 2013;28(5):555–61. doi: 10.1016/j.clinbiomech.2013.04.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kinzey SJ, Armstrong CW. The reliability of the star-excursion test in assessing dynamic balance. J Orthop Sports Phys Ther. 1998;27(5):356–60. doi: 10.2519/jospt.1998.27.5.356. [DOI] [PubMed] [Google Scholar]
- 9.Kitaoka HB, Alexander IJ, Adelaar RS, et al. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994;15(7):349–53. doi: 10.1177/107110079401500701. [DOI] [PubMed] [Google Scholar]
- 10.Martin RL, Irrgang JJ, Burdett RG, et al. Evidence of validity for the Foot and Ankle Ability Measure (FAAM) Foot Ankle Int. 2005;26(11):968–83. doi: 10.1177/107110070502601113. [DOI] [PubMed] [Google Scholar]
- 11.Mayer L. The Physiological method of tendon transplantation in the treatment of paralytic drop-foot. J Bone Joint Surg Am. 1937;19(2):389–394. [Google Scholar]
- 12.McCall RE, Frederick HA, McCluskey GM, Riordan DC. The Bridle procedure: a new treatment for equinus and equinovarus deformities in children. J Pediatr Orthop. 1991;11(1):83–9. [PubMed] [Google Scholar]
- 13.Mizel MS, Temple HT, Scranton PE, Jr, et al. Role of the peroneal tendons in the production of the deformed foot with posterior tibial tendon deficiency. Foot Ankle Int. 1999;20(5):285–9. doi: 10.1177/107110079902000502. [DOI] [PubMed] [Google Scholar]
- 14.Mont MA, Dellon AL, Chen F, et al. The operative treatment of peroneal nerve palsy. J Bone Joint Surg Am. 1996;78(6):863–9. [PubMed] [Google Scholar]
- 15.Mueller MJ, Minor SD, Sahrmann SA, et al. Differences in the gait characteristics of patients with diabetes and peripheral neuropathy compared with age-matched controls. Phys Ther. 1994;74(4):299–308. doi: 10.1093/ptj/74.4.299. discussion 309–13. [DOI] [PubMed] [Google Scholar]
- 16.Ness ME, Long J, Marks R, Harris G. Foot and ankle kinematics in patients with posterior tibial tendon dysfunction. Gait Posture. 2008;27(2):331–9. doi: 10.1016/j.gaitpost.2007.04.014. [DOI] [PubMed] [Google Scholar]
- 17.Neville C, Flemister AS, Houck JR. Deep posterior compartment strength and foot kinematics in subjects with stage II posterior tibial tendon dysfunction. Foot Ankle Int. 2010;31(4):320–8. doi: 10.3113/FAI.2010.0320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Olmsted LC, Carcia CR, Hertel J, Shultz SJ. Efficacy of the Star Excursion Balance Tests in Detecting Reach Deficits in Subjects With Chronic Ankle Instability. J Athl Train. 2002;37(4):501–506. [PMC free article] [PubMed] [Google Scholar]
- 19.Prahinski JR, McHale KA, Temple HT, Jackson JP. Bridle transfer for paresis of the anterior and lateral compartment musculature. Foot Ankle Int. 1996;17(10):615–9. doi: 10.1177/107110079601701005. [DOI] [PubMed] [Google Scholar]
- 20.Rodriguez RP. The Bridle procedure in the treatment of paralysis of the foot. Foot Ankle. 1992;13(2):63–9. doi: 10.1177/107110079201300203. [DOI] [PubMed] [Google Scholar]
- 21.Silfverskiöld N. Reduction of the uncrossed two-joints muscles of the leg to one-joint muscles in spastic conditions. Acta Chir Scand. 1924;65:315–330. [Google Scholar]
- 22.Tome J, Nawoczenski DA, Flemister A, Houck J. Comparison of foot kinematics between subjects with posterior tibialis tendon dysfunction and healthy controls. J Orthop Sports Phys Ther. 2006;36(9):635–44. doi: 10.2519/jospt.2006.2293. [DOI] [PubMed] [Google Scholar]
- 23.Vertullo CJ, Nunley JA. Acquired flatfoot deformity following posterior tibial tendon transfer for peroneal nerve injury : a case report. J Bone Joint Surg Am. 2002;84-A(7):1214–7. doi: 10.2106/00004623-200207000-00020. [DOI] [PubMed] [Google Scholar]
- 24.Vigasio A, Marcoccio I, Patelli A, et al. New tendon transfer for correction of drop-foot in common peroneal nerve palsy. Clin Orthop Relat Res. 2008;466(6):1454–66. doi: 10.1007/s11999-008-0249-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Watkins MB, Jones JB, Ryder CT, Jr, Brown TH., Jr Transplantation of the posterior tibial tendon. J Bone Joint Surg Am. 1954;36-A(6):1181–9. [PubMed] [Google Scholar]
- 26.Wiesseman GJ. Tendon transfers for peripheral nerve injuries of the lower extremity. Orthop Clin North Am. 1981;12(2):459–67. [PubMed] [Google Scholar]
- 27.Yeap JS, Birch R, Singh D. Long-term results of tibialis posterior tendon transfer for drop-foot. Int Orthop. 2001;25(2):114–8. doi: 10.1007/s002640100229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Yeap JS, Singh D, Birch R. A method for evaluating the results of tendon transfers for foot drop. Clin Orthop Relat Res. 2001;(383):208–13. doi: 10.1097/00003086-200102000-00024. [DOI] [PubMed] [Google Scholar]