

Abstract
Objectives:
To provide age- and sex-specific reference data for mechanography-derived parameters of muscle function in Canadian children and youth using the single two-legged jump (S2LJ) with hands-on-waist.
Methods:
Our sample included 2017 observations from 715 participants (9-21 years; 338 girls). Participants performed three S2LJ with hands-on-waist on a force platform (Leonardo Mechanograph, Novotec). Outcomes were maximum peak power (Pmax), Pmax /mass, peak force/body weight (Fmax /BW), force efficiency, maximum jump height (Hmax), and velocity (Vmax). We used the LMS method to construct age- and sex-specific percentile curves and mixed effects models to examine sex and ethnic differences.
Results:
With the exception of Efficiency, mechanography outcomes were greater in girls (4-40%, p<0.05) than boys at age 9. Boys’ advantage in mechanography parameters emerged in adolescence (age 11-13 years; 3-65%, p<0.05) and persisted into young adulthood, except for Fmax/BW which was not greater in boys until age 17 (4-10%, p<0.05). Mechanography outcomes were 3-9% (p<0.05) greater in Asian compared with white participants.
Conclusions:
We provide the first reference data for the S2LJ using the hands-on-waist protocol in children, youth and young adults. These data support previous findings using freely moving arms and can be used when evaluating muscle function in pediatric studies.
Keywords: Jumping Mechanography, Children, Muscle Power, Muscle Force, Adolescents
Introduction
Muscle function is central to the body’s ability to carry out activities of daily living, perform exercise and regulate basic metabolism, including insulin control[1]. Further, changes in muscle function represent key indicators of physical development[2] and musculoskeletal health across the lifespan. Conversely, diminished muscle mass, strength or power may be a marker of increased frailty[3] or increased risk of chronic disease[1]. Importantly, skeletal muscle development is tightly coupled with bone accrual during childhood and adolescence, as muscle contractions create the largest voluntary loads on bone[4,5]. Thus, assessment of muscle function is central to understanding the important muscle-bone relationship in health and disease.
There are a wide range of methods that assess muscle function. These include hand-held dynamometry, isokinetic dynamometry and field test batteries[6]. However, many of these methods, including the most frequently used isometric muscle test (grip strength), do not adequately describe muscle force and power in movements common to activities of daily living[7,8]. Currently, dynamic muscle function is often assessed in children using jumping mechanography. Jumping mechanography assesses ground reaction forces related to the jump and provides outputs such as relative maximum forces, velocity, power and jump height. Specific to our study, a portable ground reaction force plate provides a valid and reliable quantitative measure of muscle force and power[9,10].
The single two-legged jump (S2LJ) coupled with mechanography is commonly used to assess muscle function in children and adolescents. It may also be regarded as a ‘screening test’ for anaerobic fitness[7]. As a vertical countermovement jump, the aim of the S2LJ is to achieve maximum jump height. Results are influenced by factors such as muscle power, coordination, balance and jumping technique[7]. The jump may be performed with freely moving arms or with hands-on-waist; the former leads to greater jump height due to increased lower extremity work output (e.g., increased torque in the hip joint during the latter half of the propulsion phase)[11] and greater variability in jump performance due to the positive influence of an upward arm swing[12]. The latter is less mechanically challenging, minimizing the influence of coordination on jump parameters in heterogeneous populations (i.e. mix of athletic and sedentary individuals)[13] and permits a better focus on muscle actions in the lower limbs[14]. Pediatric reference data are currently only available for the S2LJ with freely moving arms[7,15]. Therefore, we sought to create a Canadian reference data set for the S2LJ for the static arm (hands-on-waist) protocol.
Methods
Participants
Our study cohort was comprised of participants in the University of British Columbia’s Healthy Bones III study (n=397; 210 females, 187 males; ages 9-21 yrs) and the Centre for Hip Health and Mobility’s (www.hiphealth.ca) Fracture and Risk-taking Behaviour Study (n=319; 129 females, 190 males; ages 9-15 yrs). Together these data comprise our Pediatric Bone and Physical Activity Database. Both cohorts are described in detail elsewhere[16,17]. For the purpose of this analysis, data from the HBSIII cohort included a maximum of 4 annual measurements conducted between 2008 (first year of mechanography) and 2012. Data for the Fracture Study cohort included a maximum of 3 annual measurements conducted between 2010 and 2014. Across both cohorts the number of measurements was 3, on average (range: 1 to 4) and the average time between measurements was 1.0 (±0.2) years. Thus, our analysis included a total of 2017 observations across a maximum 6 years (Table 1).
Table 1.
Number of jumping mechanography observations by age and sex.
| Age (yr) | Total | Girls | Boys |
|---|---|---|---|
| 9 | 82 | 54 | 28 |
| 10 | 176 | 113 | 63 |
| 11 | 224 | 134 | 90 |
| 12 | 245 | 128 | 117 |
| 13 | 195 | 85 | 110 |
| 14 | 193 | 57 | 136 |
| 15 | 204 | 67 | 137 |
| 16 | 165 | 53 | 112 |
| 17 | 152 | 58 | 94 |
| 18 | 143 | 63 | 80 |
| 19 | 100 | 51 | 49 |
| 20 | 83 | 48 | 35 |
| 21 | 55 | 32 | 23 |
| TOTAL | 2017 | 943 | 1074 |
All participants were normally active and none were taking medications known to influence musculoskeletal health. Participants represented a variety of ethnicities, as per the ethnic diversity common to Metro Vancouver[18]. Based on parental report, 56% (n=401) of our cohort was white (both parents or 3 of 4 grandparents born in North America or Europe), 32% (n=226) were Asian (both parents or 3 of 4 grandparents born in Hong Kong, China, India, Philippines, Vietnam, Korea or Taiwan) and 12% (n=88) were of mixed or other ethnicities.
Parents or legal guardians and participants aged 18 years or older provided written informed consent and participants younger than 18 years of age provided written assent. The University of British Columbia Clinical Research Ethics Board approved all procedures (#H08-01846, #H15-01194).
Anthropometry
We measured standing height (stretch stature) to the nearest 0.1 cm with a wall-mounted digital stadiometer (Seca Model 242, Hanover, MD, USA), and body mass to the nearest 0.1kg with an electronic scale (Seca Model 840, Hanover, MD, USA). We used the mean of two measures for analysis. We calculated body mass index (BMI) as mass (kg) divided by height squared (m2).
Jumping mechanography
We used the Leonardo Mechanograph Ground Reaction Force Plate (GRFP; Novotec Medical GmbH, Germany) for mechanography; the protocol is described in detail elsewhere[9]. Briefly, the GRFP has two sections, which allows for simultaneous measurement of force (vertical component only) applied to right and left legs separately[10]. The sample rate is set to 800 Hz (800 measurements/second for each force sensor). We used the manufacturer’s software (Leonardo Mechanography v4.3) to detect, store and calculate mechanography outcomes. Leonardo software uses force and time data to calculate velocity of the movement (metres/second), power (Watts, W) and jump height (metres) using the approach as described by Cavagna[19].
All participants performed a single two-legged countermovement vertical jump on the GRFP with their hands held static at their waist and their feet hip width apart. The research assistant explained the jumping protocol to all participants in a standardized manner. Participants were asked to perform the countermovement jump after hearing the tone (from the computer). The research assistant instructed each participant to initiate a downwards movement and then immediately jump as high as possible using both legs. Participants were instructed to land with both feet on the platform (with each foot on the appropriate side of the middle line) and to remain still until after hearing the tone from the computer signaling the end of the trial. Each participant performed one practice jump and three trial jumps. We used the jump associated with maximum height for analysis.
A number of outcomes are provided by the manufacturer’s software; however, the main outcomes of interest for the S2LJ are the peak power during lift off phase (Pmax, kW) and Pmax relative to body mass (Pmax/mass, W/kg). We also report Fmax normalized to body weight (body mass*force of gravity or max acceleration/g; Fmax/BW), as this variable is used to calculate force efficiency Efficiency=100*(EFI[%]/(100*((Fmax/BW)/2,4g))). Finally, we report jump height (m), velocity (m/sec) and the percent differences in Pmax between right and left legs. We did not assess reproducibility of these measures in our laboratory. However, in a previous study of children aged 7-11 years for the S2LJ using freely moving arms, the coefficient of variation (%CV) ranged from 2.3% (Vmax) to 13.1% (Fmax/BW)[10]. Another study of 19-35 year old adults using the S2LJ with static arms reported that CV% ranged from 0.1% (Pmax) to 6.0% (Efficiency)[20].
Statistical analysis
We used Stata, version 13 (StataCorp, College Station, TX) to generate z-scores for anthropometric outcomes (using the zanthro command; comparison with CDC reference data[21]) and descriptive statistics, and to compare z-scores between our sample population and the reference cohort using one-sample t-tests. To address our primary objective, we used the lambda, mu, sigma (LMS) method using LMS ChartMaker Light (Version 2.5, The Institute of Child Health, London, UK) to construct LMS tables and reference centile plots showing the 3rd, 10th, 25th, 50th, 75th, 90th and 97th centiles in both girls and boys by age[22,23]. Briefly, this method uses normal approximation after a Box-Cox transformation to describe the distribution of the mechanography parameters at a given age. The LMS method estimates measurement centiles in terms of three age-specific cubic spline curves by non-linear regression: the L curve (Box-Cox power to remove skewness), M curve (median) and S curve (coefficient of variation after transformation). We assessed goodness of fit by visually inspecting the centile curves relative to the raw data and comparing deviance statistics for varying equivalent degrees of freedom in order to obtain optimal L, M and S values. Finally, we compared mechanography outcomes between girls and boys at each age by fitting mixed effects models that included a random intercept and random slopes, allowing each individual’s profile to vary around the mean. We included sex, ethnicity, and the interaction of sex and age as fixed effects in the model. In an additional model, we included the fixed effects of height using a person-mean-centered approach, such that the within-person (intra-individual) effect of height was represented by the deviation from the participant’s mean value across years (i.e. heightti –  ; where heightti is the bone parameter on measurement occasion t in the ith participant and
; where heightti is the bone parameter on measurement occasion t in the ith participant and  is that participant’s mean height across years), while the between-person (inter-individual) effect was represented by the participant’s mean value across years, centered at a meaningful value for interpretation (i.e.
is that participant’s mean height across years), while the between-person (inter-individual) effect was represented by the participant’s mean value across years, centered at a meaningful value for interpretation (i.e.  – 160). We calculated adjusted means and estimated sex and ethnic differences in bone parameters at each age using the margins command in Stata. We used a Bonferroni adjustment to account for multiple sex comparisons for each mechanography parameter and considered a p-value <0.0038 significant (initial p-value of 0.05 divided by 13 age-group comparisons).
– 160). We calculated adjusted means and estimated sex and ethnic differences in bone parameters at each age using the margins command in Stata. We used a Bonferroni adjustment to account for multiple sex comparisons for each mechanography parameter and considered a p-value <0.0038 significant (initial p-value of 0.05 divided by 13 age-group comparisons).
Results
We provide descriptive characteristics for participants’ first jumping mechanography measurement in Table 2. Z-scores for height, mass and BMI for our cohort were positive and significantly different from zero.
Table 2.
Participant characteristics at first mechanography measurement. Values presented as mean ± standard deviation unless otherwise indicated.
| Girls (n=338) | Boys (n=377) | Total (n=715) | |
|---|---|---|---|
| Age (yr) | 13.3±3.3 | 13.9±2.7 | 13.6±3.0 |
| Height (cm) | 152.7±11.9 | 162.5±14.3 | 157.9±14.1 |
| Height (Z-score) | 0.2±1.0* | 0.3±1.0* | 0.3±1.0* |
| Weight (kg) | 47.0±13.9 | 54.9±16.2 | 51.2±15.6 |
| Weight (Z-score) | 0.2±1.0* | 0.4±1.0* | 0.3±1.0* |
| BMI (kg/m2) | 19.7±3.7 | 20.4±3.8 | 20.1±3.8 |
| BMI (Z-score) | 0.1±1.0* | 0.2±1.1* | 0.2±1.0* |
| Ethnicity (# Asian/white/Other) | 109 / 189 / 40 | 117 / 212 / 48 | 226 / 401 / 88 |
Z-scores were calculated using the CDC Growth Charts for the United States[21].
Statistically significant differences between the study group and the reference data are indicated as p<0.05.
We present percentile distributions and L, M and S parameters in [Tables 3-8] and age- and sex-specific summary statistics for mechanography outcomes in Table 9. Individual z scores for a given measurement (X) can be calculated according to the following formula:
Table 3.
Age- and sex-specific L, M and S parameters and percentile distribution for maximum power (Pmax) generated during a single two-legged jump with hands-on-waist.
| Pmax (kW) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Girls | Boys | |||||||||||||||
| Age (yr) | S | 3rd | 10th | 25th | 50th (M) | 75th | 90th | 97th | S | 3rd | 10th | 25th | 50th (M) | 75th | 90th | 97th |
| 9 | 0.18 | 0.75 | 0.84 | 0.94 | 1.07 | 1.20 | 1.34 | 1.48 | 0.15 | 0.88 | 0.96 | 1.06 | 1.18 | 1.31 | 1.43 | 1.56 |
| 10 | 0.20 | 0.82 | 0.93 | 1.05 | 1.20 | 1.37 | 1.54 | 1.72 | 0.16 | 0.95 | 1.05 | 1.17 | 1.31 | 1.46 | 1.61 | 1.77 |
| 11 | 0.21 | 0.93 | 1.06 | 1.20 | 1.39 | 1.60 | 1.81 | 2.03 | 0.18 | 1.04 | 1.16 | 1.30 | 1.47 | 1.66 | 1.84 | 2.04 |
| 12 | 0.21 | 1.07 | 1.23 | 1.40 | 1.63 | 1.88 | 2.13 | 2.40 | 0.20 | 1.14 | 1.29 | 1.46 | 1.68 | 1.92 | 2.16 | 2.41 |
| 13 | 0.21 | 1.23 | 1.41 | 1.60 | 1.85 | 2.13 | 2.40 | 2.71 | 0.22 | 1.26 | 1.46 | 1.68 | 1.96 | 2.28 | 2.60 | 2.95 |
| 14 | 0.20 | 1.37 | 1.56 | 1.76 | 2.01 | 2.30 | 2.58 | 2.88 | 0.24 | 1.45 | 1.70 | 1.98 | 2.33 | 2.73 | 3.14 | 3.59 |
| 15 | 0.19 | 1.47 | 1.66 | 1.87 | 2.12 | 2.40 | 2.68 | 2.98 | 0.23 | 1.75 | 2.02 | 2.33 | 2.71 | 3.15 | 3.59 | 4.08 |
| 16 | 0.18 | 1.53 | 1.71 | 1.92 | 2.17 | 2.45 | 2.73 | 3.03 | 0.20 | 2.07 | 2.35 | 2.66 | 3.04 | 3.47 | 3.89 | 4.36 |
| 17 | 0.18 | 1.55 | 1.74 | 1.94 | 2.19 | 2.47 | 2.75 | 3.05 | 0.19 | 2.28 | 2.57 | 2.89 | 3.29 | 3.73 | 4.16 | 4.63 |
| 18 | 0.18 | 1.56 | 1.75 | 1.95 | 2.20 | 2.48 | 2.76 | 3.05 | 0.19 | 2.37 | 2.68 | 3.02 | 3.45 | 3.92 | 4.39 | 4.90 |
| 19 | 0.18 | 1.58 | 1.76 | 1.97 | 2.22 | 2.50 | 2.77 | 3.07 | 0.20 | 2.40 | 2.72 | 3.09 | 3.54 | 4.05 | 4.55 | 5.10 |
| 20 | 0.17 | 1.60 | 1.79 | 1.99 | 2.24 | 2.52 | 2.79 | 3.08 | 0.20 | 2.41 | 2.74 | 3.12 | 3.59 | 4.11 | 4.64 | 5.21 |
| 21 | 0.17 | 1.63 | 1.81 | 2.02 | 2.27 | 2.54 | 2.81 | 3.10 | 0.21 | 2.41 | 2.75 | 3.14 | 3.61 | 4.15 | 4.68 | 5.27 |
The L parameter was 0.16 for girls and 0.18 for boys across all ages.
Table 4.
Age- and sex-specific L, M and S parameters and percentile distribution for maximum power relative to body mass (Pmax/mass) during a single two-legged jump with hands-on-waist.
| Pmax/mass (W/kg) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Girls | Boys | |||||||||||||||
| Age (yr) | S | 3rd | 10th | 25th | 50th (M) | 75th | 90th | 97th | S | 3rd | 10th | 25th | 50th (M) | 75th | 90th | 97th |
| 9 | 0.13 | 25.7 | 28.1 | 30.5 | 33.4 | 36.4 | 39.1 | 41.9 | 0.17 | 22.9 | 25.7 | 28.7 | 32.3 | 36.1 | 39.9 | 43.8 |
| 10 | 0.14 | 26.2 | 28.8 | 31.5 | 34.6 | 37.9 | 40.9 | 44.0 | 0.17 | 24.0 | 26.8 | 29.9 | 33.5 | 37.4 | 41.2 | 45.1 |
| 11 | 0.14 | 26.7 | 29.5 | 32.5 | 35.9 | 39.4 | 42.7 | 46.0 | 0.16 | 25.4 | 28.2 | 31.3 | 35.0 | 38.9 | 42.7 | 46.7 |
| 12 | 0.14 | 27.5 | 30.4 | 33.4 | 36.9 | 40.6 | 44.0 | 47.5 | 0.16 | 27.0 | 29.9 | 33.1 | 36.9 | 40.9 | 44.7 | 48.8 |
| 13 | 0.14 | 28.7 | 31.5 | 34.4 | 37.8 | 41.4 | 44.7 | 48.0 | 0.15 | 29.1 | 32.1 | 35.4 | 39.3 | 43.5 | 47.4 | 51.6 |
| 14 | 0.12 | 29.9 | 32.6 | 35.3 | 38.5 | 41.8 | 44.9 | 48.0 | 0.15 | 31.6 | 34.7 | 38.2 | 42.2 | 46.5 | 50.7 | 55.0 |
| 15 | 0.12 | 30.8 | 33.3 | 35.9 | 38.9 | 42.1 | 44.9 | 47.9 | 0.14 | 34.0 | 37.3 | 40.9 | 45.1 | 49.5 | 53.8 | 58.2 |
| 16 | 0.11 | 31.1 | 33.6 | 36.2 | 39.2 | 42.2 | 45.1 | 47.9 | 0.14 | 36.1 | 39.5 | 43.2 | 47.5 | 52.1 | 56.5 | 61.0 |
| 17 | 0.12 | 30.9 | 33.4 | 36.1 | 39.1 | 42.2 | 45.2 | 48.1 | 0.14 | 37.8 | 41.3 | 45.0 | 49.5 | 54.2 | 58.7 | 63.3 |
| 18 | 0.12 | 30.4 | 33.0 | 35.7 | 38.8 | 42.1 | 45.0 | 48.1 | 0.14 | 38.7 | 42.3 | 46.2 | 50.8 | 55.6 | 60.2 | 64.9 |
| 19 | 0.12 | 30.0 | 32.6 | 35.3 | 38.4 | 41.6 | 44.6 | 47.6 | 0.14 | 38.9 | 42.6 | 46.5 | 51.2 | 56.1 | 60.8 | 65.7 |
| 20 | 0.12 | 29.7 | 32.2 | 34.9 | 37.9 | 41.0 | 44.0 | 46.9 | 0.14 | 38.5 | 42.2 | 46.2 | 50.9 | 55.9 | 60.6 | 65.6 |
| 21 | 0.12 | 29.4 | 31.9 | 34.4 | 37.4 | 40.4 | 43.2 | 46.1 | 0.14 | 37.7 | 41.5 | 45.5 | 50.2 | 55.3 | 60.1 | 65.1 |
The L parameter was 0.59 for girls and 0.36 for boys across all ages.
Table 5.
Age- and sex-specific L, M and S parameters and percentile distribution for maximum force relative to body weight (Fmax/BW) generated during a single two-legged jump with hands-on-waist.
| Fmax/BW | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Girls | Boys | ||||||||||||||||
| Age (yr) | L | S | 3rd | 10th | 25th | 50th (M) | 75th | 90th | 97th | S | 3rd | 10th | 25th | 50th (M) | 75th | 90th | 97th |
| 9 | -0.75 | 0.17 | 1.82 | 1.98 | 2.17 | 2.42 | 2.73 | 3.07 | 3.48 | 0.15 | 1.78 | 1.88 | 2.01 | 2.20 | 2.47 | 2.84 | 3.48 |
| 10 | -0.98 | 0.16 | 1.83 | 1.98 | 2.16 | 2.39 | 2.69 | 3.02 | 3.44 | 0.14 | 1.79 | 1.90 | 2.02 | 2.21 | 2.47 | 2.81 | 3.39 |
| 11 | -1.21 | 0.16 | 1.84 | 1.98 | 2.14 | 2.36 | 2.64 | 2.97 | 3.39 | 0.14 | 1.81 | 1.91 | 2.04 | 2.21 | 2.46 | 2.78 | 3.29 |
| 12 | -1.45 | 0.15 | 1.85 | 1.97 | 2.13 | 2.33 | 2.60 | 2.92 | 3.34 | 0.13 | 1.83 | 1.93 | 2.05 | 2.22 | 2.46 | 2.75 | 3.21 |
| 13 | -1.69 | 0.14 | 1.85 | 1.97 | 2.11 | 2.31 | 2.56 | 2.86 | 3.28 | 0.12 | 1.86 | 1.96 | 2.08 | 2.24 | 2.46 | 2.73 | 3.13 |
| 14 | -1.92 | 0.13 | 1.85 | 1.96 | 2.09 | 2.28 | 2.52 | 2.81 | 3.22 | 0.12 | 1.89 | 1.99 | 2.10 | 2.26 | 2.46 | 2.72 | 3.07 |
| 15 | -2.15 | 0.13 | 1.85 | 1.95 | 2.08 | 2.25 | 2.47 | 2.75 | 3.16 | 0.11 | 1.92 | 2.02 | 2.13 | 2.28 | 2.47 | 2.70 | 3.02 |
| 16 | -2.39 | 0.12 | 1.85 | 1.94 | 2.06 | 2.22 | 2.43 | 2.69 | 3.09 | 0.10 | 1.94 | 2.03 | 2.14 | 2.29 | 2.47 | 2.69 | 2.98 |
| 17 | -2.62 | 0.11 | 1.84 | 1.93 | 2.04 | 2.19 | 2.39 | 2.63 | 3.01 | 0.10 | 1.96 | 2.05 | 2.15 | 2.29 | 2.47 | 2.68 | 2.95 |
| 18 | -2.86 | 0.11 | 1.84 | 1.92 | 2.02 | 2.16 | 2.34 | 2.57 | 2.93 | 0.10 | 1.96 | 2.05 | 2.15 | 2.29 | 2.47 | 2.67 | 2.94 |
| 19 | -3.09 | 0.10 | 1.83 | 1.91 | 2.00 | 2.13 | 2.30 | 2.51 | 2.84 | 0.10 | 1.96 | 2.05 | 2.16 | 2.29 | 2.47 | 2.67 | 2.93 |
| 20 | -3.33 | 0.09 | 1.83 | 1.90 | 1.98 | 2.10 | 2.26 | 2.45 | 2.75 | 0.10 | 1.97 | 2.06 | 2.16 | 2.30 | 2.47 | 2.66 | 2.92 |
| 21 | -3.56 | 0.09 | 1.82 | 1.88 | 1.96 | 2.07 | 2.21 | 2.39 | 2.66 | 0.09 | 1.98 | 2.07 | 2.17 | 2.30 | 2.46 | 2.65 | 2.89 |
The L parameter was -2.33 for boys across all ages.
Table 6.
Age- and sex-specific L, M and S parameters and percentile distribution for maximum velocity (Vmax) generated during a single two-legged jump with hands-on-waist.
| Vmax (m/s) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Girls | Boys | ||||||||||||||||
| Age (yr) | S | 3rd | 10th | 25th | 50th (M) | 75th | 90th | 97th | L | S | 3rd | 10th | 25th | 50th (M) | 75th | 90th | 97th |
| 9 | 0.08 | 1.69 | 1.78 | 1.88 | 1.98 | 2.08 | 2.18 | 2.27 | -0.29 | 0.11 | 1.58 | 1.68 | 1.79 | 1.92 | 2.06 | 2.21 | 2.36 |
| 10 | 0.08 | 1.74 | 1.83 | 1.93 | 2.03 | 2.14 | 2.24 | 2.33 | 0.10 | 0.10 | 1.64 | 1.75 | 1.86 | 2.00 | 2.14 | 2.28 | 2.42 |
| 11 | 0.08 | 1.78 | 1.88 | 1.98 | 2.09 | 2.20 | 2.29 | 2.39 | 0.52 | 0.10 | 1.71 | 1.82 | 1.94 | 2.08 | 2.22 | 2.36 | 2.49 |
| 12 | 0.08 | 1.82 | 1.92 | 2.02 | 2.14 | 2.25 | 2.35 | 2.45 | 0.93 | 0.10 | 1.78 | 1.90 | 2.03 | 2.17 | 2.32 | 2.45 | 2.57 |
| 13 | 0.08 | 1.86 | 1.96 | 2.06 | 2.17 | 2.29 | 2.39 | 2.49 | 1.31 | 0.09 | 1.87 | 2.00 | 2.13 | 2.28 | 2.42 | 2.55 | 2.67 |
| 14 | 0.08 | 1.88 | 1.98 | 2.09 | 2.20 | 2.32 | 2.42 | 2.52 | 1.64 | 0.09 | 1.97 | 2.11 | 2.25 | 2.39 | 2.53 | 2.66 | 2.77 |
| 15 | 0.08 | 1.90 | 2.00 | 2.11 | 2.22 | 2.34 | 2.44 | 2.55 | 1.88 | 0.08 | 2.07 | 2.22 | 2.36 | 2.50 | 2.64 | 2.76 | 2.87 |
| 16 | 0.08 | 1.91 | 2.01 | 2.12 | 2.24 | 2.35 | 2.46 | 2.56 | 1.95 | 0.08 | 2.17 | 2.32 | 2.45 | 2.60 | 2.73 | 2.85 | 2.96 |
| 17 | 0.08 | 1.91 | 2.02 | 2.12 | 2.24 | 2.36 | 2.46 | 2.57 | 1.87 | 0.08 | 2.25 | 2.39 | 2.52 | 2.67 | 2.80 | 2.92 | 3.03 |
| 18 | 0.08 | 1.91 | 2.02 | 2.12 | 2.24 | 2.36 | 2.46 | 2.57 | 1.67 | 0.08 | 2.29 | 2.43 | 2.56 | 2.71 | 2.85 | 2.97 | 3.09 |
| 19 | 0.08 | 1.91 | 2.01 | 2.12 | 2.23 | 2.35 | 2.46 | 2.56 | 1.40 | 0.08 | 2.29 | 2.43 | 2.57 | 2.72 | 2.87 | 3.00 | 3.13 |
| 20 | 0.08 | 1.90 | 2.00 | 2.11 | 2.22 | 2.34 | 2.44 | 2.55 | 1.07 | 0.09 | 2.26 | 2.41 | 2.55 | 2.72 | 2.88 | 3.02 | 3.16 |
| 21 | 0.08 | 1.89 | 1.99 | 2.09 | 2.21 | 2.33 | 2.43 | 2.53 | 0.70 | 0.09 | 2.23 | 2.38 | 2.53 | 2.70 | 2.87 | 3.03 | 3.19 |
The L parameter was 1.0 for girls across all ages.
Table 7.
Age- and sex-specific L, M and S parameters and percentile distribution for maximum jump height (Hmax) generated during a single two-legged jump with hands-on-waist.
| Hmax (m) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Girls | Boys | ||||||||||||||||
| Age (yr) | S | 3rd | 10th | 25th | 50th (M) | 75th | 90th | 97th | L | S | 3rd | 10th | 25th | 50th (M) | 75th | 90th | 97th |
| 9 | 0.13 | 0.20 | 0.22 | 0.24 | 0.26 | 0.29 | 0.31 | 0.33 | -0.70 | 0.17 | 0.19 | 0.21 | 0.23 | 0.25 | 0.28 | 0.32 | 0.36 |
| 10 | 0.13 | 0.21 | 0.23 | 0.26 | 0.28 | 0.30 | 0.33 | 0.35 | -0.38 | 0.17 | 0.20 | 0.22 | 0.24 | 0.27 | 0.30 | 0.34 | 0.38 |
| 11 | 0.13 | 0.22 | 0.25 | 0.27 | 0.30 | 0.32 | 0.34 | 0.37 | -0.04 | 0.16 | 0.22 | 0.24 | 0.26 | 0.29 | 0.33 | 0.36 | 0.40 |
| 12 | 0.13 | 0.23 | 0.26 | 0.28 | 0.31 | 0.33 | 0.36 | 0.38 | 0.29 | 0.16 | 0.23 | 0.26 | 0.29 | 0.32 | 0.35 | 0.39 | 0.42 |
| 13 | 0.13 | 0.24 | 0.27 | 0.29 | 0.32 | 0.35 | 0.37 | 0.39 | 0.60 | 0.16 | 0.25 | 0.28 | 0.31 | 0.35 | 0.38 | 0.42 | 0.45 |
| 14 | 0.13 | 0.25 | 0.27 | 0.30 | 0.32 | 0.35 | 0.38 | 0.40 | 0.85 | 0.15 | 0.27 | 0.30 | 0.34 | 0.37 | 0.41 | 0.45 | 0.48 |
| 15 | 0.13 | 0.25 | 0.27 | 0.30 | 0.33 | 0.36 | 0.38 | 0.41 | 1.02 | 0.14 | 0.29 | 0.33 | 0.36 | 0.40 | 0.44 | 0.48 | 0.51 |
| 16 | 0.13 | 0.25 | 0.28 | 0.30 | 0.33 | 0.36 | 0.38 | 0.41 | 1.06 | 0.14 | 0.32 | 0.35 | 0.39 | 0.43 | 0.47 | 0.50 | 0.53 |
| 17 | 0.13 | 0.25 | 0.28 | 0.30 | 0.33 | 0.36 | 0.39 | 0.41 | 1.00 | 0.13 | 0.33 | 0.37 | 0.40 | 0.44 | 0.48 | 0.52 | 0.56 |
| 18 | 0.13 | 0.25 | 0.28 | 0.30 | 0.33 | 0.36 | 0.39 | 0.41 | 0.86 | 0.14 | 0.34 | 0.38 | 0.41 | 0.46 | 0.50 | 0.54 | 0.58 |
| 19 | 0.13 | 0.25 | 0.28 | 0.30 | 0.33 | 0.36 | 0.39 | 0.41 | 0.68 | 0.15 | 0.34 | 0.38 | 0.42 | 0.46 | 0.51 | 0.55 | 0.59 |
| 20 | 0.13 | 0.25 | 0.28 | 0.30 | 0.33 | 0.36 | 0.39 | 0.41 | 0.48 | 0.16 | 0.33 | 0.37 | 0.41 | 0.46 | 0.51 | 0.56 | 0.61 |
| 21 | 0.13 | 0.25 | 0.28 | 0.30 | 0.33 | 0.36 | 0.39 | 0.41 | 0.27 | 0.18 | 0.32 | 0.36 | 0.40 | 0.46 | 0.51 | 0.57 | 0.63 |
The L parameter was 1.0 for girls across all ages.
Table 8.
Age- and sex-specific L, M and S parameters and percentile distribution for force efficiency during a single two-legged jump with hands-on-waist.
| Efficiency (%) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Girls | Boys | ||||||||||||||||
| Age (yr) | S | 3rd | 10th | 25th | 50th (M) | 75th | 90th | 97th | L | S | 3rd | 10th | 25th | 50th (M) | 75th | 90th | 97th |
| 9 | 0.13 | 74.6 | 84.2 | 93.3 | 102.7 | 111.6 | 119.2 | 126.3 | 0.32 | 0.14 | 79.9 | 87.5 | 95.6 | 105.3 | 115.5 | 125.3 | 135.5 |
| 10 | 0.13 | 74.7 | 83.8 | 92.5 | 101.4 | 109.9 | 117.2 | 124.0 | 0.58 | 0.14 | 79.3 | 87.0 | 95.1 | 104.5 | 114.2 | 123.2 | 132.4 |
| 11 | 0.12 | 74.8 | 83.4 | 91.6 | 100.1 | 108.2 | 115.1 | 121.7 | 0.88 | 0.13 | 78.7 | 86.6 | 94.6 | 103.7 | 112.8 | 121.1 | 129.3 |
| 12 | 0.12 | 74.6 | 82.7 | 90.5 | 98.5 | 106.2 | 112.8 | 119.0 | 1.18 | 0.13 | 78.3 | 86.3 | 94.3 | 103.1 | 111.7 | 119.4 | 126.9 |
| 13 | 0.11 | 74.3 | 82.0 | 89.3 | 96.9 | 104.2 | 110.4 | 116.4 | 1.47 | 0.12 | 78.4 | 86.6 | 94.6 | 103.2 | 111.4 | 118.5 | 125.4 |
| 14 | 0.11 | 74.3 | 81.6 | 88.6 | 95.9 | 102.9 | 109.0 | 114.7 | 1.74 | 0.12 | 79.0 | 87.5 | 95.5 | 103.8 | 111.7 | 118.4 | 124.8 |
| 15 | 0.11 | 74.4 | 81.6 | 88.4 | 95.6 | 102.4 | 108.3 | 113.9 | 1.96 | 0.11 | 80.1 | 88.7 | 96.6 | 104.7 | 112.3 | 118.7 | 124.7 |
| 16 | 0.11 | 74.6 | 81.6 | 88.3 | 95.4 | 102.2 | 108.0 | 113.6 | 2.08 | 0.11 | 81.1 | 89.5 | 97.3 | 105.1 | 112.4 | 118.6 | 124.3 |
| 17 | 0.11 | 74.6 | 81.6 | 88.3 | 95.4 | 102.2 | 108.0 | 113.5 | 2.09 | 0.10 | 81.3 | 89.4 | 96.8 | 104.4 | 111.4 | 117.4 | 122.9 |
| 18 | 0.11 | 74.6 | 81.6 | 88.3 | 95.4 | 102.1 | 107.9 | 113.5 | 2.00 | 0.10 | 80.6 | 88.1 | 95.2 | 102.5 | 109.2 | 115.0 | 120.4 |
| 19 | 0.11 | 74.7 | 81.6 | 88.3 | 95.4 | 102.0 | 107.8 | 113.3 | 1.81 | 0.10 | 79.1 | 86.1 | 92.8 | 99.8 | 106.4 | 112.0 | 117.4 |
| 20 | 0.11 | 74.7 | 81.7 | 88.3 | 95.3 | 102.0 | 107.7 | 113.2 | 1.54 | 0.10 | 77.5 | 84.0 | 90.2 | 96.9 | 103.4 | 109.0 | 114.4 |
| 21 | 0.11 | 74.8 | 81.7 | 88.3 | 95.3 | 101.9 | 107.6 | 113.1 | 1.22 | 0.10 | 75.9 | 81.9 | 87.7 | 94.2 | 100.5 | 106.2 | 111.7 |
The L parameter was 1.7 for girls across all ages.
Table 9.
Summary statistics for mechanography outcomes in girls and boys during a single two-legged jump with hands-on-waist. Values are presented as mean (standard error).
| Pmax (kW) | Pmax/mass (W/kg) | Fmax/BW | Vmax (m/s) | Hmax (m) | Efficiency (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (yr) | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | Boys |
| 9 | 0.92 (0.03)* | 0.74 (0.04) | 34.0 (0.5)* | 30.9 (0.6) | 2.52 (0.03)* | 2.36 (0.03) | 1.98 (0.02)* | 1.87 (0.02) | 0.266 (0.005)* | 0.238 (0.006) | 104.4 (1.3) | 104.7 (1.6) |
| 10 | 1.20 (0.03) | 1.13 (0.03) | 35.3 (0.4) | 33.8 (0.5) | 2.49 (0.03)* | 2.36 (0.03) | 2.04 (0.01) | 2.00 (0.02) | 0.281 (0.003) | 0.270 (0.004) | 101.8 (1.0) | 104.8 (1.2) |
| 11 | 1.44 (0.02) | 1.50 (0.03) | 36.3 (0.3) | 36.4 (0.4) | 2.45 (0.02)* | 2.35 (0.02) | 2.09 (0.01) | 2.11 (0.01) | 0.294 (0.003) | 0.300 (0.003) | 99.5 (0.8) | 104.7 (0.9)** |
| 12 | 1.44 (0.02) | 1.84 (0.02)** | 36.3 (0.3) | 38.9 (0.3)** | 2.45 (0.02) | 2.35 (0.02) | 2.09 (0.01) | 2.21 (0.01)** | 0.294 (0.003) | 0.328 (0.003)** | 99.5 (0.8) | 104.5 (0.7)** |
| 13 | 1.85 (0.02) | 2.16 (0.02)** | 37.8 (0.3) | 41.1 (0.3)** | 2.38 (0.02) | 2.34 (0.02) | 2.16 (0.01) | 2.31 (0.01)** | 0.315 (0.003) | 0.354 (0.002)** | 96.1 (0.7) | 104.2 (0.6)** |
| 14 | 2.01 (0.03) | 2.46 (0.02)** | 38.3 (0.3) | 43.2 (0.3)** | 2.34 (0.02) | 2.34 (0.02) | 2.19 (0.01) | 2.40 (0.01)** | 0.323 (0.003) | 0.377 (0.003)** | 94.9 (0.7) | 103.7 (0.6)** |
| 15 | 2.14 (0.03) | 2.72 (0.03)** | 38.7 (0.3) | 45.0 (0.3)** | 2.31 (0.01) | 2.33 (0.01) | 2.22 (0.01) | 2.48 (0.01)** | 0.330 (0.003) | 0.399 (0.003)** | 94.2 (0.7) | 103.1 (0.6)** |
| 16 | 2.24 (0.03) | 2.97 (0.03)** | 38.8 (0.4) | 46.6 (0.3)** | 2.27 (0.02) | 2.33 (0.01) | 2.23 (0.01) | 2.55 (0.01)** | 0.334 (0.003) | 0.418 (0.003)** | 93.8 (0.7) | 102.3 (0.6)** |
| 17 | 2.31 (0.04) | 3.19 (0.03)** | 38.8 (0.4) | 48.0 (0.3)** | 2.23 (0.02) | 2.32 (0.01)** | 2.24 (0.01) | 2.61 (0.01)** | 0.338 (0.004) | 0.435 (0.003)** | 93.8 (0.7) | 101.4 (0.6)** |
| 18 | 2.36 (0.04) | 3.38 (0.04)** | 38.6 (0.4) | 49.2 (0.4)** | 2.20 (0.02) | 2.32 (0.02)** | 2.25 (0.01) | 2.66 (0.01)** | 0.339 (0.004) | 0.450 (0.004)** | 94.1 (0.8) | 100.4 (0.7)** |
| 19 | 2.37 (0.05) | 3.55 (0.04)** | 38.3 (0.5) | 50.2 (0.5)** | 2.16 (0.02) | 2.31 (0.02)** | 2.25 (0.02) | 2.71 (0.02)** | 0.339 (0.005) | 0.463 (0.004)** | 94.8 (0.8) | 99.2 (0.8)** |
| 20 | 2.35 (0.06) | 3.69 (0.05)** | 37.7 (0.6) | 51.0 (0.6)** | 2.13 (0.02) | 2.31 (0.02)** | 2.24 (0.02) | 2.74 (0.02)** | 0.337 (0.006) | 0.473 (0.005)** | 95.9 (1.0) | 97.9 (1.0) |
| 21 | 2.31 (0.07) | 3.81 (0.06)** | 37.0 (0.7) | 51.6 (0.7)** | 2.09 (0.03) | 2.30 (0.03)** | 2.22 (0.02) | 2.77 (0.02)** | 0.333 (0.007) | 0.482 (0.007)** | 97.4 (1.3) | 96.4 (1.3) |
Girls >Boys, p<0.05 with Bonferroni adjustment;
Boys >Girls, p<0.05 with Bonferroni adjustment.
Scatter plots of individual values with lowess curves are provided in Figures 1 and 2 and age- and sex-specific reference curves for Pmax, Pmax/mass, Fmax/BW, Efficiency, Hmax and Vmax in Figures 3 and 4.
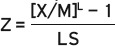
Figure 1.
Individual values and curves for the mean and 95% confidence interval for girls (on the left) and boys (on the right) by age for A) maximum peak power (Pmax), B) peak power relative to body mass (Pmax/mass), C) peak force relative to body weight (Fmax/BW), and D) Efficiency during a single two-legged jump with hands-on-waist.
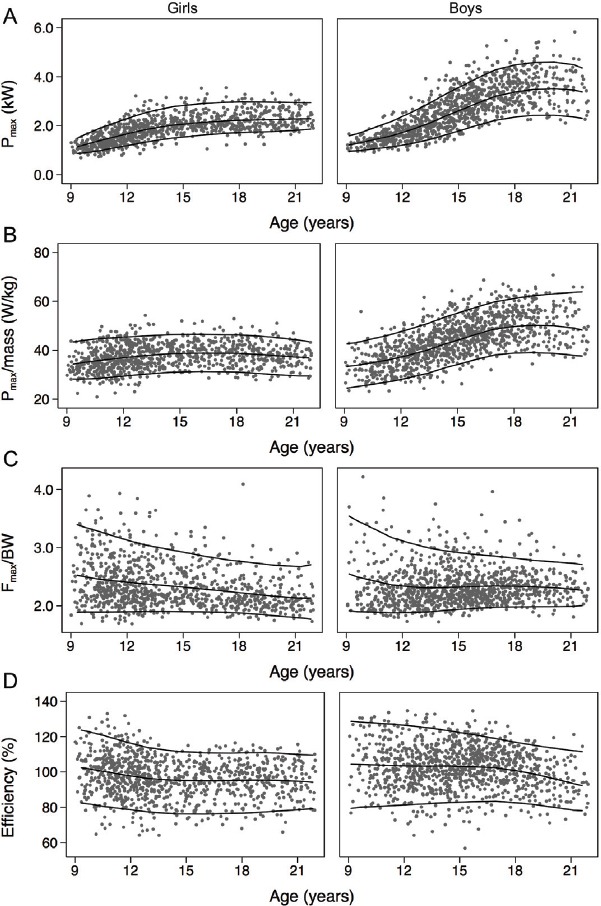
Figure 2.
Individual values and curves for the mean and 95% confidence interval for girls (on the left) and boys (on the right) by age for A) maximum velocity (Vmax) and B) maximum jump height (Hmax) during a single two-legged jump with hands-on-waist.
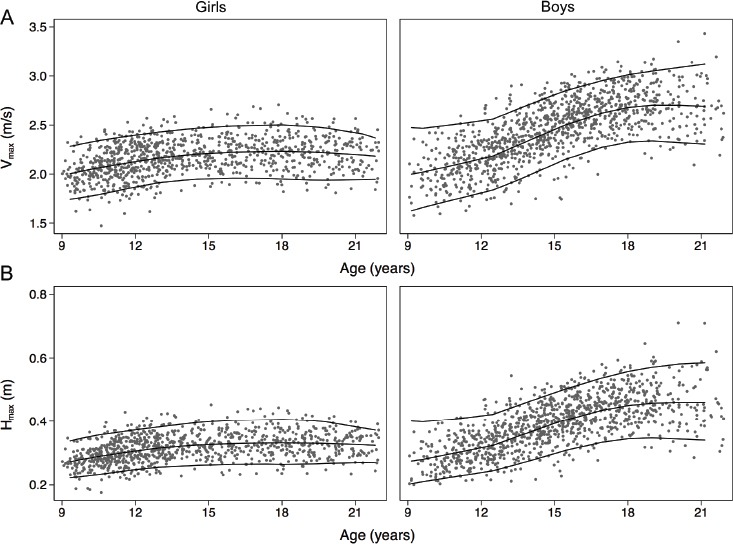
Figure 3.
Smoothed percentile graphs for girls (on the left) and boys (on the right) by age for A) maximum peak power (Pmax), B) peak power relative to body mass (Pmax/mass), C) peak force relative to body weight (Fmax/BW), and D) Efficiency during a single two-legged jump with hands-on-waist.
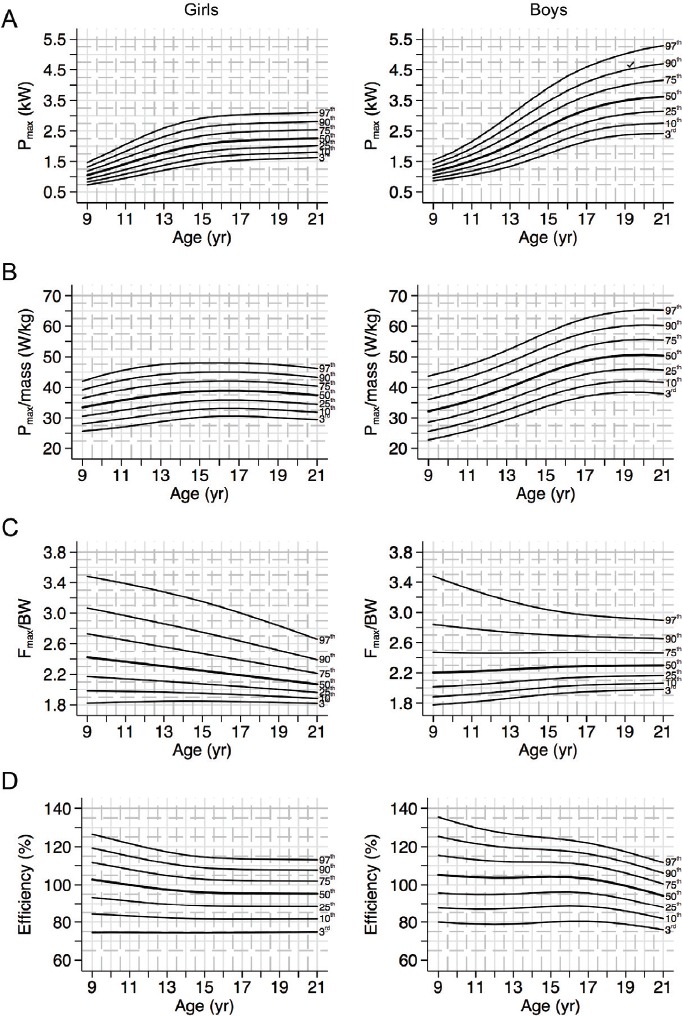
Figure 4.
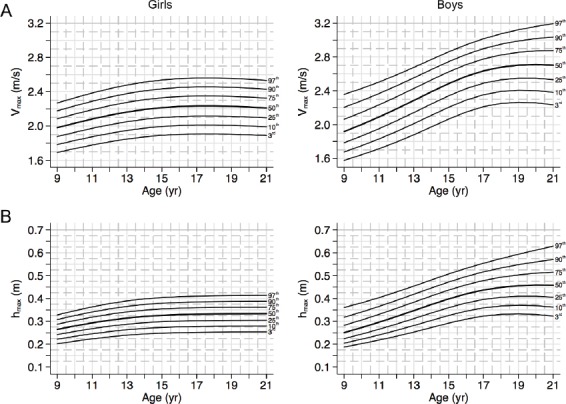
Smoothed percentile graphs for girls (on the left) and boys (on the right) by age for A) maximum velocity (Vmax) and B) maximum jump height (Hmax) during a single two-legged jump with hands-on-waist.
Age-related trends in mechanography outcomes in girls and boys
In girls, the curve for Pmax indicated an increase with age (of approximately 158%) until age 19, followed by a plateau until age 21. In boys, Pmax demonstrated a steeper increase with age during adolescence (~380% increase from age 9 and 19) and continued to increase until age 21 (Figures 1a & 3a). In girls and boys, the difference in Pmax Fmax between the right and left legs was approximately 9%, and remained constant with age (data not shown). In girls, the trajectory for Pmax/mass was similar to that of Pmax (14% increase from age 9 to 17), although Pmax/mass declined slightly after age 17 (5% decrease from age 17 to 21) (Figures 1b & 3b). In contrast, boys demonstrated a steep increase in Pmax/mass from age 9 and 17 (55%), and smaller gains thereafter.
In girls, Fmax/BW decreased with age (17% decrease from age 9 to 21). In boys this parameter remained fairly constant with age (3% decrease from age 9 to 21; Figures 1c & 3c). In girls, Efficiency gradually decreased until approximately age 16 (10% decrease from age 9 to 16) and plateaued thereafter. In boys, Efficiency remained relatively stable through adolescence (2% decrease from age 9 to 16) with greater decreases thereafter (Figures 1d & 3d).
In girls, Vmax increased until approximately age 18 (14% increase from age 9 to 18) and declined slightly thereafter. In boys, Vmax increased steeply during adolescence (42% increase from age 9 and 18) and smaller gains thereafter (Figures 2a & 4a). In girls, Hmax showed a similar trend to Vmax, but with greater age-related gains during adolescence (27% from age 9 to 18). In boys, age-related gains in Hmax were similar to those observed for other mechanography outcomes (89% increase from age 9 to 18), with smaller gains thereafter (Figures 2b & 4b).
Sex and ethnic differences in mechanography outcomes
With the exception of Efficiency, all mechanography outcomes were significantly greater in girls (range 6-20%) compared with boys at age 9 (Table 9). Fmax/BW was also significantly greater in girls (4-5%) compared with boys at age 10 and 11. Boys demonstrated an advantage in muscle power compared with girls at age 12 (Pmax, Pmax/mass) that persisted into young adulthood (5-65%), whereas boys’ advantage in Fmax/BW was not apparent until age 17 (4-10%). Boys demonstrated greater Efficiency from age 11 to 19 (5-9%), and greater jump velocity and maximum jump height compared with girls at age 12 and thereafter (6-45%).
The magnitude of sex differences persisted after adjustment for height, with the exception of absolute power and Efficiency. Pmax was similar between boys and girls until age 11 and greater in boys thereafter. Efficiency was greater in boys from age 11 to 18 years.
With the exception of Pmax, which was similar across ethnicities, all mechanography parameters (Pmax/mass, Fmax/BW, Efficiency, Vmax, and Hmax) were 3-9% greater in Asian compared with white participants. After adjustment for height, all mechanography parameters (including Pmax) were significantly greater in Asian compared with white participants by 4-10%.
Discussion
We present reference data for jumping mechanography outcomes in Canadian children, adolescents and young adults using the S2LJ with the static hands-on-waist protocol – as none existed previously. Our findings complement normative datasets for jumping mechanography using varying protocols in European children and youth[7,9,15,24].
Jumping mechanography is an objective and reproducible measure of muscle function, and a good choice to assess muscle force and power across groups, including healthy children[2,25,26] and those with clinical needs[27,28], master athletes[29] and older adults[30]. Standard mechanography protocol for a S2LJ has participants performing the jump with freely moving arms. Compared with the hands-on-hip protocol we used, with an upward arm swing participants achieve greater jump height[20,31,32] and greater muscle power[20], on average. We compared our jumping mechanography outcomes (static arms protocol) with reported values for a sample of 796 children and adolescents aged 9 to 18 years from the Czech Republic, who performed the S2LJ with freely moving arms[7]. In our sample, Hmax and Pmax were 13-19% and 17-20% lower, respectively, and these differences were systematic across all ages. Similarly, EFI z-score was approximately 9% lower in our sample, compared with the reference population (provided by the manufacturer of the Leonardo[15]), with the S2LJ performed with freely moving arms; data not shown (EFI z-score= -0.68 for girls; -0.66 for boys, on average; data not shown).
Whereas the freely moving arms protocol has been more widely used and may be a more appropriate method to assess muscle function in some athlete groups where maximum jump height is the primary outcome of interest[33], the static arm protocol may be a more reproducible method and more readily standardized for field-based measurement. Including an arm swing produces results that vary more with skill level[13,34] and may lead to larger differences between sexes[35]. In addition, the biomechanical four-segment model (segment 1= shoulder to hip including arms, segment 2= hip to knee, segment 3= knee to ankle, segment 4= ankle to toe) produced with hands-on-hips eliminates all contribution of the arms to the outcome and permits a better focus on muscle actions in the lower limbs[14]. Thus, we envision that our reference data will be useful to clinicians and researchers as an alternative to the S2LJ protocol and may be more appropriate for use in heterogeneous populations with individuals of varying athletic ability.
In both sexes, mechanography values (except Fmax/BW) were lower for younger children as compared with those in early adolescence. However, the magnitude of the age-related difference across years in muscle power and force (unadjusted) and jump height was greater for boys, compared with girls. Further, girls reached a plateau earlier in adolescence compared with boys. These findings are consistent with girls approximately two years earlier maturity compared with boys, assessed using peak height velocity[36]. Further, a previous Canadian study using longitudinal data, demonstrated a close link between age-related gains in muscle function during growth and increased height (which peaked approximately 5 months before the peak in muscle mass accrual)[37] and peak bone mass which occurred approximately 5 months after peak muscle mass accrual. Finally, androgens play a key role in muscle mass accrual; specifically, higher testosterone levels in boys during puberty generate much greater gains in muscle mass and function compared with girls[38].
The magnitude of the difference in muscle function between boys and girls varied across chronological age. Boys’ advantage in Pmax and Pmax/mass was evident at age 12. The timing for peak values in our sample of boys is one to two years earlier than observed in previous studies[7,39,40]. This may reflect the ethnic diversity of our cohort (32% were Asian). To this point, we previously reported that Asian boys and girls mature earlier compared with their white peers[16]; and in the current study Asian participants demonstrated greater values for some mechanography parameters compared with their white peers.
It is important to note that although comparisons between girls and boys based on chronological age is common, especially in clinical practice, we view this as a limitation. Given the well-documented sex differences in the tempo and timing of maturity[36] and the influence of maturation on muscle development[38], all studies would benefit from comparing girls and boys aligned on a common maturational landmark, such as age at peak height velocity. This approach was adopted for and longitudinal studies of bone and muscle development[37,41], but has not yet been utilized in pediatric jumping mechanography studies.
Relative to body weight, Fmax remained relatively constant in boys across ages, similar to previous observations for Fmax/BW during multiple one-legged hopping[7,24] and the S2LJ[15]. However, in girls, Fmax/BW declined with age. This difference may reflect different protocols; that is hands-on-waist versus hands free and S2LJ versus multiple one-legged hopping. Multiple one-legged hopping produces greater peak force and continues to increase in later adolescence (approximately 5% between 16 and 18 years)[7]. In our cohort, Fmax remained constant from age 16 onwards (data not shown). In contrast we noted an 11% difference in body mass between girls at age 9 (56 kg, on average) compared with young women at age 21 (63 kg, on average). Therefore, Fmax relative to body weight (mass * gravity) decreased slightly as the ratio of Force:Mass declined.
Boys’ advantage in Efficiency was evident from age 11 to 19 years. From the perspective of human locomotion, the most efficient movement is that which achieves a given power with the smallest force[20]. Thus, compared with same-aged girls, boys use less force to achieve the same power output. The Efficiency parameter was recently introduced by the manufacturer, and was not reported in previous reference data sets for mechanography outcomes. Thus, we are unable to compare Efficiency values in our cohort to those in other studies. However, Efficiency values in our study fluctuated around 100% of those from the manufacturer’s reference group, indicating similarities between our sample and the reference population.
Vertical jump height and velocity also increased with age in both sexes; greater jumping performance was evident in boys at age 12. This is similar to previous studies that used the hands-on-waist protocol[42,43]. Temfemo et al.[42] reported jump height during a countermovement jump as similar between girls and boys until age 12. After age 12 they explained the higher jump heights for boys by an increase in the percentage of fast twitch muscle fibres. Also, boys at age 14 had significantly greater leg length and muscle volume that also contributed to greater jump performance, compared with girls.
We note that our study has a number of limitations. First, our cohort is a convenience sample of boys and girls. Therefore, we can not say that it is represents a larger population of Canadian boys and girls, nor that recruitment, based on self selection into the study, was free from selection bias. Our sample was taller and weighed more than the 2000 reference population of U.S. children and youth. The ethnic diversity of our sample, while it represents the demographic make-up of Metro Vancouver[18], may also partially explain this difference. Second, performance during the S2LJ test is influenced by muscle power, coordination, balance and jumping technique[10]. Precision data are not currently available for the S2LJ with hands-on-hips for children. Further, motor coordination likely depends on level of physical activity[44], which also differs between girls and boys in childhood and adolescence[45]. Future studies might examine how sex differences in mechanography outcomes are influenced by these and other factors.
In conclusion, the hands-on-waist protocol for jumping mechanography may be an attractive field test option to examine muscle strength and power in children, adolescents and young adults. The sex- and age-specific data we provide for healthy Canadian children and youth may prove a useful reference for clinicians and researchers.
Acknowledgements
We gratefully acknowledge the HBSIII and Fracture and Risk-taking Behaviour Study participants, their families, and the support from prinicipals and teachers at volunteer schools in the Richmond and Vancouver School Districts. We would also like to acknowledge the research teams in the Physical Activity and Child and Youth Health Research Group and in the Department of Orthopaedics at BC Children’s Hospital. HBSIII was supported by the Canadian Institutes of Health Research (CIHR; MOP-84575), the Michael Smith Foundation for Health Research (MSFHR), the British Columbia Health Research Foundation (2400–2 and 10898–2), and 2010 Legacies Now. The Fracture Study was supported by CIHR (OBM- 101391). LG was supported by a CIHR Doctoral Research Award.
Footnotes
The authors have no conflict of interest.
Edited by: F. Rauch
References
- 1.Wolfe RR. The underappreciated role of muscle in health and disease. Am J Clin Nutr. 2006;84:475–82. doi: 10.1093/ajcn/84.3.475. [DOI] [PubMed] [Google Scholar]
- 2.Rauch R, Veilleux L-N, Rauch F, Bock D, Welisch E, Filler G, et al. Muscle force and power in obese and overweight children. J Musculoskelet Neuronal Interact. 2012;12:80–3. [PubMed] [Google Scholar]
- 3.Lang P-O, Michel J-P, Zekry D. Frailty syndrome: a transitional state in a dynamic process. Gerontology. 2009;55:539–49. doi: 10.1159/000211949. [DOI] [PubMed] [Google Scholar]
- 4.Frost HM. Bone “mass” and the “mechanostat”: a proposal. Anat Rec. 1987;219:1–9. doi: 10.1002/ar.1092190104. [DOI] [PubMed] [Google Scholar]
- 5.Schoenau E, Frost HM. The “muscle-bone unit” in children and adolescents. Calcif Tissue Int. 2002;70:405–7. doi: 10.1007/s00223-001-0048-8. [DOI] [PubMed] [Google Scholar]
- 6.Jones Stratton G. Muscle function assessment in children. Acta Paediatr. 2000;89:753–61. [PubMed] [Google Scholar]
- 7.Sumnik Z, Matyskova J, Hlavka Z, Durdilova L, Soucek O, Zemkova D. Reference data for jumping mechanography in healthy children and adolescents aged 6-18 years. J Musculoskelet Neuronal Interact. 2013;13:297–311. [PubMed] [Google Scholar]
- 8.Tikkanen O, Haakana P, Pesola AJ, Häkkinen K, Rantalainen T, Havu M, et al. Muscle activity and inactivity periods during normal daily life. PLoS ONE. 2013;8:e52228. doi: 10.1371/journal.pone.0052228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fricke O, Weidler J, Tutlewski B, Schoenau E. Mechanography - a new device for the assessment of muscle function in pediatrics. Pediatr Res. 2006;59:46–9. doi: 10.1203/01.pdr.0000191580.07644.1c. [DOI] [PubMed] [Google Scholar]
- 10.Veilleux L-N, Rauch F. Reproducibility of jumping mechanography in healthy children and adults. J Musculoskelet Neuronal Interact. 2010;10:256–66. [PubMed] [Google Scholar]
- 11.Hara M, Shibayama A, Takeshita D, Hay DC, Fukashiro S. A comparison of the mechanical effect of arm swing and countermovement on the lower extremities in vertical jumping. Hum Movemen Sci. 2008;27:636–48. doi: 10.1016/j.humov.2008.04.001. [DOI] [PubMed] [Google Scholar]
- 12.Canavan PK, Vescovi JD. Evaluation of power prediction equations: peak vertical jumping power in women. Med Sci Sports Exerc. 2004;36:1589–93. doi: 10.1249/01.mss.0000139802.96395.ac. [DOI] [PubMed] [Google Scholar]
- 13.Richter A, Räpple S, Kurz G, Schwameder H. Countermovement jump in performance diagnostics: Use of the correct jumping technique. Eur J Sport Sci. 2012;12:231–7. [Google Scholar]
- 14.Aragon-Vargas LE, Gross MM. Kinesiological factors in vertical jump performance: Differences among individuals. J Appl Biomech. 1997;13:24–44. [Google Scholar]
- 15.Busche P, Rawer R, Rakhimi N, Lang I, Martin DD. Mechanography in childhood: references for force and power in counter movement jumps and chair rising tests. J Musculoskelet Neuronal Interact. 2013;13:213–26. [PubMed] [Google Scholar]
- 16.Gabel L, Nettlefold L, Brasher PM, Moore SA, Ahamed Y, Macdonald HM, et al. Reexamining the Surfaces of Bone in Boys and Girls During Adolescent Growth: A 12-Year Mixed Longitudinal pQCT Study. J Bone Miner Res. 2015;30:2158–67. doi: 10.1002/jbmr.2570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Määttä M, Macdonald HM, Mulpuri K, McKay HA. Deficits in distal radius bone strength, density and microstructure are associated with forearm fractures in girls: an HR-pQCT study. Osteoporos Int. 2015;26:1163–74. doi: 10.1007/s00198-014-2994-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Statistics Canada. Vancouver, CMA, British Columbia (Code 933) (table). National Household Survey (NHS) Profile. 2011 National Household Survey. Statistics Canada Catalogue no. 99-004-XWE. Ottawa: 2013. [accessed September 8 2016]. Released September 11 2013. Available at: http://www12.statcan.gc.ca/nhs-enm/2011/dp-pd/prof/index.cfm?Lang=E . [Google Scholar]
- 19.Cavagna GA. Force platforms as ergometers. J Appl Physiol. 1975;39:174–9. doi: 10.1152/jappl.1975.39.1.174. [DOI] [PubMed] [Google Scholar]
- 20.Matheson LA, Duffy S, Maroof A, Gibbons R, Duffy C, Roth J. Intra- and inter-rater reliability of jumping mechanography muscle function assessments. J Musculoskelet Neuronal Interact. 2013;13:480–6. [PubMed] [Google Scholar]
- 21.Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, Flegal KM, Guo SS, Wei R, et al. CDC growth charts: United States. Adv Data. 2000;314:1–27. [PubMed] [Google Scholar]
- 22.Cole TJ, Green PJ. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med. 1992;11:1305–19. doi: 10.1002/sim.4780111005. [DOI] [PubMed] [Google Scholar]
- 23.Cole TJ, Freeman JV, Preece MA. British 1990 growth reference centiles for weight, height, body mass index and head circumference fitted by maximum penalized likelihood. Stat Med. 1998;17:407–29. [PubMed] [Google Scholar]
- 24.Lang I, Busche P, Rakhimi N, Rawer R, Martin DD. Mechanography in childhood: references for grip force, multiple one-leg hopping force and whole body stiffness. J Musculoskelet Neuronal Interact. 2013;13:227–35. [PubMed] [Google Scholar]
- 25.Anliker E, Dick C, Rawer R, Toigo M. Effects of jumping exercise on maximum ground reaction force and bone in 8- to 12-year-old boys and girls: a 9-month randomized controlled trial. J Musculoskelet Neuronal Interact. 2012;12:56–67. [PubMed] [Google Scholar]
- 26.Ward KA, Das G, Berry JL, Roberts SA, Rawer R, Adams JE, et al. Vitamin D status and muscle function in post-menarchal adolescent girls. J Clin Endocrinol Metab. 2009;94:559–63. doi: 10.1210/jc.2008-1284. [DOI] [PubMed] [Google Scholar]
- 27.Edouard T, Deal C, Van Vliet G, Gaulin N, Moreau A, Rauch F, et al. Muscle-bone characteristics in children with Prader-Willi syndrome. J Clin Endocrinol Metab. 2012;97:E275–81. doi: 10.1210/jc.2011-2406. [DOI] [PubMed] [Google Scholar]
- 28.Veilleux L-N, Lemay M, Pouliot-Laforte A, Cheung MS, Glorieux FH, Rauch F. Muscle anatomy and dynamic muscle function in osteogenesis imperfecta type I. J Clin Endocrinol Metab. 2014;99:E356–62. doi: 10.1210/jc.2013-3209. [DOI] [PubMed] [Google Scholar]
- 29.Michaelis I, Kwiet A, Gast U, Boshof A, Antvorskov T, Jung T, et al. Decline of specific peak jumping power with age in master runners. J Musculoskelet Neuronal Interact. 2008;8:64–70. [PubMed] [Google Scholar]
- 30.Belavý DL, Armbrecht G, Blenk T, Bock O, Börst H, Kocakaya E, et al. Greater association of peak neuromuscular performance with cortical bone geometry, bone mass and bone strength than bone density: A study in 417 older women. Bone. 2016;83:119–26. doi: 10.1016/j.bone.2015.10.018. [DOI] [PubMed] [Google Scholar]
- 31.Markovic G, Dizdar D, Jukic I, Cardinale M. Reliability and factorial validity of squat and countermovement jump tests. J Strength Cond Res. 2004;18:551. doi: 10.1519/1533-4287(2004)18<551:RAFVOS>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 32.Feltner ME, Fraschetti DJ, Crisp RJ. Upper extremity augmentation of lower extremity kinetics during countermovement vertical jumps. J Sports Sci. 1999;17:449–66. doi: 10.1080/026404199365768. [DOI] [PubMed] [Google Scholar]
- 33.Harman EA, Rosenstein MT, Frykman PN. The effects of arms and countermovement on vertical jumping. Med Sci Sports Exerc. 1990;1990:825–33. doi: 10.1249/00005768-199012000-00015. [DOI] [PubMed] [Google Scholar]
- 34.Coulson M, Archer D. Practical Fitness Testing. Bloomsbury Publishing; 2015. [Google Scholar]
- 35.Walsh MS, Böhm H, Butterfield MM, Santhosam J. Gender bias in the effects of arms and countermovement on jumping performance. J Strength Cond Res. 2007;21:362–6. doi: 10.1519/R-19825.1. [DOI] [PubMed] [Google Scholar]
- 36.Bailey DA, McKay HA, Mirwald RL, Crocker PR, Faulkner RA. A six-year longitudinal study of the relationship of physical activity to bone mineral accrual in growing children: The University of Saskatchewan Bone Mineral Accrual Study. J Bone Miner Res. 1999;14:1672–9. doi: 10.1359/jbmr.1999.14.10.1672. [DOI] [PubMed] [Google Scholar]
- 37.Rauch F, Bailey DA, Baxter-Jones A, Mirwald R, Faulkner R. The “muscle-bone unit” during the pubertal growth spurt. Bone. 2004;34:771–5. doi: 10.1016/j.bone.2004.01.022. [DOI] [PubMed] [Google Scholar]
- 38.Tanner JM. Growth and maturation during adolescence. Nutr Rev. 1981;39:43–55. doi: 10.1111/j.1753-4887.1981.tb06734.x. [DOI] [PubMed] [Google Scholar]
- 39.Martin RJF, Dore E, Twisk J, van Praagh E, Hautier CA, Bedu M. Longitudinal changes of maximal short-term peak power in girls and boys during growth. Med Sci Sports Exerc. 2004;36:498–503. doi: 10.1249/01.mss.0000117162.20314.6b. [DOI] [PubMed] [Google Scholar]
- 40.Doré E, Martin R, Ratel S, Duché P, Bedu M, Van Praagh E. Gender differences in peak muscle performance during growth. Int J Sports Med. 2005;26:274–80. doi: 10.1055/s-2004-821001. [DOI] [PubMed] [Google Scholar]
- 41.Farr JN, Laddu DR, Blew RM, Lee VR, Going SB. Effects of physical activity and muscle quality on bone development in girls. Med Sci Sports Exerc. 2013;45:2332–40. doi: 10.1249/MSS.0b013e31829c32fe. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Temfemo A, Hugues J, Chardon K, Mandengue S-H, Ahmaidi S. Relationship between vertical jumping performance and anthropometric characteristics during growth in boys and girls. Eur J Pediatr. 2009;168:457–64. doi: 10.1007/s00431-008-0771-5. [DOI] [PubMed] [Google Scholar]
- 43.Malina RM, Bouchard C, Bar-Or O. Growth, Maturation, and Physical Activity. Champaign, IL: Human Kinetics; 2004. [Google Scholar]
- 44.Fagard J. Skill acquisition in children: a historical perspective. In: Bar-Or O, editor. The child and adolescent athlete. Champaign, IL: Blackwell Science; 1996. [Google Scholar]
- 45.Nader PR, Bradley RH, Houts RM, Mcritchie SL, O’brien M. Moderate-to-Vigorous Physical Activity From Ages 9 to 15 Years. JAMA. 2008;300:295–305. doi: 10.1001/jama.300.3.295. [DOI] [PubMed] [Google Scholar]