

Abstract
The lumbar spine is subjected to considerable stress during many athletic efforts. The purpose of this study was to assess the effects of physiological loading on the lumbar spine in national male players of different games, which may be predictive of the future development of low back pain and injury symptoms. Thirty-four national players (12 cricket players, 12 field hockey players, and 10 basketball players) underwent magnetic resonance imaging, and selected geometric variables including intervertebral disc angles, the Farfan ratio, the lumbar body index, the compression deformity ratio, the biconcave deformity ratio and the anterior wedge deformity ratio were measured using KINOVEA-0.8.15 software and syngo fast view software and calculated using specific formulas. The results indicated a significant difference in the intervertebral disc angle between the three groups at the L2/3, L3/4 and L4/5 levels. In relation to the lumbar vertebral body shape and size, significant differences were found in the lumbar index at the L2 level, in the biconcave deformity at the L1 and L2 levels and in relation to the anterior wedge deformity at L2 between the three selected groups. Our data suggest that the different physiological loadings in the selected sports play an important role in the development of degenerative changes of the lumbar spine, which may be considered a risk factor for future injury and/or low back pain in each specific sport because of the unique demands of each discipline.
Key words: degenerative changes, magnetic resonance imaging, basketball, cricket, field hockey
Introduction
Sport and exercise are stressful by their nature, and over-stressful activity may produce injury (Clement et al., 1981). The lumbar spine is subjected to considerable stress during many athletic endeavors; therefore, abnormalities involving this region may cause injuries and pain among athletes because of the unique demands of the related sport.
Independent variables that contribute individually or in combination to lumbar spine injury include poor technique, poor conditioning, and abnormal anatomy; thus, young athletes may have a spinal deformity that is incidentally or potentially related to their sport (d’Hemecourt and Hresko, 2012).
Heavy physical work can lead to degenerative changes of the spine (Tertti et al., 1990; Videman et al., 1990), and one factor that can dramatically affect the load on the lumbar spine is a body position. In comparison to the load that is present during upright standing, compression on the lumbar spine increases with sitting and increases more with spinal flexion. Another factor that affects loading of the lumbar spine is body movement speed. Compressive damage arising from repetitive loading is most likely a common event in life; vertebral body damage decompresses the adjacent disc and subsequently leads to internal disc disruption and further degenerative changes. As degeneration advances, the height of the disc is diminished, and the distribution of force across the motion segment changes (Adams et al., 2000; Crock, 1986; Holm et al., 2004).
The capacity of the spine to resist injury is decreased if the forces applied involve flexion and are of long duration (Adams and Hutton, 1982). Based on previous studies, the vertebral unit suffers a gradual change in its dimensions under the application of a constant load (Kazarian, 1975). It has been demonstrated that the load on the spine in physical activity can be measured using changes in the stature (Boocock et al., 1986).
Cricket, basketball and field hockey are popular sports that are played around the world. Spinal loading is implicated in back injuries in cricket, whereas field invasive games such as hockey and basketball create unique physiological and physical demands on the players. For example, playing and dribbling the ball are usually executed in a position of spinal flexion. Injuries to the lumbar spine as a result of participation in field hockey have been reported in epidemiological studies (Murtaugh, 2001; Rishiraj et al., 2009).
Repetitive loading can create microscopic damage within a material or tissue, which gradually builds up until gross failure occurs. In living tissues, the process of damage accumulation is opposed by the process of adaptive remodeling (Adams et al., 2013).
In an analysis of force transmission and in model studies on the spinal column in high level athletes, it is necessary to estimate the geometric parameters of a studied object. It is particularly important to determine the sizes of intervertebral discs, vertebra and the shape of the vertebral column (Ogurkowska, 2007).
It is conventional to define vertebral body height in three places: the anterior and posterior margins (Ha and Hp) and halfway between these margins (Hm). Three types of vertebral deformities can then be defined by comparing these heights with each other and with the anterior-posterior diameter (Dap) of the vertebral body. Thus, an anterior wedge deformity is characterized by a low Ha/Hp ratio; a biconcave deformity is characterized by a low Hm/Hp ratio and a compression deformity is characterized by a low Hp/Dap ratio (Adams et al., 2013).
Ruyssen-Witrand et al. (2007) proposed that “vertebral size should be considered as a potential independent vertebral fracture risk factor”.
Therefore, since overloading the lumbar spinal column is promoted by unfavorable biomechanical situations, it can be linked to executed work or professional sport activities (Smith and Loschner, 2002).
This study attempted to assess the effects of loading on the lumbar spine through magnetic resonance imaging (MRI), which is considered to represent the most accurate method for imaging the spine (Crewe et al., 2012). In the present study, a few ergonomic parameters related to intervertebral disc angles and ratio, as well as vertebral body size and shape, which may be considered as predictive values for future lower back pain or injury, were observed in the three groups of cricket, field hockey and basketball athletes. Degenerative changes were compared in the three selected sports, which may predict future disability or injury.
Material and Methods
Participants
For the purpose of this study, 34 national players including 12 cricket players, 12 field hockey players and 10 basketball players with a mean ± standard deviation (SD) age of 23 ± 3 years, 22 ± 3 years, and 20 ± 2 years, respectively, with and without symptoms of lumbar pain underwent a case history and a physical examination. All the participants provided informed consent before commencing the experiment, and participants with a history of operation in their spine and a history of smoking were excluded from the study.
Measures
The pain description for each player was identified after filling out a self-reported questionnaire and completing a physical examination conducted by an orthopedic specialist. The age, body height and mass as well as the body mass index (BMI) of all the subjects were documented. None of the participants were receiving medication. Magnetic resonance imaging (MRI) with a dedicated scanner of 1.5 Tesla was performed by technicians from lateral views of all the participants’ lumbar spine and sacral regions.
Procedures
Since the study focused on the lower back (lumbar spine), after completing the imaging process, selected geometric variables including intervertebral disc angles, the Farfan ratio, the lumbar body index, compression deformities (Hp/Dap ratio), biconcave deformities (Hm/Hp ratio) and anterior wedge deformities (Ha/Hp ratio) were assessed from images of the lumbar region using KINOVEA-0.8.15 software and syngo fast view software. Selected indexes were calculated using specific formulas described below.
For studying discs, the intervertebral lumbar disc angle was measured as the angle created by the intersection of lines drawn through the lumbar vertebral endplates. The Farfan ratio (disc space ratio) was calculated using the following formula: (Hpd + Had) / Dap (Smith et al., 1996). This quantity thus reflects the disc height relative to its diameter.
After measuring the anterior, posterior and middle height of each lumbar vertebra and the anterior posterior diameter of each lumbar vertebra, the lumbar body index for each vertebral body was calculated by dividing the posterior height of the lumbar vertebra by the anterior height of the lumbar vertebra (Smith et al., 1996). The anterior wedge deformity for each vertebral body was calculated by dividing the anterior height of the lumbar vertebra by the posterior height of the lumbar vertebra (Ha/Hp ratio). The biconcave deformity for each vertebral body was calculated by dividing the middle height of the lumbar vertebra by the posterior height of the lumbar vertebra (Hm/Hp ratio). Finally, the compression deformity shown by the Hp/Dap ratio for each vertebral body was calculated by dividing the posterior height of the lumbar vertebra by the anterior posterior diameter (Adams et al., 2013).
Statistical Analysis
The data were tested using a one-way analysis of variance for differences between the three selected sports for the purpose of observing the effects of loading on degenerative changes of the lumbar spine caused by playing different sports. Finally, the Scheffé post hoc test was performed for the levels in which a significant difference had been found. Independent t–tests were used to determine the difference between players with and without symptoms of lumbar pain in selected biometrical variables. The data analysis was performed using SPSS software (version 17.0), and the level of significance was set at 0.05.
Results
Our findings showed that in a comparison of the three selected sport groups, there was no significant difference in relation to age, body mass, height and the BMI, suggesting that these factors did not have any major effects on the results of the study.
The intervertebral disc angles and the Farfan ratios in each level of the lumbar spine in the different selected sports are described in Table 1. It was observed that cricket players had the lowest disc angles and Farfan ratios in all levels of the lumbar spine, whereas the field hockey players had the highest values, except in L5/S1 in which the basketball players had the highest disc angle and the lowest Farfan ratio. However, in a one-way ANOVA (Table 2) and the Scheffé post hoc test (Table 3) of the significant levels, a significantly lower intervertebral disc angle (IDA) was found in the cricket players compared with the field hockey players in the L2/L3 level; additionally, in the level L3-L4 cricket players had a significantly lower intervertebral disc angle when compared with the other two groups.
Table 1.
Descriptive statistics of each intervertebral disc and vertebral body related factors in each level of the lumbar spine
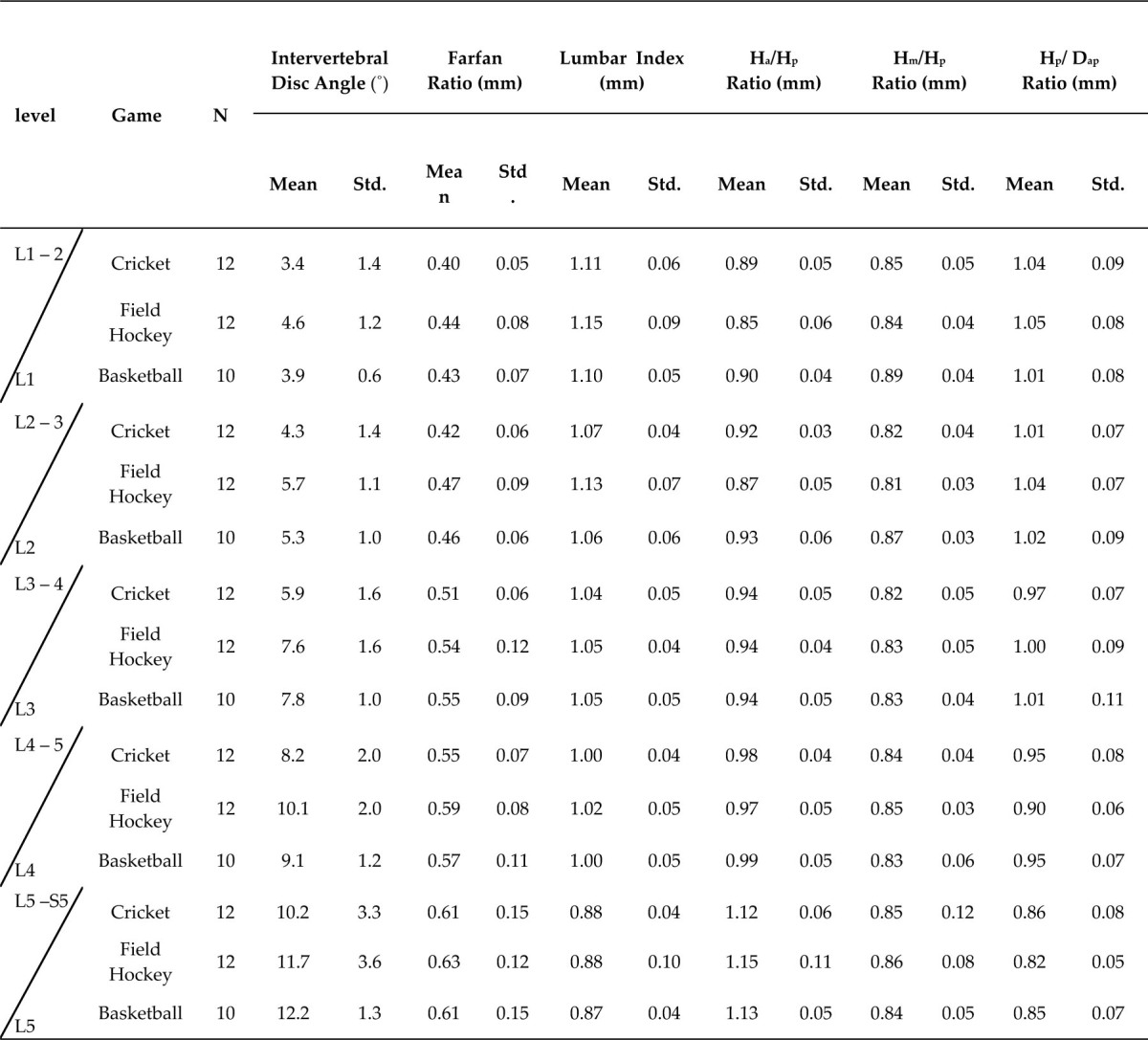
Table 2.
One way ANOVA between cricket, field hockey and basketball groups in relation to each intervertebral disc and vertebral body related factors in each level of the lumbar spine
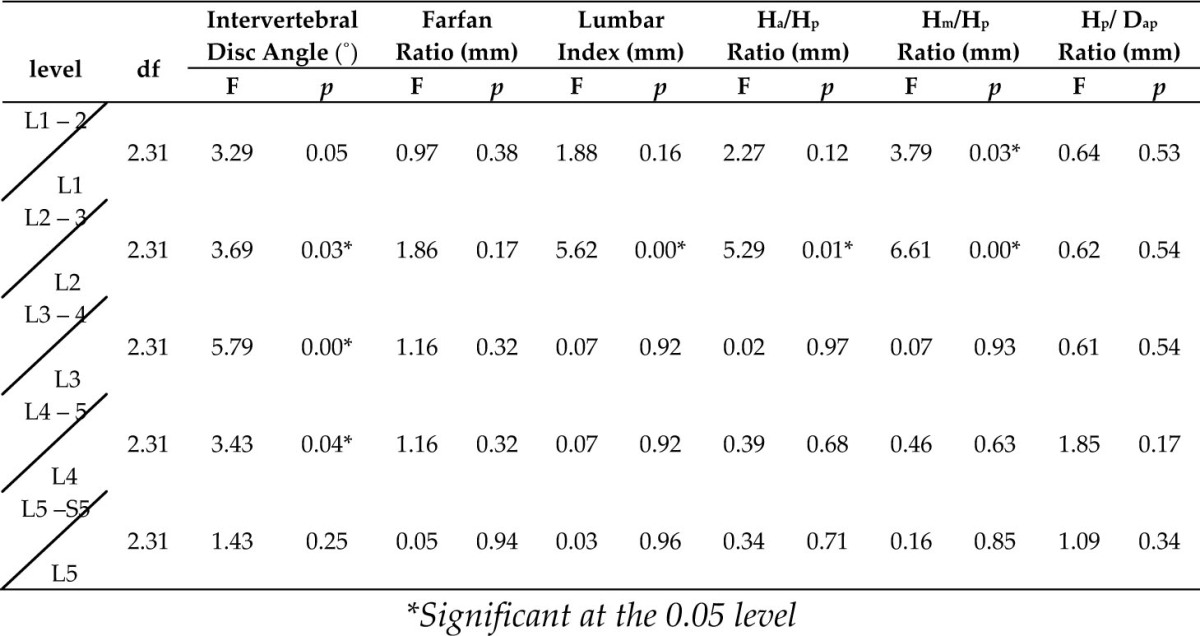
Table 3.
The Scheffé post-hoc test in significant levels in relation to each intervertebral disc and vertebral body related factors in each level of the lumbar spine
| Dependent Variable | (I) Game | (J) Game | Mean Difference (I-J) | SE | p |
|---|---|---|---|---|---|
| Lumbar Index at the L2 level | Field Hockey | Cricket | 0.06 | 0.02 | 0.03 |
| Lumbar Index at the L2 level | Field Hockey | Basketball | 0.07 | 0.02 | 0.02 |
| Ha/Hp ratio at the L2 level | Field Hockey | Basketball | -0.06 | 0.02 | 0.01 |
| Hm/Hp ratio at the L1 level | Field Hockey | Basketball | -0.04 | 0.01 | 0.04 |
| Hm/Hp ratio at the L2 level | Basketball | Cricket | 0.04 | 0.01 | 0.03 |
| Hm/Hp ratio at the L2 level | Basketball | Field Hockey | 0.05 | 0.01 | 0.00 |
| Disc Angle at the L2-L3 level | Cricket | Field Hockey | -1.33 | 0.50 | 0.04 |
The field hockey players had a significantly higher lumbar index compared with the cricket players and basketball players at the L2 level.
At the level of L2 the Ha/Hp ratio and the Hm/Hp ratio were lower for the field hockey players than for the basketball players. The field hockey players had more anterior wedge deformities (lower Ha/Hp ratio) in the level L2 and more biconcave deformities (lower Hm/Hp ratio) compared with the basketball players in levels L1 and L2 (Tables 2 and 3).
The cricket players had more biconcave deformities (lower Hm/Hp Ratio) compared with the basketball players at the level L2, but no significant differences were observed in our MRI examination of the lumbar spine in other levels according to the criteria for degenerative changes that were used.
Compression deformities, which were indicated by the Hp/Dap ratio, did not show any significant differences between the three groups. However, according to our observations, it appeared that more compression deformities were present in the L4 and L5 levels in the field hockey players and more compression deformities were present in the level L1 in the basketball players compared to the other two groups. In contrast to these MRI findings, however, no difference was found between the two groups of athletes with and without symptoms of lumbar pain in relation to the criteria for degenerative changes that were used in this study.
Figure 1.

Measurement of Ha, Hp, Hm, Hpd, Had and Dap
Discussion
Athletes and coaches in sports that have an increased risk of lumbar spine injury should be educated in preventive techniques. An athlete with back pain should seek medical assessment early to prevent progression to more severe tissue injury. Loading in different sports appears to play an important role in the development of radiographic changes of the lumbar spine as one factor that can dramatically affect the load on the lumbar spine is a body position (Dolan et al., 1994).
Therefore, for assessing the effects of loading in the present study, degeneration and abnormalities of the lumbar spine in three sports were compared. It was assumed that different body positions and different body accelerations during play caused different abnormalities in the lumbar spine.
Several studies had been conducted that compared lumbar spine abnormalities of elite athletes with non-athletic groups in various sports such as wrestling, soccer, tennis, track and field and gymnastics (Jones et al., 1999; Lundin et al., 2001; Schmitt et al., 2004). Murtaugh (2001) investigated the rates and types of injuries experienced by field hockey players and reported that low back was the most commonly injured region. Reilly and Temple (1993) demonstrated that an enhanced crouched position when dribbling accentuated the subjective and physical strain on the spine.
In this study, we focused on three groups with the same range of age, the sports level and the BMI to exclude the effects of these factors on our results. In an analysis of force transmission and in model studies on the spinal column in professional rowers, Ogurkowska (2007) reported that it was necessary to estimate the geometric parameters of a studied object. It is particularly important to determine sizes of intervertebral discs, vertebra and the shape of the vertebral column.
Our findings showed that in cricket players, movements involved the frequent hyper extension and rotation of the spinal column, which could be hypothesized to lead to a height reduction in the intervertebral discs; therefore, repeated hyper extension and body acceleration could have larger negative effects on the discs in levels L2/3, L3/4 and L4/5. Greater signs of disc degeneration of the lumbar spine could be demonstrated in cricket players compared with basketball and field hockey players, which may lead to the possibility of developing a later stage of low back pain (LBP) earlier in comparison with the other two selected sport disciplines.
Dabbs and Dabbs (1990) reported that there was a poor correlation between intervertebral disc (IVD) narrowing and the development of LBP; additionally, Lundin et al. (2001) determined a significant correlation between back pain and a decrease in disc height during the 13-year follow-up period.
Significant differences in disc height between the different disciplines of track and field were found in levels L1/2 and L3/4 in a study reported by Schmitt et al. (2004), and greater signs of disc degeneration of the lumbar spine were demonstrated in weight lifters and soccer players compared to runners and shooters (Videman et al., 1995). Another study showed more radiographic abnormalities (MRI) in gymnasts than in swimmers (Goldstein et al., 1991).
According to Alexander (1985), the type of injury that occurs in the lumbar spine is dependent on the direction, magnitude, and the point of application of the forces to the spine. Overloading of the lumbar spinal column is promoted by unfavorable biomechanical situations that are linked to executed work or professional sport activities (Smith and Loschner, 2002). Ruyssen-Witrand et al. (2007) proposed that “vertebral size should be considered a potential independent vertebral fracture risk factor”. Additionally, several studies have reported that repetitive loading on the spine can cause the compressive failure of vertebral bodies (Wolfram et al., 2011).
Repetitive loading can create microscopic damage within a material or tissue, which gradually builds up until gross failure occurs. In living tissues, the process of damage accumulation is opposed by the process of adaptive remodeling (Adams, 2004); therefore, an examination of vertebral body deformation, the lumbar index, the biconcave ratio, the compression ratio and the anterior wedge deformity were calculated in the present study.
The findings showed that by comparing the lumbar vertebral body in the three selected sports, cricket and basketball players in the L2 level showed a significantly lower lumbar index compared with field hockey players. However, in the level L2, it was observed that field hockey players had more anterior wedge deformities (lower Ha/Hp ratio) compared with basketball players. More biconcave deformities (lower Hm/Hp ratio) were observed in field hockey players compared with basketball players in the L1 and L2 levels and in cricket players compared with basketball players in the level L2.
Loading in different sports appears to play an important role in the lumbar spine as shown by our results. It appears that the second, third and fourth lumbar intervertebral discs in cricket players are more at risk for degenerative deformities, as is the second lumbar vertebra that may be affected with biconcave deformities. Schmitt et al. (2004) reported that the concavity index at all levels of the lumbar spine did not show significant differences between the different groups of athletes in track and field.
Field hockey players must pay greater attention to their higher levels of lumbar spine vertebral body deformations, particularly anterior wedge deformities and biconcave deformities. Playing and dribbling the ball in field hockey are usually executed in a position of spinal flexion; Reilly and Temple (1993) also demonstrated that an enhanced crouched position when dribbling accentuated the subjective and physical strain on the spine. Reilly and Seaton (1990) observed an average spinal shrinkage rate of 0.4 mm/min in players dribbling a hockey ball.
In field hockey, athletes must bend and rotate their bodies. It is possible that the patterns of loading experienced by the field hockey players during dribbling and frequent flexion could explain the higher rates of radiographic changes of the vertebral body in levels L1 and L2 that were observed compared with players representing other disciplines.
Although no other significant differences were observed in our MRI examination of the lumbar spine in other levels or in compression deformities, which are indicated by the Hp / Dap ratio, it appeared that more compression force was present in the L4 and L5 levels in hockey players and in the level L1 in basketball players compared to the other groups of athletes. This observation requires more attention to be hypothesized as a risk factor for stress fractures in the future.
It appears that second, third and fourth lumbar intervertebral discs in cricket players are more at risk for degenerative deformities, and it is suggested that hockey players should pay more attention to their higher levels of the lumbar spine for anterior wedge deformities and biconcave deformities.
As we observed, the changes appeared to be more severe at the second lumbar vertebral body and the second, third and fourth lumbar discs because of the greater mobility that may be present at these levels.
In this study we tried to show the different effects of three different sports on the lumbar spine of national level players, however, the factors like diet, sleep, physical and mental condition of the participants was not be controlled; another limitation related to the study includes a lack of the control group of males with similar age that do not practice sports competitively and have healthy spines.
Acknowledgements
The authors would like to thank to athletes who participated in this study, and the Orthopaedics Department and MRI centre technicians of S.S. Hospital, Banaras Hindu University for their support during data collection for this study.
Authors submitted their contribution to the article to the editorial board.
References
- Adams MA. Biomechanics of back pain. Acupunct Med. 2004;22(4):178–188. doi: 10.1136/aim.22.4.178. [DOI] [PubMed] [Google Scholar]
- Adams M, Bogduk N, Burton K, Dolan P. The Biomechanics of Back Pain. 3rd ed. Edinburgh: Elsevier/Churchill Livingstone; 2013. pp. 93–94. [Google Scholar]
- Adams M, Freeman B, Morrison H, Nelson I, Dolan P. Mechanical initiation of intervertebral disc degeneration. Spine. 2000;25(13):1625–1636. doi: 10.1097/00007632-200007010-00005. [DOI] [PubMed] [Google Scholar]
- Adams M, Hutton WC. Prolapsed intervertebral disc. A hyper flexion injury 1981 Volvo Award in Basic Science. Spine. 1982;7(3):184–191. [PubMed] [Google Scholar]
- Alexander MJ. Biomechanical aspects of lumbar spine injuries in athletes: a review. Can J Appl Sport Sci. 1985;10(1):1–20. [PubMed] [Google Scholar]
- Boocock M, Reilly T, Linge K, Troup JDG, Reilly T, Watkins J, Borms J. Fine Measurement of Stature for Studying Spinal Loading. Kinanthropometry III. London: E and F N Spon; 1986. pp. 98–103. [Google Scholar]
- Clement D, Taunton J, Smart G, McNicol KL. A survey of overuse running injuries. Phys Sports Med. 1981;9:47–58. doi: 10.1080/00913847.1981.11711077. [DOI] [PubMed] [Google Scholar]
- Crewe H, Elliott B, Couanis G, Campbell A, Alderson J. The lumbar spine of the young cricket fast bowler: an MRI study. J Sci Med Sport. 2012;15(3):190–194. doi: 10.1016/j.jsams.2011.11.251. [DOI] [PubMed] [Google Scholar]
- Crock HV. Internal disc disruption. A challenge to disc prolapse fifty years on. Spine. 1986;11(6):650–653. [PubMed] [Google Scholar]
- Dabbs V, Dabbs L. Correlation between disc height narrowing and low-back pain Spine”. Spine. 1990;15(12):1366–1369. doi: 10.1097/00007632-199012000-00026. [DOI] [PubMed] [Google Scholar]
- d’Hemecourt P, Hresko MT. Spinal deformity in young athletes. Clin Sports Med. 2012;31(3):441–451. doi: 10.1016/j.csm.2012.03.013. [DOI] [PubMed] [Google Scholar]
- Dolan P, Earley M, Adams MA. Bending and compressive stresses acting on the lumbar spine during lifting activities. J Biomech. 1994;27(10):1237–1248. doi: 10.1016/0021-9290(94)90277-1. [DOI] [PubMed] [Google Scholar]
- Goldstein J, Berger P, Windler G, Jackson DW. Spine injuries in gymnasts and swimmers. An epidemiologic investigation. Am J Sports Med. 1991;19(5):463–468. doi: 10.1177/036354659101900507. [DOI] [PubMed] [Google Scholar]
- Holm S, Holm A, Ekstrom L, Karladani A, Hansson T. Experimental disc degeneration due to endplate injury. J Spinal Disord Tech. 2004;17(1):64–71. doi: 10.1097/00024720-200402000-00012. [DOI] [PubMed] [Google Scholar]
- Jones D, Tearse D, el-Khoury G, Kathol M, Brandser EA. Radiographic abnormalities of the lumbar spine in college football players. A comparative analysis. Am J Sports Med. 1999;27:335–338. doi: 10.1177/03635465990270031101. [DOI] [PubMed] [Google Scholar]
- Kazarian LE. Creep characteristics of the human spinal column. Orthop Clin North Am. 1975;6(1):3–18. [PubMed] [Google Scholar]
- Lundin O, Hellström M, Nilsson I, Swärd L. Back pain and radiological changes in the thoraco-lumbar spine of athletes. A long-term follow-up. Scand J Med Sci Sports. 2001;11(2):103–109. doi: 10.1034/j.1600-0838.2001.011002103.x. [DOI] [PubMed] [Google Scholar]
- Murtaugh K. Injury patterns among female field hockey players. Med Sci Sports Exerc. 2001;33:201–207. doi: 10.1097/00005768-200102000-00005. [DOI] [PubMed] [Google Scholar]
- Ogurkowska MB. Pathological changes in lumbar-sacral intervertebral discs in professional rowers. Biol Sport. 2007;24(4):375. [Google Scholar]
- Reilly T, Seaton A. Physiological strain unique to field hockey. J Sports Med Phys Fitness. 1990;30(2):142–146. [PubMed] [Google Scholar]
- Reilly T, Temple J. Lovesey E. Contemporary Ergonomics. London: Taylor & Francis; 1993. Some ergonomic consequences of playing field hockey; pp. 441–444. [Google Scholar]
- Rishiraj N, Taunton J, Niven B. Injury profile of elite under-21 age female field hockey players. J Sports Med Phys Fitness. 2009;49(1):71–77. [PubMed] [Google Scholar]
- Ruyssen-Witrand A, Gossec L, Kolta S, Dougados M, Roux C. Vertebral dimensions as risk factor of vertebral fracture in osteoporotic patients: a systematic literature review. Osteoporos Int. 2007;18:1271–1278. doi: 10.1007/s00198-007-0356-6. [DOI] [PubMed] [Google Scholar]
- Schmitt H, Dubljanin E, Schneider S, Schiltenwolf M. Radiographic changes in the lumbar spine in former elite athletes. Spine. 2004;29(22):2554–2559. doi: 10.1097/01.brs.0000145606.68189.69. [DOI] [PubMed] [Google Scholar]
- Smith L, Weiss E, Lehmkuhl LD. Brunnstrom’s Clinical Kinesiology. 5th ed. Philadelphia: F. A. Davis; 1996. p. 161169. [Google Scholar]
- Smith R, Loschner C. Biomechanics feedback for rowing. J Sports Sci. 2002;20(10):783–791. doi: 10.1080/026404102320675639. [DOI] [PubMed] [Google Scholar]
- Tertti M, Paajanen H, Kujala U, Alanen A, Salmi T, Kormano M. Disc degeneration in young gymnasts. A magnetic resonance imaging study. Am J Sports Med. 1990;18(2):206–208. doi: 10.1177/036354659001800216. [DOI] [PubMed] [Google Scholar]
- Videman T, Nurminen M, Troup JDG. Lumbar spinal pathology in cadaveric material in relation to history of back pain, occupation and physical loading. Spine. 1990;15:728–740. [PubMed] [Google Scholar]
- Videman T, Sarna S, Battié MC, Koskinen S, Gill K, Paananen H, Gibbons L. The long-term effect of physical loading and exercise life styles on back related sypmtoms, disability and spinal patology among men. Spine. 1995;20:699–709. doi: 10.1097/00007632-199503150-00011. [DOI] [PubMed] [Google Scholar]
- Wolfram U, Wilke H, Zysset PK. Damage accumulation in vertebral trabecular bone depends on loading mode and direction. J Biomech. 2011;44:1164–1169. doi: 10.1016/j.jbiomech.2011.01.018. [DOI] [PubMed] [Google Scholar]