

Abstract
Plagiocephaly is a common condition that affects infants. It can be broadly grouped into positional and non positional plagiocephaly Positional plagiocephaly frequently resolves without intervention. Non positional plagiocephaly resulting from craniosynostosis often requires surgical intervention. In this case report, we present a rare case of unilateral frontosphenoid craniosynostosis. We discuss the appropriate diagnostic workup, the available treatment options, and patient follow-up over time. Furthermore, we provide a detailed review of the literature discussing treatment options for aesthetic appearance as the child ages.
Keywords: Plagiocephaly, Frontosphenoid Craniosynostosis, Orbital Reconstruction
Introduction
Positional plagiocephaly is common in infants and typically affects the posterior skull, but non positional plagiocephaly is rare and can affect the anterior skull [1]. On the other hand, once non positional plagiocephaly is identified, classification of the type of plagiocephaly is important in order to determine the most effective clinical management. The two main types of non positional plagiocephaly are craniosynostosis and canal molding. Craniosynostosisis the premature closure of the fibrous sutures in an infants skull and frequently requires surgical intervention as the child ages where as canal molding usually spontaneously resolves without intervention [2]. The type of craniosynostosis most frequently reported in the literature as causing anterior non positional plagiocephaly is coronal craniosynostosis, however, 10 cases of frontosphenoid craniosynostosis have also been reported [3]. It is important to be aware of frontosphenoid craniosynostosis because it has erroneously been mistaken for coronal craniosynostosis in the literature and treatment therefore delayed [4]. Frontosphenoid craniosynostosis more commonly affects females than males 5:2 ratio, but the underlying cause for this gender difference is currently unknown [5]. Frontosphenoid craniosynostosis has been associated with unique allelic conditions such as achondroplasia, but can also occur sporadically [6]. In this report, we present a unique case of frontosphenoid craniosynostosis in a male, provide a detailed review of the literature, and discuss the appropriate management for this rare form of anterior non positional plagiocephaly.
Case
The patient was a two and a half year-old male at time of presentation that had been meeting developmental milestones. He had an uneventful delivery at 34 weeks via C-section due to a breech-presenting twin. It was noted at time of delivery that he had an abnormally shaped forehead. As he aged, he lost the ability to close his right eye due to protrusion of the orbital bones and was referred by his pediatrician for an emergent inpatient pediatric neurosurgical consultation. At time of admission, a CT scan was obtained and revealed right frontosphenoid craniosynostosis (Figure 1). Surgical repair was deemed necessary and a four-tiered approach was utilized with a bilateral frontal craniotomy, supraorbital rim osteotomy, supraorbital advancement, and orbital frontal cranial reconstruction. The frontal, bicoronal flap was advanced anteriorly in the subperiosteal plane until it reached the supraorbital rim (Figure 2). The patient tolerated surgery well and remained hemodynamically stable. The patient had an uneventful postoperative course and was discharged 5 days post-operatively with no headaches, emesis, or fever.
Figure 1.
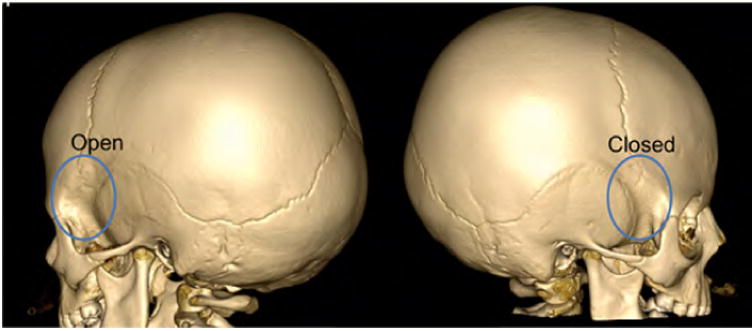
Preoperative CT. Three-dimensional CT reconstruction of the head showing (A) patent left frontosphenoid suture and (B) fusion of right frontosphenoid suture. Patent coronal sutures can be seen on both sides.
Figure 2.
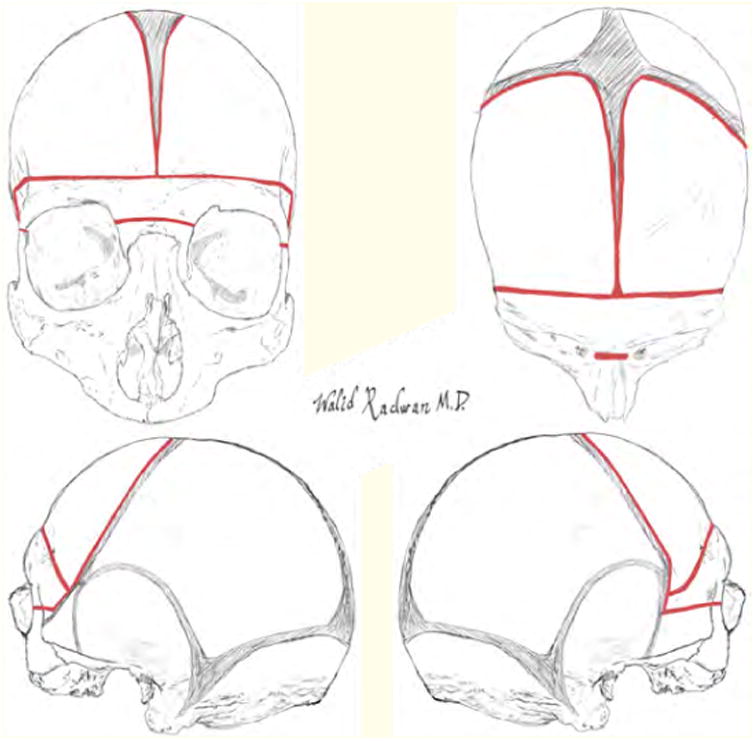
Craniotomy and orbital rim osteotomies for frontosphenoid craniosynostosis repair. Note the prematurely fused frontosphenoid suture on the right side.
At his 1-year follow-up, he was meeting developmental milestones appropriately and head proportions appeared symmetrical. He was still having some difficulty closing his right eye at that visit. During winter of 2014, a CT was performed showing skull changes due to growth. An area of the right orbital roof had bony uncovering. During a follow up exam in Spring 2015, it was noted that his right orbit seemed to be descending, the right cheekbone was less prominent, and his forehead was more pinched limiting his ability to be properly fitted for sport helmets. Despite this limitation, he was doing well in school and sports. It was decided after consulting with plastic surgery to perform craniofacial contour remodeling using a polyether ether ketone (PEEK) implant once bone maturity is achieved.
Discussion
Anterior plagiocephaly causes unilateral frontal flattening and recession of the supraorbital rim. The most likely etiology for anterior plagiocephaly is fusion of the unilateral coronal suture, but fusion of the frontosphenoidal suture should not be overlooked [7]. CT imaging is the gold standard for diagnosing craniosynostosis [8]. In conjunction with pertinent history and physical findings, the diagnosis can be made early thereby facilitating rapid treatment. A skull-molding helmet has been tried by some groups, however, most patients failed and required surgical treatment [9]. Careful evaluation of sutures is necessary to differentiate frontosphenoid craniosynostosis from the more common coronal craniosynostosis [10]. In this case, afronto-orbital advancement as pioneered by Tessier in 1969 was performed and consisted of a bilateral frontal craniotomy, supraorbital rim osteotomy, supraorbital advancement, and orbital frontal cranial reconstruction [11]. The patient tolerated the surgery well and recovered uneventfully.
One of the key features of frontosphenoid craniosynostosis is dysmorphology. The sphenoid bone is more likely to be affected than either the temporal or zygomatic bone [3]. The premature fusion causes disturbed growth of the orbit increasing its protrusion while causing frontal flattening overall [12]. Addressing the aesthetic appearance of the misshaped skull should be a priority for surgical planning [13]. It is important to recognize that anterior plagiocephaly may be caused by frontosphenoid craniosynostosis as this pathology, given its rarity, may be overlooked. The limitations of the repair are primarily due to persistent skull growth. Titanium and mesh implants around the orbit do not expand as the skull grows therefore necessitating follow-up procedures. Ideally, if the patient is doing well clinically, the second repair should be delayed until bone maturity has been reached. Patient-specific PEEK implants have been found to be the most effective for aesthetic reconstruction once bone maturity is reached [14].
Conclusion
Two types of non-positional plagiocephaly are commonly reported in the literature: craniosynostosis and canal molding. Herein we described a unique case of frontosphenoid craniosynostosis. This type of plagiocephaly can be differentiated from the more common type of coronal craniosynostosis using CT imaging. Once identified, early surgical treatment using the approach pioneered by Tessier is mandated. As the child ages, further surgeries are often needed to enhance aesthetic appearance. PEEK implants placed around the orbit after bone maturity has been established have been shown to be the most effective.
Bibliography
- 1.Bot G, et al. Frontosphenoid synostosis: an unusual cause of anterior plagiocephaly. Journal of Craniofacial Surgery. 2015;26.1:174–175. doi: 10.1097/SCS.0000000000001183. [DOI] [PubMed] [Google Scholar]
- 2.Pickrell BB, et al. Isolated Unilateral Frontosphenoidal Craniosynostosis: A Rare Cause of Anterior Plagiocephaly. Journal of Craniofacial Surgery. 2015;26.6:1944–1946. doi: 10.1097/SCS.0000000000001950. [DOI] [PubMed] [Google Scholar]
- 3.Sakamoto Y, et al. Involvement of the sphenosquamosal suture for unilateral coronal synostosis. Journal of Craniofacial Surgery. 2012;23.5:1267–1269. doi: 10.1097/SCS.0b013e3182519a97. [DOI] [PubMed] [Google Scholar]
- 4.Rogers GF, et al. Unilateral fusion of the frontosphenoidal suture: a rare cause of synostotic frontal plagiocephaly. Plastic and Reconstructive Surgery. 2002;110.4:1011–1021. doi: 10.1097/01.PRS.0000021308.37931.18. [DOI] [PubMed] [Google Scholar]
- 5.Sauerhammer TM, et al. Isolated frontosphenoidal synostosis: a rare cause of synostotic frontal plagiocephaly. Journal of Neurosurgery Pediatrics. 2014;13.5:553–558. doi: 10.3171/2014.1.PEDS1378. [DOI] [PubMed] [Google Scholar]
- 6.Hubbard BA, et al. Unilateral frontosphenoidal craniosynostosis with achondroplasia: a case report. Cleft Palate-Craniofacial Journal. 2011;48.5:631–635. doi: 10.1597/09-266. [DOI] [PubMed] [Google Scholar]
- 7.Ben Nsir A, et al. Plagiocephaly due to Frontosphenoidal Suture Synostosis: Report of 2 Cases and Literature Review. Pediatric Neurosurgery. 2016;51.4:204–209. doi: 10.1159/000444194. [DOI] [PubMed] [Google Scholar]
- 8.Magge KT, et al. Incidental findings on preoperative computed tomography for nonsyndromic single suture craniosynostosis. Journal of Craniofacial Surgery. 2014;25.4:1327–1330. doi: 10.1097/SCS.0000000000000797. [DOI] [PubMed] [Google Scholar]
- 9.Shen WM, et al. Plagiocephaly resulted from frontosphenoidal synostosis and squamosal suture synostosis: a report of five cases. Zhonghua Zheng Xing Wai Ke Za Zhi. 2012;28.6:407–410. [PubMed] [Google Scholar]
- 10.Marucci DD, et al. Unilateral isolated frontosphenoidal craniosynostosis causing frontal plagiocephaly. Journal of Plastic Reconstructive and Aesthetic Surgery. 2009;62.8:e255–e258. doi: 10.1016/j.bjps.2007.12.016. [DOI] [PubMed] [Google Scholar]
- 11.Tessier P. Total facial osteotomy. Crouzon's syndrome, Apert's syndrome: oxycephaly, scaphocephaly, turricephaly. Annales de Chirurgie Plastique Esthétique. 1967;12.4:273–286. [PubMed] [Google Scholar]
- 12.Nagasao T, et al. A biomechanical study on the effect of premature fusion of the frontosphenoidal suture on orbit asymmetry in unilateral coronal synostosis. Cleft Palate-Craniofacial Journal. 2010;47.1:82–91. doi: 10.1597/08-164.1. [DOI] [PubMed] [Google Scholar]
- 13.Showalter BW, et al. Influence of frontosphenoidal suture synostosis on skull dysmorphology in unicoronal suture synostosis. Journal of Craniofacial Surgery. 2012;23.6:1709–1712. doi: 10.1097/SCS.0b013e31826beecc. [DOI] [PubMed] [Google Scholar]
- 14.Rammos CK, et al. Patient-specific polyetheretherketone implants for repair of craniofacial defects. Journal of Craniofacial Surgery. 2015;26.3:631–633. doi: 10.1097/SCS.0000000000001413. [DOI] [PubMed] [Google Scholar]