

Abstract
Objectives
We aimed to investigate whether SDMA- symmetric dimethylarginine -the symmetrical stereoisomer of ADMA- might be a marker of left ventricular function in AMI.
Background
Asymmetric dimethylarginine (ADMA) has been implicated in the prognosis after acute myocardial infarction (AMI) and heart failure (HF).
Methods
Cross sectional prospective study from 487 consecutive patients hospitalized <24 hours after AMI. Patients with HF on admission were excluded. Serum levels of ADMA, SDMA and L-arginine were determined using HPLC. Glomerular filtration rate (eGFR) was estimated based on creatinine levels. Outcomes were in-hospital severe HF, as defined by Killip class >2, and death.
Results
Patients were analysed based on SDMA tertiles. Sex, diabetes, dyslipidemia, and prior MI were similar for all tertiles. In contrast, age and hypertension increased across the tertiles (p<0.001). From the first to the last tertile, GRACE risk score was elevated while LVEF and eGFR was reduced. The rate of severe HF and death were gradually increased across the SDMA tertiles (from 0.6% to 7.4%, p = 0.006 and from 0.6% to 5.0%, p = 0.034, respectively). Backward logistic multivariate analysis showed that SDMA was an independent estimate of developing severe HF, even when adjusted for confounding (OR(95%CI): 8.2(3.0–22.5), p<0.001). Further, SDMA was associated with mortality, even after adjustment for GRACE risk score (OR(95%CI): 4.56(1.34–15.52), p = 0.015).
Conclusions
Our study showed for the first time that SDMA is associated with hospital outcomes, through altered LVEF and may have biological activity beyond renal function.
Introduction
Coronary artery disease (CAD) including acute myocardial infarction (MI) is the most frequent cause of altered Left Ventricular Ejection Fraction (LVEF) and Heart Failure (HF). Conversely, HF is a frequent complication of acute MI and significantly worsens the prognosis of patients with CAD. Given the strong association of acute MI and HF, it is important to understand the underlying mechanisms of HF in patients with acute MI.
Impaired nitric oxide (NO) bioavailability is involved in the pathogenesis and progression of CAD. Moreover, in patients with chronic HF, accumulation of methylated arginine metabolites has been associated with disease progression [1]. Asymmetric dimethylarginine (ADMA), as a methylated product of L-arginine, may compete with L-arginine as the substrate for the nitric oxide synthases (NOS) or inhibit NOS phosphorylation and therefore decrease NO production [2]. Over the last decades, it has emerged as a novel cardiovascular risk factor in the setting of endothelial dysfunction including type 2 diabetes, hypertension, CAD, HF and end stage renal disease [3,4].Moreover, in recent works we have suggested the specific link between ADMA and HDL levels [5].
Much less is known about the biological role of an alternative methylation product of L-arginine, namely symmetric dimethylarginine (SDMA). Although structural isomer of ADMA, SDMA is not a direct competitive inhibitor of NOS, but could interfere with L-arginine uptake into the cells via the y+ class of cationic amino acid transporters (CAT) [6]. SDMA is mainly cleared by the renal route and its circulating levels are elevated in chronic kidney disease. SDMA has been initially considered as a powerful marker of renal function [7]. Recent lines of evidence showed that SDMA could not be simply yet another uremic toxin, but also a mediator with pathophysiological relevance as an early diagnostic for detrimental cardiovascular outcomes [8,9]. Notably, in patients with acute MI, elevated SDMA levels are strong predictors of late cardiac events, beyond chronic kidney disease [10]. Moreover, in patients with chronic systolic HF, SDMA levels were associated with the presence of LV dysfunction, suggesting a potential role of SDMA in the pathophysiological of HF [1].
In a subgroup analysis from a large prospective study in acute MI patients [5], we evaluated the relationship between circulating levels of dimethylarginines, in particular SDMA, with renal function and LVEF.
Methods
Study subjects
All the consecutive patients aged >18 years and hospitalized <24 hours after symptom onset for acute MI in the Coronary Care Unit of Dijon University Hospital from 1st January 2011 to 30th June 2012 were included. Patients with relevant co-morbidities (infection, autoimmune disorders and cancers) or admitted with heart failure were excluded from the study. MI was defined by an increase in serum troponin Ic [> upper limit of the hospital normal (ULN) range: 0.1 μg/L] associated with symptoms of ischemia and/or typical ECG signs. ST-segment elevation MI (STEMI) was defined as chest pain lasting for ≥20min with typical ECG changes including ≥1mV ST segment elevation in two or more limb leads or ≥2mV in two or more contiguous precordial leads. The study was approved by the Consultative Committee of Protection of Persons in Biomedical Research of Burgundy and conducted in accordance with Declaration of Helsinki. All subjects gave their written consent to participate in the study.
Data collection
Data on demographics, risk factors [history of hypertension, diabetes, dyslipidemia, body mass index (BMI)], chronic treatments and prior MI were prospectively collected. Chronic kidney disease was defined based on the presence of kidney damage or glomerular filtration rate (eGFR<60 mL/min per 1.73 m2) for 3 months, irrespective of cause[11].
History of HF was defined as previous hospital admission with diagnosis of HF or documented clinical symptoms of HF. Killip class was classified as follow: Killip I: no clinical signs of HF; Killip class II: rales or crackles < 50% lung field; Killip class III frank acute pulmonary oedema; Killip class IV: cardiogenic shock. In-hospital severe HF was defined by Killip class >II. The Global Registry of Acute Coronary Event (GRACE) risk score was calculated for each patient with admission variables including age, heart rate, serum creatinine, systolic blood pressure, Killip class, cardiac arrest, ST-segment deviation, and cardiac markers (http://www.outcomes-umassmed.org/grace/). Echocardiography was performed at 2±1 days with the Simpson method to assess LVEF. Altered LVEF was defined as LVEF ≤ 40% for more clinical relevance.
Biological data
Blood samples were drawn on admission (Median time from symptom onset to blood sampling: 16 (8–20) hours), as previously described [5]. Creatinine levels were measured on a Vitros 950 analyzer (Ortho Clinical Diagnostics) and the glomerular filtration rate (eGFR) was estimated on the Chronic Kidney Disease (CKD) EPI formula [12]. Normal or weakly impaired renal function, moderate and severe renal dysfunction were defined as eGFR > 60 mL/min, 30–60 mL/min and < 30 mL/min respectively. Plasma troponin Ic peak was assessed by sampling every eight hours during the first two days after admission (Dimension Vista Intelligent Lab System, Siemens).
Dimethylarginines and L-arginine analysis
Samples were allowed to clot at room temperature for 30 minutes and centrifuged at 2500 rpm for 10 minutes at 4°C. The serum was kept frozen at -80°C until analysis. As described in detail previously [5], L-arginine, ADMA, and SDMA, were measured by high performance liquid chromatography (HPLC) [13,14].
Statistical analysis
Continuous data are presented as median [IQR (inter quartile range)] or mean ± SD, as appropriate or as proportion. For continuous variables, a Kolmogorov-Smirnov analysis was performed to test for normality. Non normal variables were log-transformed before entering into the analysis (i.e. SDMA, NtproBNP, ADMA and Larginine). To compare the data between 2 groups, the Mann-Whitney Rank Sum test or student’s t test was performed and a 1-way ANOVA or by Kruskal-Wallis 1-way analysis, as appropriate, was performed for 3 groups comparisons. Dichotomous variables were compared by Chi square tests.
Multiple linear regression analysis was performed with eGFR as a dependent variable with age and SDMA as covariates.
No data were available on the relationship between SDMA levels and HF in patients with acute MI. Hence, we have empirically calculated our sample size, based on the number of patients to include for an expected number of 20 events (severe heart failure) chosen as the minimal number of events for adequate statistical performance and yielding a study population at ≈ 500 subjects with MI. Logistic regression analysis was further performed to estimate the variables associated with the risk of developing severe HF during the hospital stay. Only variables that were significant by univariate analyses (p<0.01) were entered into the multivariate models, with an exclusion cut-off at 2%. The first model included LVEF, eGFR, and Nt-proBNP. A second model included LVEF, eGFR and SDMA (instead of Nt-proBNP). ROC curve analysis was further performed for each model and AUC were used to compare the discriminative value for the 2 models.
Another model of backward logistic regression analysis was built to assess the association between SDMA and in-hospital mortality. NtproBNP and GRACE risk score were included as covariates, in addition to SDMA, with the same exclusion cutoff. All the analyses were performed using the SPSS 12.0 software package (IBM Inc, USA).
Results
Baseline clinical and biological variables
The characteristics of the 487 patients classified by SDMA tertiles are shown in Table 1. Sex, diabetes, dyslipidemia, and prior MI were similar for all tertiles. In contrast, mean age and proportion of patients with hypertension increased across the tertiles (p<0.001). Anterior location and hemodynamic parameters on admission did not differ significantly. From the first to the last tertile, GRACE risk score was elevated and LVEF was reduced. Rate of PCI was decreased across SDMA tertiles.
Table 1. Presenting characteristics (n(%), median (IQR) or mean ± SD).
| SDMA tertiles Median (IQR)range(min-max), μmol/L | ||||
|---|---|---|---|---|
| T10.35(0.31–0.39)0.15–0.42n = 163 | T20.50(0.46–0.54)0.42–0.59n = 163 | T30.76(0.66–0.96)0.59–2.48n = 161 | p | |
| Risk factors | ||||
| Female | 33(20%) | 37(23%) | 42(26%) | 0.474 |
| Age, years | 59±12 | 62±13 | 70±15 | <0.001 |
| Diabetes | 29 (18%) | 28 (17%) | 38 (24%) | 0.289 |
| Hypertension | 69 (42%) | 77 (47%) | 100 (62%) | 0.001 |
| Dyslipidemia | 70 (44%) | 71 (44%) | 67 (42%) | 0.889 |
| Current Smoker | 64 (39%) | 56 (34%) | 35 (22%) | 0.003 |
| Prior MI | 17 (10%) | 19 (12%) | 26 (16%) | 0.249 |
| Chronic kidney disease | 0 (0%) | 2 (1%) | 14 (9%) | <0.001 |
| Clinical data | ||||
| STEMI | 103 (63%) | 82 (50%) | 79 (49%) | 0.018 |
| Anterior wall location | 60 (37%) | 66 (41%) | 53 (33%) | 0.347 |
| Heart rate, beats/min | 75 [64–85] | 74 [64–83] | 75 [64–88] | 0.842 |
| SBP, mmHg | 134 [122–160] | 140 [117–160] | 139 [116–161] | 0.961 |
| DBP, mmHg | 84 [70–96] | 80 [70–90] | 79 [69–90] | 0.026 |
| GRACE risk score | 127±26 | 132±30 | 147±33 | <0.001 |
| LVEF, % | 55 [50–60] | 58 [50–65] | 50 [45–60] | 0.010 |
| Chronic treatments | ||||
| Aspirin | 24 (15%) | 27 (17%) | 42 (26%) | 0.020 |
| Betablocker | 26 (16%) | 40 (25%) | 49 (30%) | 0.009 |
| Fibrate | 9 (6%) | 6 (4%) | 2 (1%) | 0.107 |
| ACE inhibitor | 21 (13%) | 31 (19%) | 30 (19%) | 0.259 |
| Statin | 35 (22%) | 37 (23%) | 41 (26%) | 0.684 |
| Acute revascularization | ||||
| PCI | 124 (76%) | 109 (67%) | 99 (63%) | 0.017 |
| Thrombolysis | 39 (24%) | 43 (26%) | 29 (18%) | 0.172 |
| CABG | 6 (4%) | 15 (9%) | 11 (7%) | 0.130 |
MI: Myocardial Infarction; CV: Cardiovascular; ACE: angiotensin-converting enzyme; CAD: coronary artery disease; CABG: Coronary Arterial Bypass Graft; SBP: Systolic blood pressure; DBP: Diastolic blood pressure; HR: heart rate; LVEF: left ventricular ejection fraction; PCI: Percutaneous Coronary Intervention; SBP: systolic blood pressure; SDMA: Symmetric dimethylarginine; STEMI: ST segment elevation MI.
Biological data are presented in Table 2. Lipid parameters vary significantly among the 3 groups. A dramatic increase in Nt-proBNP level was observed in the last SDMA tertile (p<0.001). ADMA, L-arginine and homocysteine levels gradually increased across the tertiles.
Table 2. Biological data (Median (IQR) or mean ± SD).
| SDMA tertiles Median (IQR)range(min-max), μmol/L | ||||
|---|---|---|---|---|
| T10.35(0.31–0.39)0.15–0.42N = 163 | T20.50(0.46–0.54)0.42–0.59N = 163 | T30.76(0.66–0.96) 0.59–2.48N = 161 | p | |
| eGFR, ml/min/1.73 m2 | 84±19 | 80±21 | 62±26 | <0.001 |
| Nt-proBNP, pg/ml | 252 [79–959] | 459 [167–1396] | 1343 [322–5249] | <0.001 |
| Homocysteine, μmol/L | 11 [9–14] | 12 [9–16] | 14 [11–21] | <0.001 |
| ADMA, μmol/L | 0.53 [0.38–0.82] | 0.57 [0.44–0.94] | 0.70 [0.50–1.13] | <0.001 |
| L-arginine, μmol/L | 86 [70–115] | 96 [72–127] | 96 [74–128] | 0.022 |
| LDL-cholest, mg/dl | 131±38 | 130±41 | 118±45 | 0.006 |
| HDL-cholest, mg/dl | 39 [30–47] | 40 [33–52] | 43 [33–54] | 0.002 |
| Total-cholest, mg/dl | 201±44 | 202±44 | 188±51 | 0.013 |
| Triglycerides, mg/dl | 121 [89–177] | 127 [084–176] | 103 [76–151] | 0.043 |
| CRP, mg/L | 4.6 [3.0–10.8] | 5.0 [3.0–13.5] | 5.6 [3.0–15.0] | 0.347 |
| Troponin Ic, peak, μg/L | 20.0 [6.4–41.0] | 19.0 [4.0–41.0] | 12.7 [2.9–41.0] | 0.163 |
ADMA: Asymmetric dimethylarginine; CRP: C-reactive protein; eGFR: Estimated Glomerular filtration rate; HDL-C: high density lipoprotein; LDL-C: low density lipoprotein; NT-proBNP: N-terminal Pro-Brain Natriuretic Peptide. SDMA: Symmetric dimethylarginine.
SDMA and renal function
Rate of patients with chronic renal failure was almost 10 fold higher in the last tertile than lower tertiles (p<0.001) (Table 1). Moreover, eGFR markedly decreased across the SDMA tertiles from 84 to 62 ml/min/1.73 m2 (Table 2). Given the potential for renal clearance to serve as an important determinant of plasma levels of dimethylated products of L-arginine, in particular for SDMA levels, patients were classified according to their eGFR. SDMA levels showed a strong and gradual relationship with renal filtration rate (Fig 1).
Fig 1. Symmetric dimethylarginine concentrations according to estimated Glomerular Filtration Rate (p value for comparison between the tertiles).

Patients with severely altered renal dysfunction (eGFR <30 ml/min/1.73 m2) had markedly higher SDMA levels than patients with normal renal function (≈ +113%, 0.98 vs. 0.46 μmol/L). In contrast, no significant difference was seen for ADMA (0.55(0.43–0.80), 0.58(0.43–1.01), 0.61(0.43–0.89) μmol/L, p = 0.860) or L-arginine levels (86(56–114), 87(69–117), 91(72–125) μmol/L, p = 0.104) in the 3 groups. A significant correlation between between SDMA and eGFR was found (r = -0.499, p<0.001); although less strong, this correlation was also reported in STEMI patients (r = -0.335, p< 0.001). Moreover, by multivariate linear regression analysis, SDMA remained an independent predictor of eGFR (B = -18.0 ± 2.0, p<0.001) even after adjustment on age (B = -0.8 ±0.1, p<0001).
SDMA and LVEF
A significant correlation between between SDMA and LVEF was found (r = -0.124, p<0.009); although less strong, this correlation was also reported in STEMI patients (p = 0.011). When patients were classified according to LVEF alteration (≤ 40%) (Fig 2), SDMA was significantly elevated in patients with altered LVEF (0.54 (0.39–0.89) vs. 0.50 (0.39–0.64) μmol/L, p = 0.04).
Fig 2. Symmetric dimethylarginine concentrations according to Left Ventricular Ejection Fraction (p value for comparison between the 2 groups).
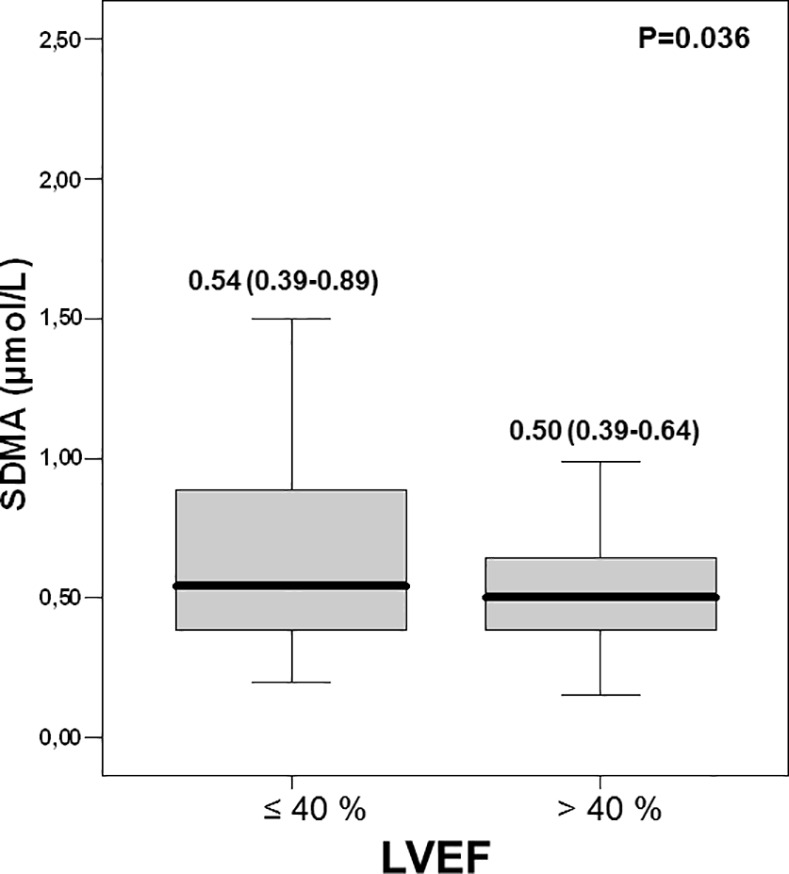
In contrast, there was no difference for the two groups for ADMA and L-arginine levels (0.54 (0.43–0.74) vs.0.56 (0.42–0.87); p = 0.41 and (89 (75–117) vs. 89 (70vs. 121) μmol/L; p = 0.99, respectively).
SDMA and in-hospital outcomes
Median length of hospital stay was 4(3–4) days. During hospital stay, 19 patients developed severe HF and 12 patients died. The rate of severe HF was similar in STEMI and NSTEMI (5% vs 4%, p = 0.645, respectively). Fig 3 shows the distribution of hospital events across the SDMA tertiles.
Fig 3. Cardiovascular outcomes according to Symmetric dimethylarginine tertiles values (p value for comparison between the tertiles).
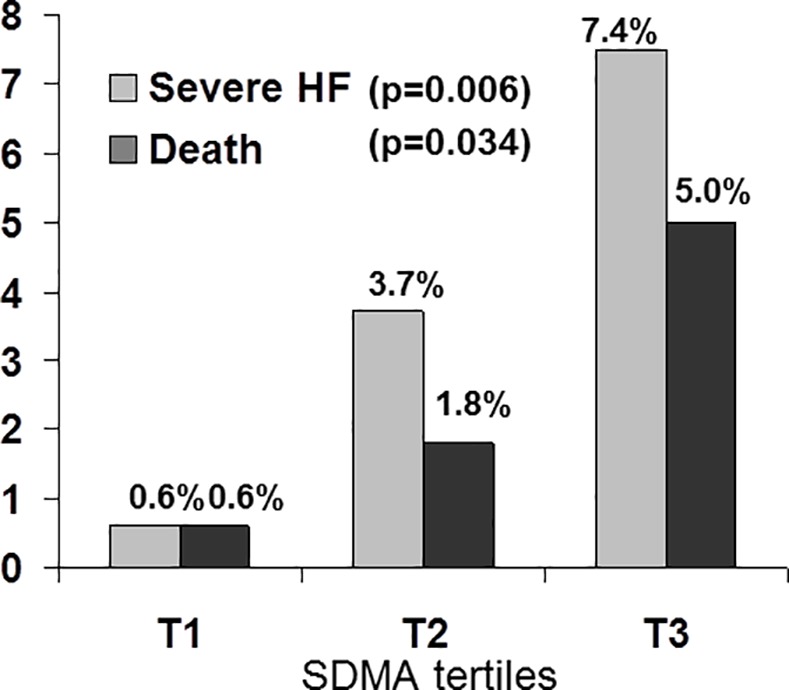
Markedly more patients had HF in the higher tertiles of SDMA, with a rate of severe HF more than 10 fold higher in the last tertile when compared to the lowest tertile (p = 0.006). Similarly, there was a gradual increase in mortality across the SDMA tertiles, from 0.6% to 5.0% (p = 0.034). Given the strong relationship between SDMA and LVEF, we further tested whether SDMA could estimate the later development of HF during hospital stay. The first model included LVEF, eGFR, and Nt-proBNP. By backward logistic multivariate analysis, Nt-proBNPlevels, in addition to altered LVEF, was an independent estimate of developing severe hospital HF (OR(95%CI): 1.7(1.2–2.3), p = 0.002 and 10.7(3.8–30.4), p<0.001). ROC curve analysis for the model provided an AUC at 0.860 (SE: 0.047), p<0.001. A second model showed that SDMA -as covariate instead of Nt-proBNP- remained an independent predictor of severe HF beyond altered LVEF (OR(95%CI): 8.2(3.0–22.5), p<0.001, and 16.8(5.8–48.9), p<0.001), respectively). The corresponding AUC was 0.863 (SE: 0.042), p<0.001). The comparison of the ROC curves of the 2 models gave similar discrimination performance (p = 0.951), further suggesting the value of SDMA as biomarker for the prediction of HF. Sensitivity analyses, based on the location of MI (anterior vs other or unknown location) were further performed. SDMA remained an estimate of HF development in patients with anterior wall location (n = 179(37%)) (OR(95%CI): 26.36(0.93–747,30), p = 0.055) or without anterior wall location (OR(95%CI): 5.61(2.03–15.53), p = 0.001).
Moreover, SDMA was associated with excess risk of hospital mortality, even after adjustment for GRACE risk score (OR(95%CI): 4.56(1.34–15.52), p = 0.015, and 1.03(1.00–1.05), p = 0.013), respectively).
Discussion
ADMA has been shown to competitively inhibit the binding of L-arginine to the substrate-binding moiety of NOS and is a strong predictor of CV events in selected population [4]. Moreover, we have recently suggested a link between ADMA and HDL-C levels, which may be due to the modulation of eNOS activity [5]. Less attention has been paid to its structural isomer, namely SDMA, as a biomarker in prospective clinical studies. To the best of our knowledge, this is the first study addressing the role of SDMA in high risk patients. Our large cross sectional prospective study showed that SDMA is a powerful factor associated with alteration of LVEF, beyond its relationship with renal function. Moreover, our findings showed that the circulating levels of this dimethylarginine on admission were predictive for worse outcome, characterized by the development of HF.
SDMA and renal function
Elimination of SDMA occurs primarily by renal excretion and not surprisingly, we found its levels particularly elevated in patients with acute MI, characterized by frequent impaired renal function. The levels of SDMA were markedly elevated when compared with SDMA levels in healthy individuals from a large community-based cohort using a stable isotope dilution assay [15] [median (IQR), our study: 0.52(0.40–0.71) vs. 0.37(0.32–0.43) μmol/L in Schwedhelm et al]. Our findings on the strong relationship of SDMA serum levels with eGFR are in agreement with both animal experiments and human studies, where SDMA has emerged as an endogenous marker of renal function. In particular, evidence has accumulated from > 2100 patients with CKD or CAD[7], with a correlation coefficient between SDMA and creatinine levels at 0.75 (p<0.001).
SDMA and outcomes
Although SDMA was usually thought to be functionally inactive, recent works highlighted its predictive value for CV events[16]. However, these works were limited to specific subgroups of CAD patients. Our works extent these findings across the whole spectrum of acute MI. Although SDMA lacks competitive NOS inhibitory activity, all methylated arginine metabolites are thought to inhibit NO synthesis indirectly as L-arginine analogues via blockade of cationic arginine transport–a process shown to be impaired in the setting of HF [17,18]. Moreover, presence of elevated levels SDMA inside the HDL particles may also participate to the noxious vascular effects of the lipoprotein in CKD [9]. Our work is the first to highlight the strong and independent relationship between SDMA, but not ADMA, and altered LV function in acute MI. Moreover, we found that elevated levels of SDMA are strongly associated with the development of HF during hospitalisation, beyond traditional factors including renal impairment. A direct relationship between accumulation of methylated arginine metabolites, including SDMA and altered LV diastolic function has been reported in patients with chronic systolic HF [1]. Moreover, there is strong in vivo and in vitro evidence for a marked depression of L-arginine transport [17] and endothelial dysfunction in patients with chronic HF. Plasma ADMA levels were also reported elevated in patients with chronic HF, and correlated significantly with New York Heart Association (NYHA) functional class and exercise capacity [19]. In addition, elevated plasma ADMA levels were associated with increased risk of mortality and adverse cardiovascular outcome in patients with chronic HF [20,21]. After an acute ischemic stroke, short term survival decreased significantly with ascending tertiles of SDMA levels at admission [22].
Our findings also found an independent association between SDMA and short term mortality (OR: 4.55(1.34–15.52)), further suggesting a pathophysiological role for this marker. A recent study also showed that SDMA was an independent predictor of all cause and cardiovascular mortality in a large multiethnic population-based cohort [23].
Limitations
This work, however, suffers the usual limitations of observational, non-randomized studies, and therefore determines association, rather than causal relationships. Other potential factors may influence the prognosis in the setting of acute MI, including delays for invasive strategy, location of chronic total occlusion or multivessel disease[24–26]. These factors were not available in our study and may potentially alter the strength of our findings. However, no data are currently available on the relationship between SDMA and such confounding. Although the origin of circulating dimethylarginines levels remains unclear, endothelial cells may be a major contributor [8]. The involvement of cardiac EC, in conjunction with the pulmonary endothelial cells, is of critical importance in the development of HF because this represents the largest single source of endothelial mediators[27]. In experimental post-MI setting, EC dysfunction has been shown to contribute to the development of HF [28] and impaired prognosis[29]. Dimethylarginines levels in HF have been suggested as a pathophysiologic link between oxygen radical load and impaired vasodilator capacity [29]. Preincubation with SDMA has been shown to stimulate ROS production in isolated monocytes by stimulating Ca2+ entry via the SOCs [30] and was associated with an increase of reactive oxygen species in culture endothelial cells [31]. None of these effects were found with ADMA. However, further studies are needed to better understand the underlying biological effects of SDMA.
Conclusion
Our large prospective study is the first to date showing an association between elevated SDMA and worse hospital outcomes including major surrogate markers in acute MI, such as altered renal function. Our works suggests that such dimethylarginines may probably exert biological activity by other pathways than NOS activity inhibition and at least partly beyond renal function.
Acknowledgments
The authors thank Mr. P. Bastable for English review of the manuscript, Florence Bichat, Aline Chagnon, Françoise Bechet, for technical assistance and Maud Maza for statistical analysis.
Data Availability
The data underlying our findings can be found in the body of the manuscript.
Funding Statement
This work was supported by the University Hospital of Dijon, the Association de Cardiologie de Bourgogne, and by grants from the Agence Régionale de Santé (ARS) de Bourgogne, French Ministry of Research, Institut National de la Santé et de la Recherche Médicale (INSERM), Fédération Française de Cardiologie, Société Française de Cardiologie and from the Regional Council of Burgundy.
References
- 1.Wilson Tang WH, Tong W, Shrestha K, Wang Z, Levison BS, Delfraino B, et al. Differential effects of arginine methylation on diastolic dysfunction and disease progression in patients with chronic systolic heart failure. Eur Heart J. 2008;29:2506–2513 10.1093/eurheartj/ehn360 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Teerlink T, Luo Z, Palm F, Wilcox CS. Cellular ADMA: Regulation and action. Pharmacol Res. 2009;60:448–460 10.1016/j.phrs.2009.08.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ronden RA, Houben AJ, Teerlink T, Bakker JA, Bierau J, Stehouwer CD, et al. Reduced renal plasma clearance does not explain increased plasma asymmetric dimethylarginine in hypertensive subjects with mild to moderate renal insufficiency. Am J Physiol. 2012;303:F149–156 [DOI] [PubMed] [Google Scholar]
- 4.Zeller M, Korandji C, Guilland JC, Sicard P, Vergely C, Lorgis L, et al. Impact of asymmetric dimethylarginine on mortality after acute myocardial infarction. Arterioscl Thromb Vasc Biol. 2008;28:954–960 10.1161/ATVBAHA.108.162768 [DOI] [PubMed] [Google Scholar]
- 5.Lorin J, Guilland JC, Korandji C, Touzery C, Bichat F, Chagnon A, et al. High levels of asymmetric dimethylarginine are strongly associated with low HDL in patients with acute myocardial infarction. PloS One. 2013;8:e64796 10.1371/journal.pone.0064796 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Closs EI, Basha FZ, Habermeier A, Förstermann U. Interference of L-arginine analogues with L-arginine transport mediated by the y+ carrier hCAT-2B. Nitric oxide.1997;1:65–73 10.1006/niox.1996.0106 [DOI] [PubMed] [Google Scholar]
- 7.Kielstein JT, Salpeter SR, Bode-Boeger SM, Cooke JP, Fliser D. Symmetric dimethylarginine (SDMA) as endogenous marker of renal function—a meta-analysis. Nephrol Dial Transpl. 2006;21:2446–2451 [DOI] [PubMed] [Google Scholar]
- 8.Schwedhelm E, Boger RH. The role of asymmetric and symmetric dimethylarginines in renal disease. Nat Rev Nephrol. 2011;7:275–285 10.1038/nrneph.2011.31 [DOI] [PubMed] [Google Scholar]
- 9.Speer T, Rohrer L, Blyszczuk P, Shroff R, Kuschnerus K, Kränkel N, et al. Abnormal high-density lipoprotein induces endothelial dysfunction via activation of Toll-like receptor-2. Immunity. 2013;38:754–768 10.1016/j.immuni.2013.02.009 [DOI] [PubMed] [Google Scholar]
- 10.Cavalca V, Veglia F, Squellerio I, De Metrio M, Rubino M, Porro B, et al. Circulating levels of dimethylarginines, chronic kidney disease and long-term clinical outcome in non-st-elevation myocardial infarction. PloS One. 2012;7:e48499 10.1371/journal.pone.0048499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.K/DOQI. Clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am J Kidney Dis.2002;39:S1–266. [PubMed] [Google Scholar]
- 12.Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ivanova M, Artusi C, Boffa GM, Zaninotto M, Plebani M. HPLC determination of plasma dimethylarginines: method validation and preliminary clinical application. Clin Chim Acta.2010;411:1632–1636 10.1016/j.cca.2010.06.001 [DOI] [PubMed] [Google Scholar]
- 14.Korandji C, Zeller M, Guilland JC, Vergely C, Sicard P, Duvillard L, et al. Asymmetric dimethylarginine (ADMA) and hyperhomocysteinemia in patients with acute myocardial infarction. Clin Biochem. 2007;40:66–72. 10.1016/j.clinbiochem.2006.08.004 [DOI] [PubMed] [Google Scholar]
- 15.Schwedhelm E, Xanthakis V, Maas R, Sullivan LM, Atzler D, Lüneburg N, et al. Plasma symmetric dimethylarginine reference limits from the Framingham offspring cohort. Clin Chem Lab Med. 2011;49:1907–1910 10.1515/CCLM.2011.679 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Meinitzer A, Kielstein JT, Pilz S, Drechsler C, Ritz E, Boehm BO, et al. Symmetrical and asymmetrical dimethylarginine as predictors for mortality in patients referred for coronary angiography: The Ludwigshafen Risk and Cardiovascular Health study. Clin Chem. 2011;57:112–121 10.1373/clinchem.2010.150854 [DOI] [PubMed] [Google Scholar]
- 17.Kaye DM, Parnell MM, Ahlers BA. Reduced myocardial and systemic L-arginine uptake in heart failure. Circ Res. 2002;91:1198–1203 [DOI] [PubMed] [Google Scholar]
- 18.Tojo A, Welch WJ, Bremer V, Kimoto M, Kimura K, Omata M, et al. Colocalization of demethylating enzymes and NOS and functional effects of methylarginines in rat kidney. Kidney Int. 1997;52:1593–1601 [DOI] [PubMed] [Google Scholar]
- 19.Usui M, Matsuoka H, Miyazaki H, Ueda S, Okuda S, Imaizumi T. Increased endogenous nitric oxide synthase inhibitor in patients with congestive heart failure. Life Sci. 1998;62:2425–2430 [DOI] [PubMed] [Google Scholar]
- 20.Duckelmann C, Mittermayer F, Haider DG, Altenberger J, Eichinger J, Wolzt M. Asymmetric dimethylarginine enhances cardiovascular risk prediction in patients with chronic heart failure. Arterioscl Thromb Vasc Biol. 2007;27:2037–2042 10.1161/ATVBAHA.107.147595 [DOI] [PubMed] [Google Scholar]
- 21.Zairis MN, Patsourakos NG, Tsiaousis GZ, Theodossis Georgilas A, Melidonis A, Makrygiannis SS, et al. Plasma asymmetric dimethylarginine and mortality in patients with acute decompensation of chronic heart failure. Heart. 2012;98:860–864 10.1136/heartjnl-2011-301372 [DOI] [PubMed] [Google Scholar]
- 22.Luneburg N, von Holten RA, Topper RF, Schwedhelm E, Maas R, Böger RH. Symmetric dimethylarginine is a marker of detrimental outcome in the acute phase after ischaemic stroke: Role of renal function. Clin Sci. 2012;122:105–111 10.1042/CS20110013 [DOI] [PubMed] [Google Scholar]
- 23.Gore MO, Luneburg N, Schwedhelm E, Ayers CR, Anderssohn M, Khera A, et al. Symmetrical dimethylarginine predicts mortality in the general population: observations from the dallas heart study. Arterioscl Thromb Vasc Biol.2013;33(11): 2682–8. 10.1161/ATVBAHA.113.301219 [DOI] [PubMed] [Google Scholar]
- 24.Hoebers LP, Elias J, van Dongen IM, Ouweneel DM, Claessen BE, Piek JJ, et al. The impact of the location of a chronic total occlusion in a non-infarct-related artery on long-term mortality in ST-elevation myocardial infarction patients. EuroIntervention. 2016;12:423–430 10.4244/EIJV12I4A75 [DOI] [PubMed] [Google Scholar]
- 25.Moretti C, D'Ascenzo F, Quadri G, Omedè P, Montefusco A, Taha S, et al. Management of multivessel coronary disease in STEMI patients: a systematic review and meta-analysis. Int J Cardiol. 2015;179:552–557 10.1016/j.ijcard.2014.10.035 [DOI] [PubMed] [Google Scholar]
- 26.Russo JJ, Goodman SG, Cantor WJ, Tan MK, Borgundvaag B, Fitchett D, et al. TRANSFER-AMI Investigators. Efficacy and safety of a routine early invasive strategy in relation to time from symptom onset to fibrinolysis (a subgroup analysis of TRANSFER-AMI). Am J Cardiol. 2015;115:1005–12. 10.1016/j.amjcard.2015.01.533 [DOI] [PubMed] [Google Scholar]
- 27.Brutsaert DL. Cardiac endothelial-myocardial signaling: its role in cardiac growth, contractile performance, and rhythmicity. Physiol Rev. 2003;83:59–115 10.1152/physrev.00017.2002 [DOI] [PubMed] [Google Scholar]
- 28.Qi XL, Stewart DJ, Gosselin H, Azad A, Picard P, Andries L, et al. Improvement of endocardial and vascular endothelial function on myocardial performance by captopril treatment in postinfarct rat hearts. Circulation. 1999;100:1338–1345 [DOI] [PubMed] [Google Scholar]
- 29.von Haehling S, Bode-Boger SM, Martens-Lobenhoffer J, Rauchhaus M, Schefold JC, Genth-Zotz S, et al. Elevated levels of asymmetric dimethylarginine in chronic heart failure: a pathophysiologic link between oxygen radical load and impaired vasodilator capacity and the therapeutic effect of allopurinol. Clin Pharmacol Ther. 2010;88:506–512 10.1038/clpt.2010.116 [DOI] [PubMed] [Google Scholar]
- 30.Schepers E, Glorieux G, Dhondt A, Leybaert L, Vanholder R. Role of symmetric dimethylarginine in vascular damage by increasing ROS via store-operated calcium influx in monocytes. Nephrol Dial Transpl. 2009;24:1429–1435 [DOI] [PubMed] [Google Scholar]
- 31.Bode-Böger SM, Scalera F, Kielstein JT, Martens-Lobenhoffer J, Breithardt G, Fobker M, et al. Symmetrical dimethylarginine: a new combined parameter for renal function and extent of coronary artery disease. J Am Soc Nephrol. 2006;17:1128–1134 10.1681/ASN.2005101119 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data underlying our findings can be found in the body of the manuscript.