

Introduction
Aortic coarctation (CoA) constitutes the fifth most common congenital heart defect (1 in 2500 live births). This lesion comprises 5–8% of congenital heart disease and has variable severity and mode of presentation.1 Critical coarctation in newborns usually presents with severe narrowing of the upper thoracic aorta below the isthmus and adjacent to the arterial duct, and is dependent on duct patency for survival. Rapid deterioration of the patient usually results from spontaneous closure of the patent arterial duct (PDA). This deterioration is in part due to reduced renal perfusion resulting in fluid and acid retention causing heart failure and metabolic acidosis. This may be alleviated by the administration of intravenous prostaglandin, with temporary improvement of distal aortic blood flow, and overall condition. The treatment of choice is surgical resection with the ‘extended end-to-end’ technique.
We present a case of a severely ill newborn with complex coarctation, multiorgan failure, disseminated intravascular coagulation and oedema, who was treated with emergency stenting on the tenth day of life. This was followed by surgical stent removal and repair of the arch on the 29th day of life. We followed the strategy of minimally invasive interventional bridging of a borderline patient with regard to the experience of stenting of native coarctations in older patients, or complex recurrent stenosis of previously surgically treated children.2
Patient
We report a 9 day old female baby who presented acutely in the neonatal period with profound acidosis, heart failure, severe metabolic acidosis and disseminated intravascular coagulation. She was ventilated and echocardiography revealed CoA with a hypoplastic arch as well as partial anomalous pulmonary venous drainage and a small ventricular septal defect. This diagnosis was made in a regional centre in a country (Malta) without ready access to a paediatric cardiac surgical centre.
The infant was started on prostaglandin with no benefit, was ventilated and the acid base deficit addressed. A bare metal coronary artery stent (Biotronik Pro Kinetic 3.5/13 mm) was implanted across the CoA site (figures 1–4) via a right femoral artery cut-down which was repaired postoperatively.
Figure 1.
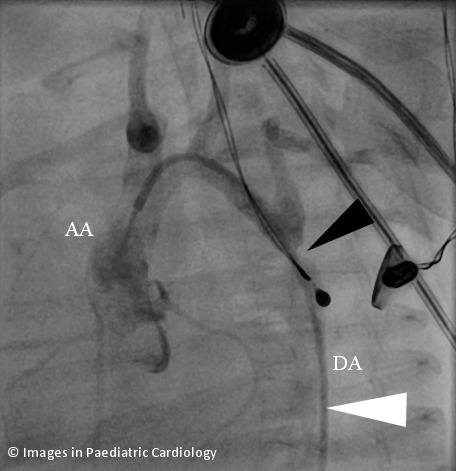
Angiogram prior to stenting, retrograde passage of catheter (white arrow) up the descending aorta, across the coarctation site (black arrow). AA=ascending aorta, DA=descending aorta. Note several ECG leads crossing field.
Figure 4.
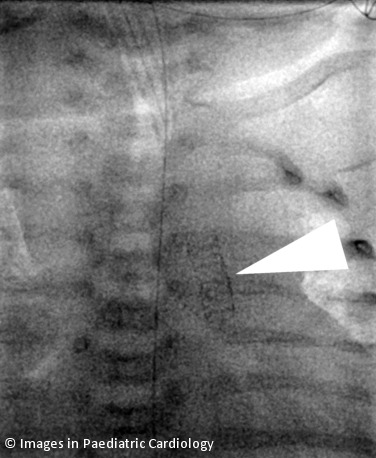
Stent in descending aorta.
Figure 2.
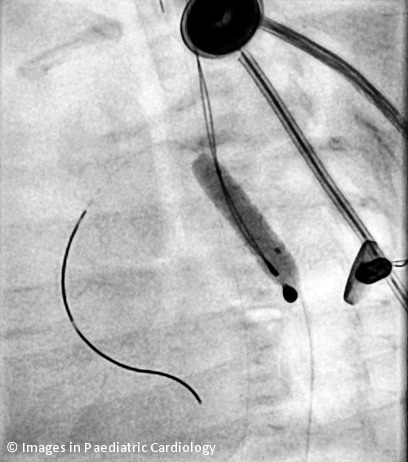
Coronary stent being inflated by balloon (premounted stent) across the coarctation site.
Figure 3.
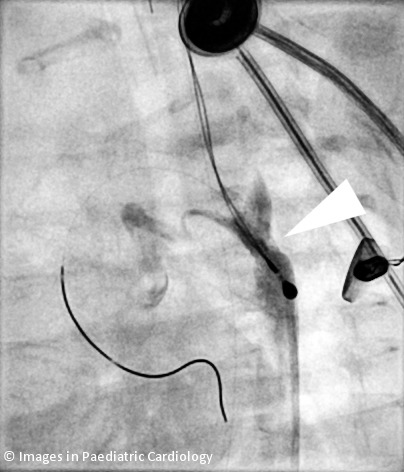
Postinflation angiogram.
The acidosis and intravascular coagulation rapidly improved and the child was a few hours later extubated. She was electively transferred to London six days later. Surgery was carried out through a median sternotomy because of the arch hypoplasia. The stent was removed without any complications and corrective surgery was carried out, with excision of the coarctation site and augmentation of the aorta. The patient rapidly developed rapidly progressive recoarctation and this was uneventfully ballooned a few weeks after the initial operation, with good result.
Discussion
This strategy has been previously utilized not only for neonates and young infants,3 but also for premature infants in whom surgical repair may not be technically feasible.4 Although palliative balloon angioplasty does work, it is less reliable and recoarctation can recur very early. The axillary artery is bigger than the femoral but because of the abnormal and hypoplastic arch in this case, the femoral approach was used.
In selected cases and under special circumstances, stenting a neonatal coarctation is a reasonable option. As the stent was likely to be in place for a short time and because of the unknown safety of Drug Eluting Stents (DES) in infants, we elected to use a simple bare metal coronary stent. Early removal of the stent and repair is recommended to avoid having the stent firmly embedded in the aortic wall. The midline approach is essential when there is concomitant arch hypoplasia and it is surgically more feasible to treat the arch hypoplasia at this age due to the extensive experience obtained with the Norwood procedure for hypoplastic left heart syndrome.
References
- 1.Kenny D, Hijazi ZM. Coarctation of the aorta: from fetal life to adulthood. Cardiol J. 2011; 18:487–95. [DOI] [PubMed] [Google Scholar]
- 2.Holzer RJ, Chisolm JL, Hill SL, Cheatham JP. Stenting complex aortic arch obstructions. Catheter Cardiovasc Interv. 2008;71:375–82. [DOI] [PubMed] [Google Scholar]
- 3.Sreeram I, Sreeram N, Bennink G. Palliative stent implantation for coarctation in neonates and young infants. Ann Pediatr Card. 2012;5:145–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Radtke WA, Waller BR, Hebra A, Bradley SM. Palliative stent implantation for aortic coarctation in premature infants weighing <1500 g. Am J Cardiol. 2002;90:1409–12. [DOI] [PubMed] [Google Scholar]