

Abstract
Purpose:
An increasing number of comparative studies are conducted on the stigmatization of persons with mental illness, in particular with regard to regional and diachronic variation. So far, there have been no studies comparing stigmatization of persons with mental illness in two different regions of India. Therefore, we examined the differences in perception of stigma attached to mental illnesses in Kolkata and Chennai, with regard to cultural and geographical differences to better understand the roots and origins of this issue.
Materials and Methods:
Explorative surveys in the context of public attitudes toward people with mental disorders were conducted among conveniently selected members of the general population in Chennai (n = 166) and Kolkata (n = 158) with identical methodology. Link's perceived devaluation-discrimination measure was used. The samples were matched for age, gender, and education.
Results:
The calculated sum score indicated that respondents from Kolkata had a higher level of perceived discrimination toward persons with mental illness than respondents from Chennai (P = 0.043). Furthermore, regression analysis revealed that lower perceived stigma was associated with stronger religious devotion (P = 0.049) and higher educational attainment (P = 0.001) in both cities.
Discussion:
The results showed that perceived stigma was higher in Kolkata than in Chennai. The correlation of higher stigma with lower education was in line with the previous research, and interestingly, it was found that higher stigma correlated with weaker religious devotion. Further studies exploring a wider variety of factors may provide us with a better understanding of the roots of perceived stigma in India.
Key words: Education, mental illness, perceived stigma, religion
INTRODUCTION
Stigma in the context of mental disorders is a field that has been broadly studied in the past and is characterized by rejection, blame, or exclusion as a result of adverse social judgment about a person with a mental health disorder.[1] Discrimination and devaluation of persons with mental illness may have an effect on many aspects of their lives, including housing, employment, access to services, and interpersonal relationships. Furthermore, in terms of health-care utilization, individuals that worry about discrimination because of public awareness toward their mental illness may suffer from delayed diagnosis, personal distress, and impeded recovery.[2,3,4]
While stigma on its own can be regarded as a direct social judgment about a person, perceived stigma concerns the expected reaction of others and is therefore relevant for people with psychological disorders, who want to be open about their disorders. This is especially with regard to how the general population influences, how the public reacts to those suffering from mental illnesses, and what their attitudes toward them are.[5] Recently, researchers conducted comparative studies of mental illness stigma both over time and in different nations, societies, and cultures.[5,6] While a range of studies have been conducted in developing countries,[3,7,8] none have so far intended to compare the levels of stigmatization between different regions on the subcontinent of India.
With a rapidly growing population, it can only be expected that the number of individuals suffering from mental illnesses in India will increase as well. There is an estimated 5.82–7.35% prevalence of mental disorders that today accounts for roughly 70 million people.[9] In addition, India has a rather low median of 0.2 psychiatrists per 100,000 people compared with the global median of 1.2.[9] These figures do well in highlighting the importance of efficiency and effectiveness when diagnosing mental illnesses and offering adequate treatment. Stigmatization of persons suffering from mental illnesses, as with many other developing countries with rooted traditions, is a major issue since it may hinder the process of bridging the mental health-care gap.[3]
This study aims to compare the public perception of persons with mental illness in two very distinct cities in India. The first city is Kolkata, located in the eastern state of West Bengal, with the other city being Chennai, located in the southern state of Tamil Nadu. The two cities are separated by roughly 1700 km and are culturally different in many ways, ranging from their language to their literacy rates, and their religious composition.[10] Therefore, we aim to analyze whether any difference in sociodemographic characteristics has an influence on the level of perceived stigma.
MATERIALS AND METHODS
Sample
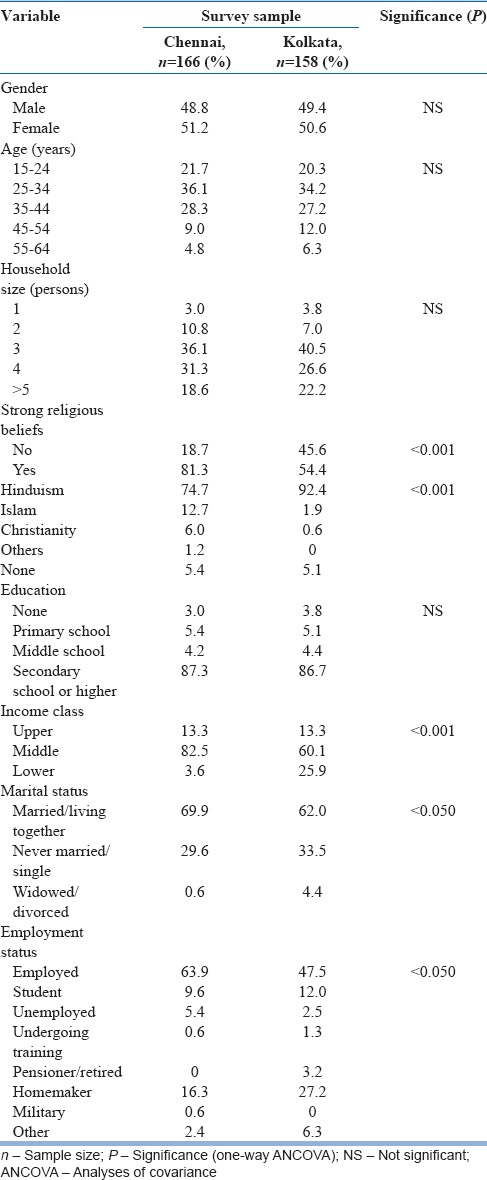
Data collection in Chennai and Kolkata was carried out in April and May 2014. The assistance of a market research firm “Panoramix™” in the data collection process ensured accurate and consistent completion of the questionnaires in both cities. Since we included participants who were registered with the firm, it resulted in a convenience sample. Our sampling method did not involve a probability-based selection method. Individuals were asked to redo any questionnaire that was either inaccurate or incomplete, thus yielding a completion rate of 100%. Kolkata was the first city in which participants were recruited, following which participants from Chennai were recruited to match the gender, age, and educational attainment of Kolkata. Participants were neither younger than 17 nor older than 64 years of age. The number of respondents in Chennai was 166 while the number of respondents in Kolkata was 158, with an overall sample size of 324. The detailed demographic characteristics of our sample are presented in Table 1.
Table 1.
Sociodemographic characteristics of survey sample
Interview
The interview-based questionnaire conducted by a psychologist, used to assess respondent's perceived stigma was Link's perceived discrimination and devaluation scale (PDDS).[11] Relevant sociodemographic information was gathered and assessed such as gender, age, religion, household size, family size, income level, educational attainment, marital status, and household size.
As the questionnaire was initially created within the context of Western societies, the wording had to be changed in certain cases so as to be understood better by the local population in both cities.[12] This involved adjusting terminology relating to religion, spirituality, and educational attainment.
Translation procedure
Furthermore, the original questionnaire was translated into the local Indian languages by the market research firm using a back-translation method. The interview was administered using a fully structured interview.
Perceived stigma
Perceived stigma was assessed using data drawn from the established Link's PDDS including 12 items.[11] For these questions, the respondents had to indicate their opinion on whether most Indians would agree or disagree with statements regarding former psychiatric or mentally ill patients. Their opinion was indicated on a 5-point Likert scale ranging from “definitely true” to “definitely not true,” and the content of the statements was with regard to several factors such as intelligence, relationships, and whether they should be taken seriously.
Statistical analyses
Statistical analyses were performed using the program IBM SPSS Statistics for Mac OSX, Version 21.0 (Armonk, NY: IBM Corp). To analyze any difference in the sociodemographic characteristics between the two cities, a one-way analysis of variance (ANOVA) was performed. This ANOVA was done to compare the two samples and rule out possible confounding variables such as age, gender, education, household size, income class, religion, and strength of religious beliefs. In this case, the possible confounding factors formed the dependent list while the two cities became the factor.
A sum score was calculated by averaging the responses from all the participants for the questions related to perceived stigma. Six of the items were reversed to calculate this score. This calculation results in a score from one to five, representative of the five possible responses to each question. A score of one would indicate a low level of perceived stigma while a score of five would indicate a high level of perceived stigma. Multiple linear regression was calculated to determine the influence of the sociodemographic influences on the calculated sum score of the perceived discrimination scale. Gender, cities, educational school attainment, strength of religious beliefs, income class, marital status, and employment status were entered as categorical variables and age and household size as continuous variables.
A multivariate analysis of variance was then performed to confirm these influencing factors as well as identify differences and similarities between the two samples with regard to perceived stigma at the single item level. This was done by having the 12 questions of the PDDS as the independent variables, the two cities as the dependent variables, and the sociodemographic variables including age, gender, education, household size, income class, religion, and strength of religious beliefs as the covariates. For the statistical analyses, the five-point scale was reduced to three points, with “strongly agree” and “agree” as well as “strongly disagree” and “disagree” being merged. Detailed descriptive analyses were then performed on the significant items to control the direction of associations with higher perceived stigma.
The level of significance was set at P < 0.05.
RESULTS
Table 1 displays the sociodemographic characteristics and differences between Chennai and Kolkata. Since the samples were matched for age, gender, and educational attainment, there were no significant differences between the two cities for these demographics. Furthermore, there were no significant differences in household size. Significant differences were, however, found for the different religions (P < 0.001), reported strength of religious beliefs (P < 0.001), income class (P < 0.001), employment status (P < 0.05), and marital status (P < 0.05).
As can be seen in Table 2, a multilinear regression was calculated to determine the effect of each of the demographic variables on the level of perceived stigma, represented by the sum score. It is evident from the table that there was no significance for gender, age, household size, income class, marital status, or employment status. It is evident, however, that there was a significant effect caused by city (B = 0.072, β =0.121, P = 0.043), with Kolkata showing a higher level of perceived stigma, as well as for educational attainment (B = −0.166, β = −0.197, P = 0.001), where a higher level of educational attainment was associated with a lower level of perceived stigma, and finally for strength of religious devotion (B = 0.148, β =0.116, P = 0.049), where stronger religious beliefs were associated with lower levels of perceived stigma.
Table 2.
Multiple linear regression showing the influences of the demographic variables with mental illness on the perceived discrimination and devaluation scale sum score
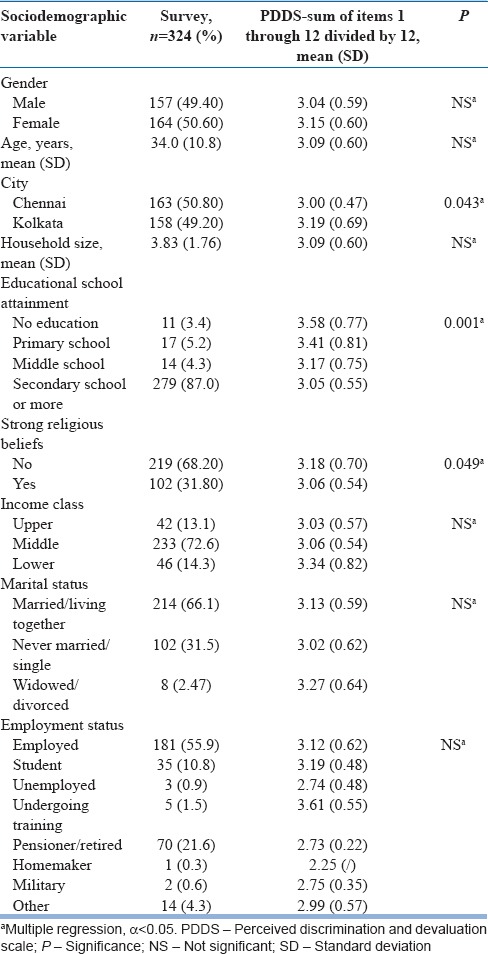
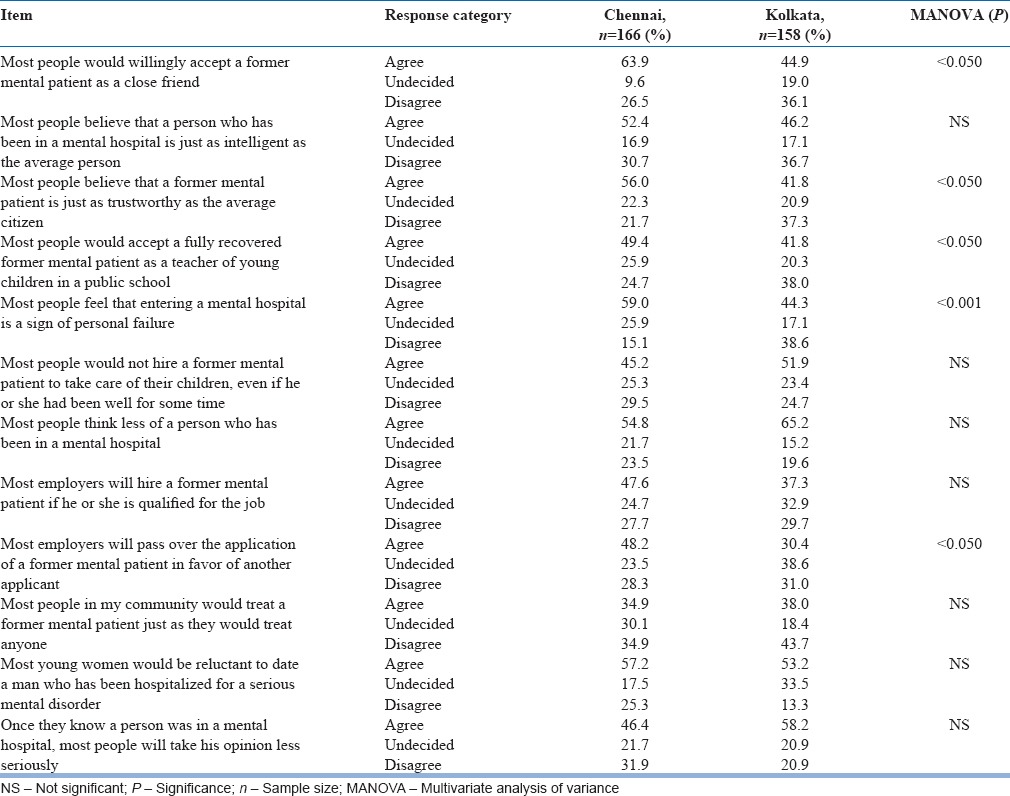
Table 3 shows a summary of the participants' responses from each city, along with the significant values that were calculated using multivariate analysis. Overall, it was found that higher levels of perceived stigma were correlated with being from Kolkata (P < 0.001). Out of the five items intended to measure differences between the two cities, three were particularly significant in revealing higher levels of perceived stigma for Kolkata than Chennai. These included believing that most people would accept a former mental patient as a close friend (item 1, P < 0.050), former mental patients are just as trustworthy as the average citizen (item 3, P < 0.050), and finally, most people would accept a fully recovered mental patient as a teacher of young children in a public school (item 4, P < 0.50). It was only the two items regarding people feeling that entering a mental hospital was a sign of personal failure (item 5, P < 0.001) and believing that employers would pass over the application of a mental patient in favor of another applicant (item 9, P < 0.050), for which respondents from Chennai showed significant perceived discrimination and devaluation of persons with mental illness. There were no significant differences for the other items of the PDDS.
Table 3.
Devaluation and discrimination of mental patients as perceived by respondents from Chennai and Kolkata
DISCUSSION
While the first clear observation was that respondents from Kolkata were associated with a significantly higher level of perceived stigmatization of persons with mental illness than respondents from Chennai, it is very important to note the factors that had a key influence on these levels of stigma. Lower levels of educational attainment were associated with higher levels in perceived stigma while stronger religious devotion was associated with lower levels of perceived stigma in both cities. The level of educational attainment was a demographic variable that was controlled for, so there was no significant difference between the two cities to explain the difference in perceived stigma. It is interesting to note, however, that a lower level of educational attainment was associated with higher levels of perceived stigma when both cities were taken into account. This is in line with previous research which indicated that lower literacy rates result in increased difficulty with accessing information about mental illnesses and treatment plans, for example, mental health literacy, while also increasing the level of stigma experienced.[13,14]
While the level of educational attainment provides a possible explanation for the level of perceived stigmatization of persons with mental illness in both cities, religion is a factor that seems to play a role not only with the overall level of perceived stigma in both cities but also with the differences in stigma between the cities. Although there was a significant difference of reported religious attainment from respondents of both cities, this did not seem to influence the amount of perceived stigmatization. This finding is in contrast with studies that reported that stigma would differ across different religions. This has been shown in a study[15] comparing the health beliefs of elderly Christians, Hindus, and Muslims. The study found that people of these different religions varied in their likelihood to seek professional help or that of a religious healer. Furthermore, Hindus were nearly twice as likely to be embarrassed or ashamed about suffering from a mental illness. Interestingly, rather than the different religions, it was, in fact, the reported strength of an individual's religious beliefs that stood out as an influencing factor concerning the level of perceived stigma. It has been reported in a previous study that individuals with stronger religious beliefs would display higher levels of stigma, for instance, with regard to the stigma of HIV/AIDS in Puerto Rico.[16] This suggests that religious beliefs are intertwined with ideas of health, illness and service provision, and an individual's attitudes and perceptions. Furthermore, the study suggested that religious beliefs can be seen as cultural factors that influence or promote stigma; an example being an illness such as HIV/AIDS being interpreted as the repentance of sinful behaviors and thus as a way of returning to God. As evidenced from our data, however, stronger religious beliefs were associated with lower perceived stigma. Again, difference in concept between stigma and perceived stigma has to be taken into account. While the previously mentioned study looked directly at the stigma regarding illness, our study looks at how individuals perceive the stigma of others in their society. This may raise the question of whether people of stronger religious beliefs hold a more idealistic view of their society. While the actual stigma could well be high, the individuals who we surveyed from both cities with stronger religious beliefs held the view that there was a lower stigma in their society. It is of interest to note the results of a 2012 study looking at attitudes toward psychotherapy with regard to religion and ethnicity.[17] When comparing Jewish Whites to non-Jewish Whites and Black American individuals from the New York area of the United States, it was found that the Jewish people were more confident in a therapist's ability to help, more tolerant of stigma associated with mental health help-seeking, and were rated higher on interpersonal openness. Furthermore, the pattern of stronger religious beliefs associated with lower perceived stigma as seen in this study could be explained by the way that people who hold beliefs in moralistic, punitive, and knowing Gods generally show an increased impartiality toward others with similar beliefs, regardless of their religion.[18] It must be said, however, that most studies comparing stigmatization of mental illness with religious devotion in Europe and Africa found that they had no significant relationship with one another.[19,20,21,22]
Limitations
There were several factors that may have limited our study. First, it is clear that to gain a more accurate reading of a society, a larger sample size may prove beneficial. Furthermore, including more cities in different regions of the country may provide a wider scope for comparison and understanding. On that note, it would also be interesting if similar studies were conducted in other low- and middle-income countries as well as developed countries to provide a helpful comparison of differing cultures, societies, and norms. While age, gender, and educational attainment were the possible confounding factors controlled for in our study, it is not possible to rule out other factors such as urban/rural differences, or familiarity with mental illnesses, that may have caused a bias. Similarly, it would also be helpful in future studies to look at a wider variety of possible influencing factors that may have had a significant impact on the level of stigma.
CONCLUSION
To summarize, this study was conducted with participants from the Indian cities of Chennai and Kolkata, with the goal of investigating the perceived stigma among the local population. Many demographic variables were considered to gauge any influencing factor on high or low levels of perceived stigma, respectively. While Kolkata was associated with a higher level of perceived stigma than Chennai, the two cities did not show any significant difference when it came to the influencing factors, and it was found that in both cities, stronger religious devotion was associated with a lower level of perceived stigma while lower literacy was associated with a higher level of perceived stigma. While assumptions can be made as to why these factors had such an effect on the level of perceived stigma, it would be interesting to investigate whether similar patterns would emerge with a larger sample size, looking at a larger variety of possible causal factors. Another interesting direction for future studies may be an examination of whether these patterns emerge on a national level also.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Weiss MG, Ramakrishna J. Stigma interventions and research for international health. Lancet. 2006;367:536–8. doi: 10.1016/S0140-6736(06)68189-0. [DOI] [PubMed] [Google Scholar]
- 2.Fung KM, Tsang HW, Chan F. Self-stigma, stages of change and psychosocial treatment adherence among Chinese people with schizophrenia: A path analysis. Soc Psychiatry Psychiatr Epidemiol. 2010;45:561–8. doi: 10.1007/s00127-009-0098-1. [DOI] [PubMed] [Google Scholar]
- 3.Kermode M, Bowen K, Arole S, Pathare S, Jorm AF. Attitudes to people with mental disorders: A mental health literacy survey in a rural area of Maharashtra, India. Soc Psychiatry Psychiatr Epidemiol. 2009;44:1087–96. doi: 10.1007/s00127-009-0031-7. [DOI] [PubMed] [Google Scholar]
- 4.Rüsch N, Heekeren K, Theodoridou A, Dvorsky D, Müller M, Paust T, et al. Attitudes towards help-seeking and stigma among young people at risk for psychosis. Psychiatry Res. 2013;210:1313–5. doi: 10.1016/j.psychres.2013.08.028. [DOI] [PubMed] [Google Scholar]
- 5.Angermeyer MC, Matschinger H, Carta MG, Schomerus G. Changes in the perception of mental illness stigma in Germany over the last two decades. Eur Psychiatry. 2014;29:390–5. doi: 10.1016/j.eurpsy.2013.10.004. [DOI] [PubMed] [Google Scholar]
- 6.Deshpande SN, Kaur J, Zaky M, Loza N. Mental health legislation in Egypt and India. Ethical and practical aspects. Int J Ment Health. 2013;42:91–105. [Google Scholar]
- 7.Sadik S, Bradley M, Al-Hasoon S, Jenkins R. Public perception of mental health in Iraq. Int J Ment Health Syst. 2010;4:26. doi: 10.1186/1752-4458-4-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.St Louis KO, Roberts PM. Public attitudes toward mental illness in Africa and North America. Afr J Psychiatry (Johannesbg) 2013;16:123–33. doi: 10.4314/ajpsy.v16i2.16. [DOI] [PubMed] [Google Scholar]
- 9.Sinha SK, Kaur J. National mental health programme: Manpower development scheme of eleventh five-year plan. Indian J Psychiatry. 2011;53:261–5. doi: 10.4103/0019-5545.86821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Government of India. Census of India 2011. State Lit. 2011. [Last accessed on 2016 May 02]. pp. 3–4. Available from: http://www.censusindia.gov.in/2011.prov.results/data_files/india/Final_PPT_2011_chapter 6.pdf .
- 11.Link BG, Cullen FT, Struening E, Shrout P, Dohrenwend BP. A modified labeling theory approach in the area of mental disorders. An empirical assessment. Am Sociol Rev. 1989;54:100–23. [Google Scholar]
- 12.Sartorius N, Kuyken W, Orley J. Quality of Life Assessment: International Perspectives. Berlin: Springer; 1994. Translation of health status instruments; pp. 2–8. [Google Scholar]
- 13.Lincoln AK, Arford T, Doran MV, Guyer M, Hopper K. A preliminary examination of the meaning and effect of limited literacy in the lives of people with serious mental illness. J Community Psychol. 2015;43:315–20. [Google Scholar]
- 14.Girma E, Tesfaye M, Froeschl G, Möller-Leimkühler AM, Müller N, Dehning S. Public stigma against people with mental illness in the Gilgel Gibe Field Research Center (GGFRC) in Southwest Ethiopia. PLoS One. 2013;8:e82116. doi: 10.1371/journal.pone.0082116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Eisenberg D, Downs MF, Golberstein E, Zivin K. Stigma and help seeking for mental health among college students. Med Care Res Rev. 2009;66:522–41. doi: 10.1177/1077558709335173. [DOI] [PubMed] [Google Scholar]
- 16.Varas-Díaz N, Neilands TB, Malavé Rivera S, Betancourt E. Religion and HIV/AIDS stigma: Implications for health professionals in Puerto Rico. Glob Public Health. 2010;5:295–312. doi: 10.1080/17441690903436581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Midlarsky E, Pirutinsky S, Cohen F. Religion, ethnicity, and attitudes toward psychotherapy. J Relig Health. 2012;51:498–506. doi: 10.1007/s10943-012-9599-4. [DOI] [PubMed] [Google Scholar]
- 18.Purzycki BG, Apicella C, Atkinson QD, Cohen E, McNamara RA, Willard AK, et al. Moralistic gods, supernatural punishment and the expansion of human sociality. Nature. 2016;530:327–30. doi: 10.1038/nature16980. [DOI] [PubMed] [Google Scholar]
- 19.Adewuya AO, Makanjuola RO. Social distance towards people with mental illness in southwestern Nigeria. Aust N Z J Psychiatry. 2008;42:389–95. doi: 10.1080/00048670801961115. [DOI] [PubMed] [Google Scholar]
- 20.Alonso J, Buron A, Rojas-Farreras S, de Graaf R, Haro JM, de Girolamo G, et al. Perceived stigma among individuals with common mental disorders. J Affect Disord. 2009;118:180–6. doi: 10.1016/j.jad.2009.02.006. [DOI] [PubMed] [Google Scholar]
- 21.Audu IA, Idris SH, Olisah VO, Sheikh TL. Stigmatization of people with mental illness among inhabitants of a rural community in Northern Nigeria. Int J Soc Psychiatry. 2013;59:55–60. doi: 10.1177/0020764011423180. [DOI] [PubMed] [Google Scholar]
- 22.Girma E, Möller-Leimkühler AM, Müller N, Dehning S, Froeschl G, Tesfaye M. Public stigma against family members of people with mental illness: Findings from the Gilgel Gibe Field Research Center (GGFRC), Southwest Ethiopia. BMC Int Health Hum Rights. 2014;14:2. doi: 10.1186/1472-698X-14-2. [DOI] [PMC free article] [PubMed] [Google Scholar]