

Abstract
Introduction:
A situation analysis report on elderly in India shows that the literacy rate for persons aged above 60 is 36%. Using HMSE and its modification in the first phase of a two phase study to estimate the prevalence of dementia in such a population must be read with caution as these tests are literacy dependent. We conducted a post hoc analysis to explore the feasibility of using EASI as an alternative to HMSE and its modifications as the first phase screen in two phase surveys to estimate the prevalence of dementia.
Materials and Methods:
A post hoc analysis was conducted on data obtained from a study conducted on elderly population (60 years and above) from selected geographical areas (Migrant, Urban, Rural and Tribal) of Himachal Pradesh state in North-west India. The co-relation coefficient was used to establish the strength of association between EASI and HMSE and its modification and therefore the feasibility of using it as an alternative.
Results:
As the scores on EASI rise, the scores on HMSE fall both pointing to identification of the same clinical diagnosis i.e., dementia. Further the Pearson Correlation coefficient at -2.52 was found to be statistically significant.
Conclusion:
EASI may be used as alternative to mental state examination.
Key words: Alternative, everyday abilities scale of India, feasibility, mental state examination, two-phase survey
INTRODUCTION
Studies in the past including one by the authors of this study have expressed limitations of using Mini Mental State Examination (MMSE) and its variant like Hindi Mental State Examination (HMSE) in estimating the prevalence of dementia in a largely, illiterate elderly population like ours.[1,2,3] The same cannot be said of the functional ability scales. Indian population has an overall literacy rate of 74%. However, a situation analysis report on elderly in India shows that the literacy rate for persons aged above 60 is much lower at 36%.[4] Furthermore, the literacy level is much less in rural areas at 29.[4]
Researchers in the past across the world have used standardized functional ability tests[5,6,7] with or without MMSE to detect dementia. In this context, researchers in India have used everyday abilities scale of India (EASI).[8]
We conducted a post-hoc analysis of the data from a study conducted by us on the prevalence of dementia in selected geographical areas of Himachal Pradesh, wherein we had used both EASI and HMSE and its modification in the first phase of a two-phase study to estimate the prevalence of dementia.[9] The purpose of this analysis was to explore the feasibility of using EASI as an alternative to HMSE and its modifications as the first phase in two-phase survey to estimate the prevalence of dementia in largely, illiterate Indian population.
MATERIALS AND METHODS
The data used for analysis in the present study were obtained from a study conducted on the elderly population (60 years and above) from selected geographical areas (migrant, urban, rural, and tribal) of Himachal Pradesh, Northwest India.[9] A brief description of the source study is given here.
A total of 500 individuals above 60 years of age were included from each geographical site giving us a target sample size of 2000. The study was a cross-sectional study conducted in two phases: (1) a screening phase and (2) a clinical phase. The screening also involved a detail of the sociodemographic profile of the study population.
Screening
Each participant was asked details regarding participant's age, sex, and educational status. A Hindi version of cognitive screen (HMSE) was used in urban, rural, and migrant population. For the tribal population, a modified (Bharmouri) version referred as Bharmouri Version of Mental State Examination (BMSE) of cognitive screen was used. Screening also involved administration and scoring on EASI
Clinical evaluation and diagnosis
A score <24 (out of a possible score of 30) on cognitive screen was considered as a suspect case of dementia and was evaluated for clinical diagnosis. The clinical evaluation was carried out by a psychiatrist with the help from an internist and two public health specialists. After clinical evaluation, study participants were classified as normal or demented.
For the purpose of this post-hoc analysis, the data of all 2000 participants were analyzed. The analysis focused on correlation of scores on EASI and HMSE/BMSE.
RESULTS
Table 1 provides details on the correlation between EASI scores and HMSE/BMSE scores. The same details have been reproduced in Figure 1. As can be seen from in Table 1 and Figure 1, there is a clear-cut negative correlation between EASI and HMSE/BMSE. Therefore, as the scores on EASI rise, the scores on MMSE fall both pointing to identification of the same clinical diagnosis, i.e., dementia. Further, the Pearson correlation coefficient is −2.52 and this is statistically highly significant [Table 1]. This high statistical significance points to a strong association between EASI and MMSE/BMSE.
Table 1.
Correlations between Everyday abilities score and HMSE/BMSE score
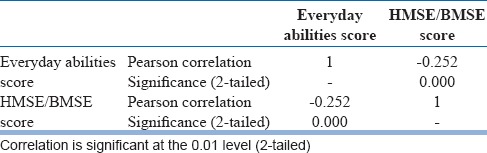
Figure 1.
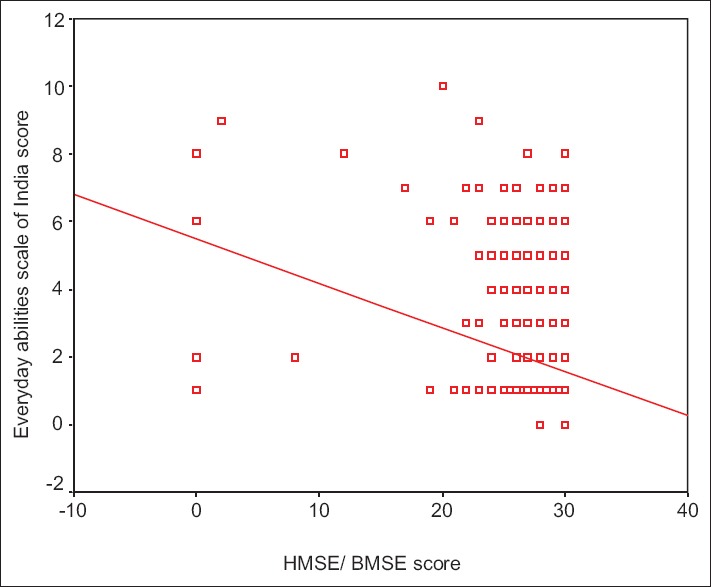
Depicting the correlation between EASI and HMSE/BMSE
DISCUSSION
The current study was conducted with the aim to explore the feasibility of using EASI as an alternative to HMSE and its modifications as the first phase in two-phase survey to estimate the prevalence of dementia in largely, illiterate Indian population. With a predominantly, illiterate elderly population, HMSE and its modification may not be useful in estimating the prevalence of dementia. This is because HMSE and its modification like MMSE use learned language as a medium of assessment.
This becomes important, keeping in view, the fact that majority of elderly Indians are illiterate and it becomes difficult to navigate through various components of Mental State Examination. This is not the case with EASI, wherein response to questions asked from caregivers is recorded. In a study conducted in Ballabgarh, India, among participants who could be tested cognitively, the HMSE, the neuropsychological battery, and EASI had sensitivities of 81.3%, 81.3%, and 62.5%, respectively, with specificities of 60.2%, 74.5%, and 89.7%, respectively. The combination of all three was found to be 93.8% sensitive and 41.8% specific. The sensitivity of the HMSE alone was not significantly improved by the addition of either the EASI or neuropsychological battery, whereas its specificity was significantly decreased by their addition. EASI has an additional advantage that it can be administered to the informants of cognitively untestable subjects.[10]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Ylikoski R, Erkinjuntti T, Sulkava R, Juva K, Tilvis R, Valvanne J. Correction for age, education and other demographic variables in the use of the Mini Mental State Examination in Finland. Acta Neurol Scand. 1992;85:391–6. doi: 10.1111/j.1600-0404.1992.tb06034.x. [DOI] [PubMed] [Google Scholar]
- 2.De Silva R, Disanayaka S, De Zoysa N, Sanjeewanie N, Somaratne S, Foster J, et al. Norms for the mini-mental state examination from a sample of Sri Lankan older people. Int J Geriatr Psychiatry. 2009;24:666–70. doi: 10.1002/gps.2168. [DOI] [PubMed] [Google Scholar]
- 3.Raina SK, Raina S, Chander V, Grover A, Singh S, Bhardwaj A. Development of a cognitive screening instrument for tribal elderly population of Himalayan region in Northern India. J Neurosci Rural Pract. 2013;4:147–53. doi: 10.4103/0976-3147.112744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Situation Analysis of the Elderly in India, 2011. Central Statistics Office Ministry of Statistics & Programme Implementation Government of India. 2011. [Last accessed on 2015 Aug 21]. Available from: http://www.mospi.nic.in/mospi_new/upload/elderly_in_india.pdf .
- 5.Juva K, Mäkelä M, Erkinjuntti T, Sulkava R, Ylikoski R, Valvanne J, et al. Functional assessment scales in detecting dementia. Age Ageing. 1997;26:393–400. doi: 10.1093/ageing/26.5.393. [DOI] [PubMed] [Google Scholar]
- 6.Bronnick K, Ehrt U, Emre M, De Deyn PP, Wesnes K, Tekin S, et al. Attentional deficits affect activities of daily living in dementia-associated with Parkinson's disease. J Neurol Neurosurg Psychiatry. 2006;77:1136–42. doi: 10.1136/jnnp.2006.093146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Avlund K, Kreiner S, Schultz-Larsen K. Functional ability scales for elderly: A validation study. Eur J Public Health. 1996;6:35–42. [Google Scholar]
- 8.Fillenbaum GG, Chandra V, Ganguli M, Pandav R, Gilby JE, Seaberg EC, et al. Development of an activities of daily living scale to screen for dementia in an illiterate rural older population in India. Age Ageing. 1999;28:161–8. doi: 10.1093/ageing/28.2.161. [DOI] [PubMed] [Google Scholar]
- 9.Raina SK, Raina S, Chander V, Grover A, Singh S, Bhardwaj A. Is dementia differentially distributed? A study on the prevalence of dementia in migrant, urban, rural, and tribal elderly population of Himalayan region in Northern India. N Am J Med Sci. 2014;6:172–7. doi: 10.4103/1947-2714.131243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Pandav R, Fillenbaum G, Ratcliff G, Dodge H, Ganguli M. Sensitivity and specificity of cognitive and functional screening instruments for dementia: The Indo-U.S. dementia epidemiology study. J Am Geriatr Soc. 2002;50:554–61. doi: 10.1046/j.1532-5415.2002.50126.x. [DOI] [PubMed] [Google Scholar]