

Abstract
Patient: Male, 18
Final Diagnosis: Perforation
Symptoms: Abdominal pain
Medication: —
Clinical Procedure: Endoscopy
Specialty: Surgery
Objective:
Rare disease
Background:
Toothpick ingestion is implicated in bowel injuries that may cause violent complications, mimicking diseases causing acute abdomen.
Case Report:
A 18-year-old man was admitted with a 3-day history of a swallowed wooden toothpick. The patient had tenderness in the left flank area. Computed tomography indicated toothpick impaction at the splenic flexura of the colon. It was successfully removed with colonoscopy. After the procedure, abdominal radiography showed free air as a sign of perforation. Along with conservative management, the patient was discharged without surgery.
Conclusions:
There is need for greater awareness of the hazardous of an ingested toothpick. Endoscopic approach should be considered in the first-line management of toothpick perforations.
MeSH Keywords: Emergency Service, Hospital; Intestinal Perforation; Radiology Department, Hospital
Background
Most foreign bodies pass through the intestinal tract without any problem, but the risk of morbidity and mortality is higher when long, cutting, rough objects such as chicken bones or toothpicks are swallowed [1,2]. Toothpick ingestion is implicated in intestinal injuries that may cause severe complications, mimicking diseases causing acute abdomen. Potential complications such as hemorrhagia, obstruction, perforation, and fistula are commonly reported [3].
Stomach, duodenum, caecum, sigmoid colon, jejunum, and whole colon are the locations most commonly injured by toothpick ingestion [3–7], while the splenic flexure affected infrequently [4]. The precise identification is made difficult because of few patients can remember swallowing a toothpick.
Additionally, physical examination and laboratory results are not specific, and radiology is generally insufficient to localize toothpicks.
We present successful endoscopic management of a patient who was admitted with a perforation of the splenic flexure caused by ingestion of a wooden toothpick.
Case Report
An 18-year-old man with left abdominal pain was admitted to the emergency clinic with a 4-day history of an inadvertently ingested wooden toothpick. Vital parameters of the patient were 36.7°C body temperature, pulse 90/min, respiratory rate 14/mi, and blood pressure 110/70 mm Hg. On physical examination of the abdomen, rebound and defense were not detected. The patient had minimal tenderness in the left flank area. Intestinal sounds were hypoactive. Hemogram and biochemistry results were within normal range. Abdominal X-ray and ultrasound were normal. Computed tomography imaging demonstrated toothpick impaction at the splenic flexura of the colon (Figure 1). There was no extraluminal abscess or fluid collection. After bowel preoperation with anal enema, colonos-copy was performed. The toothpick was identified in the splenic colon with one end embedded in the bowel lumen and the other end outside the colonic wall (Figure 2). The free end of the toothpick was carefully caught with a polypectomy snare (Figure 2) and the foreign body was gently removed from the colonic wall. The toothpick was eventually dislodged from the anal canal by the endoscopist’s finger (Figure 3).
Figure 1.
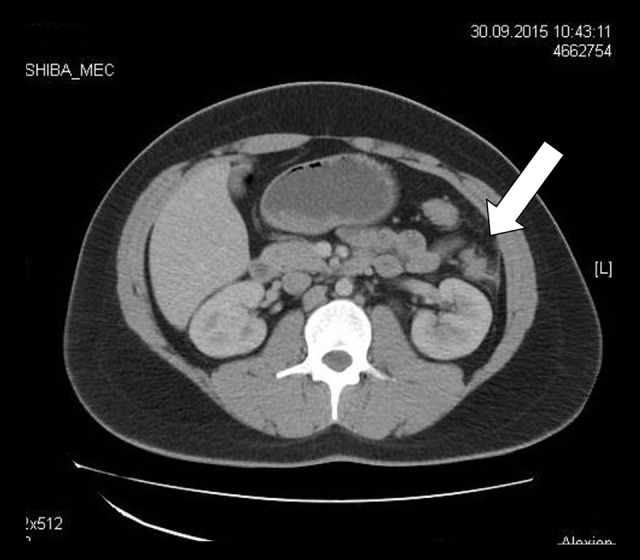
CT scan of the abdomen revealing a foreign body.
White arrow shows the wooden toothpick.
Figure 2.

Endoscopic view of a toothpick impacted in the wall of the splenic flexura (white arrow) (A). Removal of toothpick with polypectomy snare (B).
Figure 3.
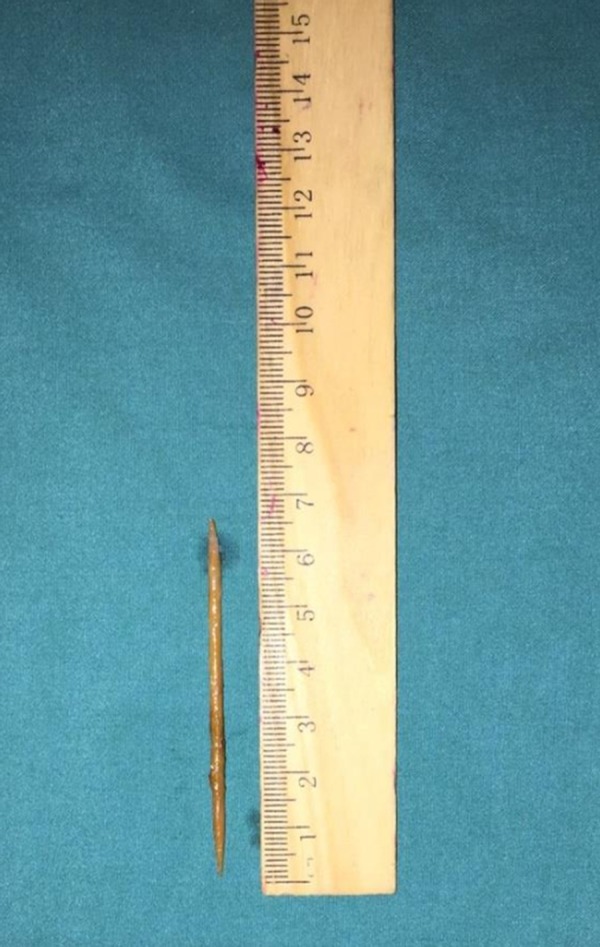
The wooden toothpick (6.5×0.2 cm) after endoscopic removal from the splenic flexura.
Postprocedure, the patient had minimal abdominal pain and the abdominal X-ray was positive for pneumoperitoneum due to insufflation of endoscopy (Figure 4). Intravenous broad-spectrum antibiotic therapy was started and oral intake was stopped. A normal diet was gradually resumed on the third day and antibiotics were replaced by conservative management. The patient was discharged without surgery on the fifth day.
Figure 4.
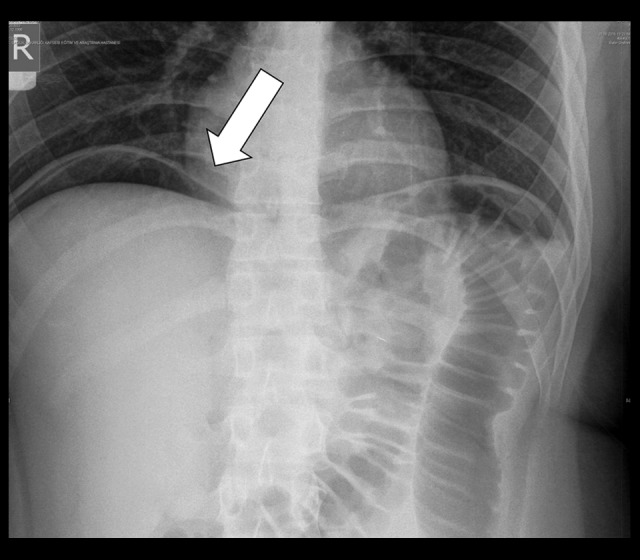
Postprocedure abdominal X-ray with free intra-abdominal air.
Discussion
Swallowed foreign bodies generally (60–90%) travel through the intestinal tract without any problem, and perforation happens in less than 1% of cases [8]. Toothpicks are involved in less than 0.1% of cases [9]. Toothpicks, however, by their nature are more likely to cause intestinal perforations than other objects because they are long and pointed at both ends [10]. The incidence of “toothpick-related injuries” to internal organs is estimated at 0.2/100 000 population [11] and the mortality rate has been reported to be about 18% [4].
Only12% of such patients in fact remember ingesting a toothpick, so many patients who swallow toothpicks do not seek medical assistance, permitting the sharp toothpick to travel down the intestinal tract, and even to enter other intestinal organs, veins, or arteries, causing further injuries [4]. A recent article showed that foreign bodies most often cause perforations in the duodenum (25%), sigmoid colon (14%), and stomach (4%) [4]. Perforation of the splenic flexure of the colon is very rare [4].
With radiological tools, toothpicks were found in 14% of such patients [4]. In our patient we could not see the toothpick in the abdominal imaging or ultrasonography, but the dense, short, and thin toothpick was visualized by computed tomography of the abdomen.
Computed tomography is helpful to achieve clinical information, such as determining the localization of the toothpick and organ injury [12,13]. The intravenous contrast indicated the route made by the toothpick. Hence, we suggest use of contrast agents in similar cases.
The precise diagnosis and management is most commonly made by laparotomy (53%), endoscopy (19%), and computed tomography [4]. Wichmann et al. described use of the laparoscopic approach in an intestinal perforation caused by a toothpick [14]. In our patient, we successfully located the wooden toothpick with colonoscopy, and the endoscopic removal was performed without any problems by using endoscopic instruments.
Postprocedure, the patient had minimal pain in the abdomen and an abdominal X-ray was positive for pneumoperitoneum due to insufflation of endoscopy. After conservative management, the patient discharged without surgery.
Conclusions
Endoscopic removal of a toothpick obviates the need for surgical intervention. Surgical intervention is used in cases in which the ingested toothpick causes complications of peritonitis, abscesses, fistulas, migration to adjacent extra-colonic structures, intractable bleeding, or in those having failed endoscopic retrieval.
References:
- 1.Theodoropoulou A, Roussomoustakaki M, Michalodimitrakis MN, et al. Fatal liver abscess caused by a fish bone. Lancet. 2002;359:977. doi: 10.1016/S0140-6736(02)07999-0. [DOI] [PubMed] [Google Scholar]
- 2.Kumar S, Gupta NM. Foreign bodies migrating from gut to liver. Indian J Gastroenterology. 2000;19:42. [PubMed] [Google Scholar]
- 3.Ioannidis O, Kakoutis E, Sakkas L, et al. Ingested toothpick fistula of the ileum mimicking Crohn’s disease. Acta Gastroenterol Belg. 2010;73:527–29. [PubMed] [Google Scholar]
- 4.Isık A, Demiryılmaz I, Yılmaz I, et al. Effectiveness of manual knotting at laparoscopic appendectomy. GMJ. 2016;27:19–20. [Google Scholar]
- 5.Sadaf A, Hammond I. Answer to case of the month #150 right iliac fossa abscess secondary to cecal perforation by toothpick. Can Assoc Radiol J. 2009;60:146–48. doi: 10.1016/j.carj.2009.02.026. [DOI] [PubMed] [Google Scholar]
- 6.Işik A, Deniz Firat Y, Peker K, et al. How could such a wide piece of tree root pass through the narrow pyloric orifice? An extremely rare case. Am J Case Rep. 2014;15:284–87. doi: 10.12659/AJCR.890713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ragazzi M, Delcò F, Rodoni-Cassis P, et al. Toothpick ingestion causing duodenal perforation. Pediatr Emerg Care. 2010;26:506–7. doi: 10.1097/PEC.0b013e3181e5bf85. [DOI] [PubMed] [Google Scholar]
- 8.Leelouche N, Ayoub N, Bruneel F, et al. Thigh cellulitis caused by toothpick ingestion. Intensive Care Med. 2003;29:662–63. doi: 10.1007/s00134-003-1673-7. [DOI] [PubMed] [Google Scholar]
- 9.Macmanus JE. Perforations of the intestine by ingested foreign bodies: report of two cases and review of the literature. Am J Surg. 1941;53:393–400. [Google Scholar]
- 10.Nash PA, Cregan PC. Perforation of the gastrointestinal tract by a toothpick. Med J Aust. 1987;147:415–16. [PubMed] [Google Scholar]
- 11.Budnick LD. Toothpick-related injuries in the United States, 1979 through 1982. JAMA. 1984;252:796–97. [PubMed] [Google Scholar]
- 12.Matsubara M, Hirasaki S, Suzuki S. Gastric penetration by an ingested toothpick successfully managed with computed tomography and endoscopy. Intern Med. 2007;46:971–74. doi: 10.2169/internalmedicine.46.0037. [DOI] [PubMed] [Google Scholar]
- 13.Işık A, Demiryıldız I, Yılmaz I, et al. Rectal lymphoma. Turkish Colon Rectum Surgery Journal. 2015;25:106–8. [Google Scholar]
- 14.Wichmann MW, Hüttl TP, Billing A, Jauch KW. Laparoscopic management of a small bowel perforation caused by a toothpick. Surg Endosc. 2004;18:717–18. doi: 10.1007/s00464-003-4267-0. [DOI] [PubMed] [Google Scholar]