

Abstract
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is a preventable disease. Long distant travelers are prone to variable degree to develop VTE. However, the low risk of developing VTE among long-distance travelers and which travelers should receive VTE prophylaxis, and what prophylactic measures should be used led us to develop these guidelines. These clinical practice guidelines are the result of an initiative of the Ministry of Health of the Kingdom of Saudi Arabia involving an expert panel led by the Saudi Association for Venous Thrombo Embolism (a subsidiary of the Saudi Thoracic Society). The McMaster University Guideline working group provided the methodological support. The expert panel identified 5 common questions related to the thromboprophylaxis in long-distance travelers. The corresponding recommendations were made following the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach.
Deep venous thromboembolism (DVT) and/or pulmonary embolism (PE) can develop during long distant travel.1-3 Using ultrasound screening, the incidence of DVT in long distance travelers may range between 0-12%.4 Symptomatic venous thromboembolism (VTE) is less common with PE occurring in approximately 0.5 per million travelers on the arrival day5,6 and 27 VTE events (both PE and DVT) per million travelers presenting within 14 days of travel.7 A population-based study estimated that the risk of fatal PE at 0.5 per million and 1.3 per million for air flights lasting >3 hours (hrs) and >8 hrs, respectively.8 For flights of >8 hrs the odds ratio for fatal PE was 7.9 (95% confidence interval [CI]: 1.1-55.1) compared with those who did not undertake a long-distance flight.8 Strategies to prevent travel-associated VTE have been suggested. Maintaining mobility is a reasonable precaution for all travellers on >3 hrs flights.9 The global use of mechanical or pharmacologic prophylaxis compression stockings and anticoagulants is not advocated.9 However, for high risk travelers, guidelines have been issued with conflicting recommendations.9,10 Travelers who are considered at high VTE risk are those with one or more of the following risk factors: previous VTE, active malignancy, recent surgery or trauma, advanced age, severe obesity, estrogen use, pregnancy, limited mobility, and a thrombophilic disorder.11-16
Being the land of the Two Holy Mosques and having a rapidly developing economy, the Kingdom of Saudi Arabia (KSA) is the destination and point of departure of a high number of travelers from and to many distant countries. Currently, there is no guidance for VTE prevention in the long-distance travelers in the KSA. The aim of this document is therefore, to provide such guidance for adult travelers in KSA who have increased VTE risk. The full guideline, which was issued in 2015 is available at: http://www.moh.gov.sa/depts/Proofs/Pages/Guidelines.aspx17
Methods
In March, 2015, the Saudi Ministry of Health (MOH), through the Saudi Center for Evidence Based Healthcare, partnered with a group of clinicians who were nominated by the Saudi Association for VTE (SAVTE) and served as an expert panel for guideline development on VTE prevention. The McMaster University guidelines group provided methodological support. The methodology used to develop recommendations and grade the quality of the supporting evidence is briefly described below. Its details are available in a separate publication.18
The overall process
The KSA guideline panel selected the topic of this guideline and the clinical questions using a formal prioritization process. The McMaster University guideline group updated the relevant systematic reviews that were related to the selected questions. When relevant, the meta-analyses were updated. The group also conducted systematic searches for information specific to the Saudi context, such as patients’ values and preferences and cost. Next, a McMaster guideline group (led by EAA) developed a summary of findings and evidence-to-decision tables for each question and shared them with the panel members. The guideline panel was asked to provide additional relevant information, including unpublished data. The guideline panel met in Riyadh, KSA in March 2015 and developed the final recommendations using a structured consensus process with transparent documentation of all decisions. Potential conflicts of interests of the panel members were managed according to the World Health Organization rules.19
The selected questions
The following is a list of the clinical questions selected by the KSA guideline panel and addressed in this guideline. For details on the process by which the questions were selected please refer to the separate methodology publication.18
Should frequent ambulation versus no frequent ambulation be used for VTE prophylaxis in long-distance travelers at increased risk of VTE?
Should calf muscle exercise versus no calf muscle exercise be used for VTE prophylaxis in long-distance travelers at increased risk of VTE?
Should sitting in an aisle seat versus no sitting in an aisle seat be used for VTE prophylaxis in long-distance travelers at increased risk of VTE?
Should anticoagulants versus no anticoagulants be used for VTE prophylaxis in long-distance travelers at increased risk of VTE?
Should graduated compression stockings (GCS) versus no GCS be used for VTE prophylaxis in long-distance travelers at increased risk of VTE?
Grading the quality of evidence
The panel assessed the quality of evidence using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach.20 Quality of evidence was classified as “high”, “moderate”, “low”, or “very low” based on the following factors: risk of bias, indirectness, imprecision, inconsistency, and publication bias. The definition of each category is as follows:21
High: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate: We are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low: Our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.
Very low: We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect.
Grading the strength of recommendations
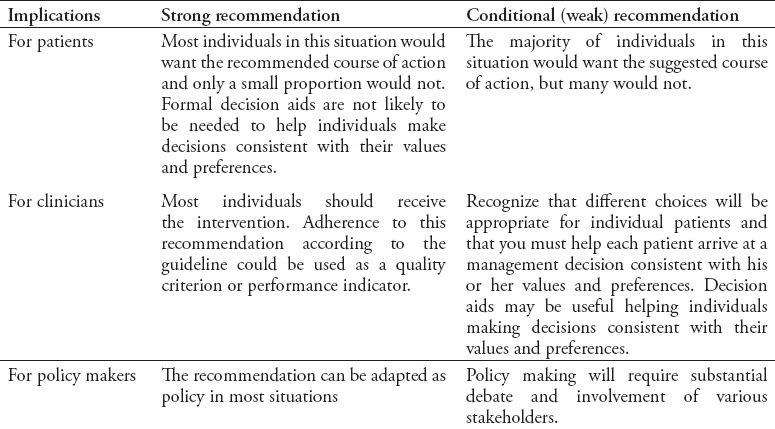
The GRADE Working Group defines the strength of recommendation as the extent to which we can be confident that desirable effects of an intervention outweigh undesirable effects.22 The strength is dependent on a number of factors including: priority of the problem, quality of evidence, balance of benefits and harms, resources use, impact on equity, acceptability, and feasibility. According to the GRADE approach, the strength of a recommendation is either strong or conditional (weak), in favour or against, and has explicit implications (Table 1).22
Table 1.
Interpretation of strong and conditional (weak) recommendations.
Results
The panel provided 5 recommendations to cover thromboprophylaxis in long-distance travelers in the Saudi context.
Definitions
We defined travelers who are at high risk of VTE as those with one or more of the following risk factors: previous VTE, active malignancy, recent surgery or trauma, advanced age, severe obesity, estrogen use, pregnancy, limited mobility, and a thrombophilic disorder.11-16 We also defined long-distance travel as flights that are longer than 8 hours in duration.5,13,23-26
Question 1: Should frequent ambulation versus no frequent ambulation be used for VTE prophylaxis in long-distance travelers at increased risk of VTE?
Summary of findings
Our review did not identify any eligible systematic review or eligible trial. We identified one relevant case-control study, the Multiple Environmental and Genetic Assessment of risk factors for venous thrombosis study.26 The study included 11033 individuals who had travelled for more than 4 hours by air within the previous 8 weeks, and assessed a number of risk factors. The adjusted odds ratio for the association between exercising during flight and thrombosis was 1.2 (95% CI: 0.6-2.6).
Benefits and harms of the option
Given the nature of the available evidence, we could not estimate the absolute effect of frequent ambulation compared with no frequent ambulation in long-distance travelers. No potentially significant harm was identified.
Resource use
The panel judged the cost of frequent ambulation to be small and probably cost effective for long-distance travelers at increased VTE risk.
Feasibility, acceptability, and equity considerations
The panel judged frequent ambulation to probably be feasible and acceptable in long-distance travelers at increased VTE risk. The panel was uncertain about the impact of frequent ambulation on health inequity in long-distance travelers at increased VTE risk.
Balance between desirable and undesirable consequences
The panel judged the benefits of frequent ambulation for the prophylaxis of VTE to probably outweigh the harms in long-distance travelers. The certainty of the evidence was considered to be very low. The panel judged the intervention to be low-cost, probably cost effective, feasible and acceptable.
Recommendation 1:
In long distance (>8 hrs duration) high-risk travelers the panel suggests frequent ambulation for the prophylaxis of VTE (conditional recommendation, very low quality evidence).
Question 2: Should calf muscle exercise versus no calf muscle exercise be used for VTE prophylaxis in long-distance travelers at increased risk of VTE?
Summary of findings
Our review did not identify any eligible systematic review or eligible trial. As mentioned above, the Multiple Environmental and Genetic Assessment of risk factors for venous thrombosis case-control study found an adjusted odds ratio for the association between exercising during flight and thrombosis of 1.2 (95% CI: 0.6-2.6).26
Benefits and harms of the option
Given the nature of the available evidence, we could not estimate the absolute effect of calf muscles exercises compared with no calf muscle exercise for VTE prophylaxis in long-distance travelers. No potentially significant harm was identified.
Feasibility, acceptability and equity considerations
The panel judged calf muscle exercise to probably be feasible and acceptable for VTE prophylaxis in long-distance travelers. The panel was uncertain about the impact of calf muscle exercise on health inequity for VTE in long-distance travelers.
Balance between desirable and undesirable consequences
The panel judged the benefits of calf muscle exercise for prophylaxis of VTE to probably outweigh the harms in long-distance travelers. The certainty of the evidence was considered to be very low. The panel judged the intervention to be feasible and acceptable.
Recommendation 2:
In long distance (>8 hrs duration) high-risk travelers the panel suggests calf muscle exercise for the prophylaxis of VTE. (conditional recommendation, very low quality evidence).
Question 3: Should sitting in an aisle seat versus no sitting in an aisle seat be used for VTE prophylaxis in long-distance travelers at increased risk of VTE?
Summary of findings
Our review did not identify any eligible systematic review or eligible trial. The Multiple Environmental and Genetic Assessment of risk factors for venous thrombosis case-control study found that window seating compared with aisle seating was associated with thrombosis (odds ratio: 2.2; 95% CI: 1.1-4.4).26
Benefits and harms of the option
Given the nature of the available evidence, we could not estimate the absolute effect of aisle seating compared with window seating for VTE prophylaxis in long-distance travelers. No potentially significant harm was identified.
Feasibility, acceptability, and equity considerations
The panel judged sitting in an aisle to probably be feasible and acceptable for VTE prophylaxis in long-distance travelers. The panel was uncertain about the impact of sitting in an aisle seat on health inequity for VTE in long-distance travelers.
Balance between desirable and undesirable consequences
The panel judgedthe benefits of sitting in the aisle seat for the prophylaxis of VTE to probably outweigh its harms in long-distance travelers. The certainty of the evidence was considered to be very low. The panel judged the intervention to be feasible and acceptable.
Recommendation 3:
In long-distance (>8 hrs duration) high-risk travelers the panel suggests sitting in an aisle seat for the prophylaxis of VTE. (conditional recommendation, very low quality evidence).
Question 4: Should anticoagulants versus no anticoagulants be used for VTE prophylaxis in long-distance travelers at increased risk of VTE?
Summary of findings
We identified one trial comparing LMWH, aspirin and no drug intervention in 300 “high-risk” air travelers.25 Participants were scanned for asymptomatic DVT, and there were 0 events in 82 individuals receiving LMWH, 3 events in 84 receiving aspirin, and 4 events in 83 individuals in the control group. None of the reported events was a symptomatic VTE.
Benefits and harms of the option
We could not estimate the absolute effect of anticoagulant use compared with no anticoagulant use for VTE prophylaxis in long-distance travelers. There is indirect evidence about the increased risk of bleeding with anticoagulants.
Resource use
The panel judged the cost of anticoagulant use to be probably not small and probably not cost effective for VTE prophylaxis in long-distance travelers.
Feasibility, acceptability, and equity considerations
The panel judged anticoagulant use to probably not be feasible and acceptable for VTE prophylaxis in long-distance travelers. The panel was uncertain about the impact of anticoagulant use for VTE prevention on health inequity in long-distance travelers.
Balance between desirable and undesirable consequences
The panel judged the benefits of offering pharmacological thromboprophylaxis to probably outweigh the harms in long-distance travelers at increased VTE risk. The certainty of the evidence was considered to be very low. The panel, however, judged the intervention to be neither of low-cost, cost effective, feasible or acceptable.
Recommendation 4:
In long-distance (>8 hrs duration) travelers at increased risk of VTE, the panel suggests using anticoagulants. (conditional recommendation, very low quality evidence).
Research priorities
Consider conducting studies on efficacy and safety of anticoagulant thrombo-prophylaxis in long-distance high-risk travelers.
Question 5: Should GCS versus no GCS be used for VTE prophylaxis in long-distance travelers at increased risk of VTE?
Summary of findings
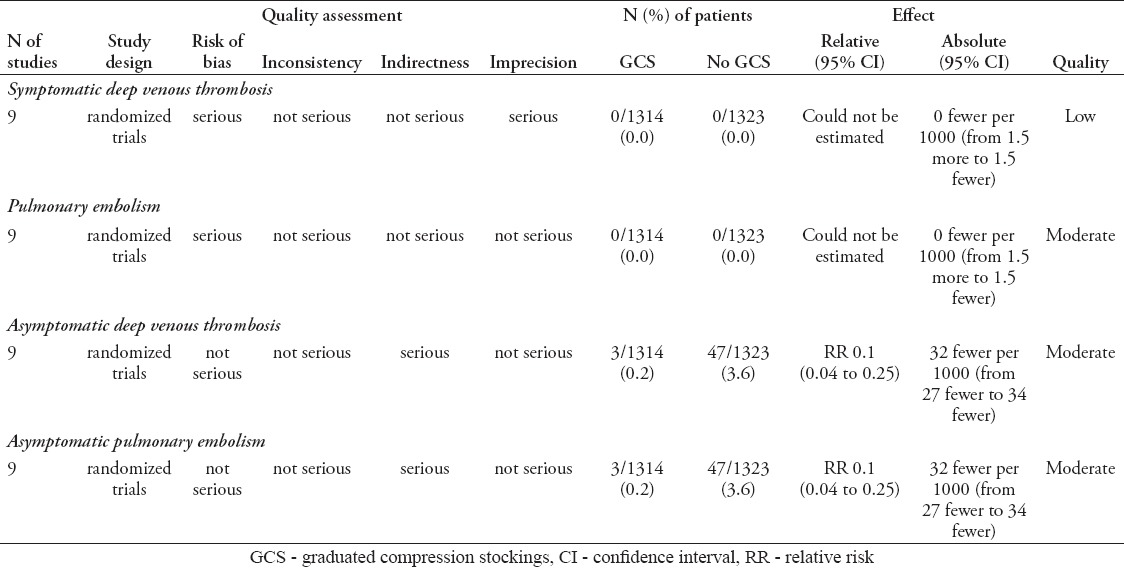
We updated a Cochrane systematic review by Clarke et al,27 but we did not identify new studies. The summary of findings is presented in Table 2.
Table 2.
Graduated compression stockings (GCS) compared with no GCS for venous thromboembolism in long distance travelers.
Benefits and harms of the option
The meta-analysis of 9 trials (total of 2,637 participants) for the use of GCS compared with no GCS in long-distance travelers found:
Low quality evidence for symptomatic DVT; while we could not estimate the relative effect, the absolute effect was: 0 fewer per 1000; 95% CI: 1.5-1.5.
Moderate quality evidence for PE; while we could not estimate the relative effect, the absolute effect was: 0 fewer per 1000; 95 % CI: 1.5-1.5
Moderate quality evidence that did not rule out a reduction or an increase in symptomless DVT with a RR: 0.1; 95% CI: 0.04 to 0.25; absolute effect: 32 fewer events per 1000; 95% CI: 27-34.
Moderate quality evidence that did not rule out a reduction or an increase in symptomless PE with a RR: 0.1; 95% CI: 0.04 to 0.25; absolute effect: 32 fewer events per 1000; 95% CI: 27-34).
Resource use
The panel judged the cost of GCS to probably not be small and probably not be cost effective for VTE prophylaxis in long-distance travelers.
Feasibility, acceptability, and equity considerations
The panel judged the use of GCS to probably not be feasible or acceptable. The panel was uncertain about the impact of GCS on health inequity in long-distance travelers.
Balance between desirable and undesirable consequences
The panel judged the harms of GCS for prevention of VTE to probably outweigh its benefits in long-distance high-risk travelers. The certainty of the evidence was considered to be very low. The panel judged the intervention to be of high cost and probably not cost effective. The panel also judged the intervention to be neither feasible nor acceptable.
Recommendation 5:
In long-distance (>8 hrs duration) high-risk travelers, the panel suggests not using GCS for the prophylaxis of VTE. (conditional recommendation, very low quality evidence).
Discussion
The purpose of this clinical practice guideline is to provide guidance on selected clinical questions related to VTE prevention in long-distance travelers. The recommendations were made taking into account the available evidence, resource use, patient preference and the Saudi context. The target audience of the guideline includes primary care physicians, internists and specialists in Internal Medicine. However, it is not intended to be a care standard. Clinicians, patients, third-party payers, institutional review committees, other stakeholders and courts should never view the guideline recommendations as dictates.
VTE is a relatively rare complication of travel,5-7 but can be fatal.8 There is limited evidence on thrompoprophylaxis in long distance travelers. This has probably led to weak and sometimes conflicting recommendations.9,10 A guideline from the United Kingdom recommended VTE risk assessment, stated that well fitted below knee compression stockings should be put on by high risk travelers and suggested the use of pharmacologic prophylaxis.9 On the other hand, the ninth edition of the American College of Chest Physicians Evidence-Based Clinical Practice Guidelines suggested the use of properly fitted below-knee GCS at the ankle for high risk travellers and against the use of pharmacologic prophylaxis.10 Both guidelines suggested maintain mobility.9,10 The recommendations in this guideline are different. The Saudi guideline suggested pharmacologic prophylaxis and was against GCS use for high risk long distance travellers.
VTE prevention in long-distance travelers is one of the public health issues that requires increased public awareness. Hence, dissemination of the recommendations in this guideline is important. However, we should note that the evidence on VTE prevention in long-distance travelers is either lacking or of low quality. Further research is needed to determine the effectiveness and safety of the various VTE prevention modalities in this population.
In conclusion, Long distant travelers are prone to develop DVT and/or PE, especially those with VTE risk factors. This evidence-based clinical practice guideline may help the healthcare providers working in KSA in reducing the variabilities in thromprophylaxis practices for high risk long distance travellers. The guideline suggested frequent ambulation, calf muscle exercise, sitting in an aisle seat and pharmacologic prophylaxis for high risk long distance travellers. It also suggested against GCS use. Further studies are needed as the evidence on thromboprophylaxis in long distance travellers is either lacking or of low quality.
Acknowledgment
The authors would like to thank Dr. Zulfa Alrayess, Dr. Yaser Adi, and the rest of the members of the Saudi Center for Evidence Based Healthcare, Ministry of Health, Riyadh, Kingdom of Saudi Arabia for their unlimited support.
Footnotes
References
- 1.Hughes RJ, Hopkins RJ, Hill S, Weatherall M, Van de Water N, Nowitz M, et al. Frequency of venous thromboembolism in low to moderate risk long distance air travellers: the New Zealand Air Traveller’s Thrombosis (NZATT) study. Lancet. 2003;362:2039–2044. doi: 10.1016/s0140-6736(03)15097-0. [DOI] [PubMed] [Google Scholar]
- 2.Cannegieter SC, Doggen CJ, van Houwelingen HC, Rosendaal FR. Travel-related venous thrombosis: results from a large population-based case control study (MEGA study) PLoS Med. 2006;3:e307. doi: 10.1371/journal.pmed.0030307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Scurr JH, Machin SJ, Bailey-King S, Mackie IJ, McDonald S, Smith PD. Frequency and prevention of symptomless deep-vein thrombosis in long-haul flights: a randomised trial. Lancet. 2001;357:1485–1489. doi: 10.1016/S0140-6736(00)04645-6. [DOI] [PubMed] [Google Scholar]
- 4.Philbrick JT, Shumate R, Siadaty MS, Becker DM. Air travel and venous thromboembolism: a systematic review. J Gen Intern Med. 2007;22:107–114. doi: 10.1007/s11606-006-0016-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lapostolle F, Surget V, Borron SW, Desmaizières M, Sordelet D, Lapandry C, et al. Severe pulmonary embolism associated with air travel. N Engl J Med. 2001;345:779–783. doi: 10.1056/NEJMoa010378. [DOI] [PubMed] [Google Scholar]
- 6.Pérez-Rodríguez E, Jiménez D, Díaz G, Pérez-Walton I, Luque M, Guillén C, et al. Incidence of air travel-related pulmonary embolism at the Madrid-Barajas airport. Arch Intern Med. 2003;163:2766–2770. doi: 10.1001/archinte.163.22.2766. [DOI] [PubMed] [Google Scholar]
- 7.Kelman CW, Kortt MA, Becker NG, Li Z, Mathews JD, Guest CS, et al. Deep vein thrombosis and air travel: record linkage study. BMJ. 2003;327:1072. doi: 10.1136/bmj.327.7423.1072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Parkin L, Bell ML, Herbison GP, Paul C, Skegg DC. Air travel and fatal pulmonary embolism. Thromb Haemost. 2006;95:807–814. [PubMed] [Google Scholar]
- 9.Watson HG, Baglin TP. Guidelines on travel-related venous thrombosis. Br J Haematol. 2011;152:31–34. doi: 10.1111/j.1365-2141.2010.08408.x. [DOI] [PubMed] [Google Scholar]
- 10.Kahn SR, Lim W, Dunn AS, Cushman M, Dentali F, Akl EA, et al. Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e195S–226S. doi: 10.1378/chest.11-2296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kesteven P, Robinson B. Incidence of symptomatic thrombosis in a stable population of 650,000: travel and other risk factors. Aviat Space Environ Med. 2002;73:593–596. [PubMed] [Google Scholar]
- 12.Cannegieter SC, Doggen CJ, van Houwelingen HC, Rosendaal FR. Travel-related venous thrombosis: results from a large population-based case control study (MEGA study) PLoS Med. 2006;3:e307. doi: 10.1371/journal.pmed.0030307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Schwarz T, Siegert G, Oettler W, Halbritter K, Beyer J, Frommhold R, et al. Venous thrombosis after long-haul flights. Arch Intern Med. 2003;163:2759–2764. doi: 10.1001/archinte.163.22.2759. [DOI] [PubMed] [Google Scholar]
- 14.Arfvidsson B, Eklof B, Kistner RL, Masuda EM, Sato DT. Risk factors for venous thromboembolism following prolonged air travel. Coach class thrombosis. Hematol Oncol Clin North Am. 2000;14:391–400. doi: 10.1016/s0889-8588(05)70140-4. [DOI] [PubMed] [Google Scholar]
- 15.Martinelli I, Taioli E, Battaglioli T, Podda GM, Passamonti SM, Pedotti P, et al. Risk of venous thromboembolism after air travel: interaction with thrombophilia and oral contraceptives. Arch Intern Med. 2003;163:2771–2774. doi: 10.1001/archinte.163.22.2771. [DOI] [PubMed] [Google Scholar]
- 16.Guyatt GH, Akl EA, Crowther M, Gutterman DD, Schuünemann HJ. American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis Panel. Executive summary: Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 suppl):7S–47S. doi: 10.1378/chest.1412S3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Al-Hameed F, Abdelaal MA, Alaklabi A, Aldahan S, Al-Dorzi HM, Alomi YA, et al. Clinical Practice Guideline on Prophylaxis of VTE in Medical Patients and Long Distance Travelers. 2015. [Update 2015, Accessed 2016 July 30]. Available from: http://www.moh.gov.sa/endepts/Proofs/Pages/Guidelines.aspx .
- 18.McMaster University Guideline Working Group. Methodology for the Development of the Ministry of Health of Saudi Arabia and McMaster University Clinical Practice Guidelines. 2014. [Accessed 2015 February 23]. Available from: http://www.moh.gov.sa/endepts/Proofs/Pages/GuidelineAdaptation.aspx .
- 19.World Health Organization. WHO Handbook for Guideline Development. Geneva (CH): WHO; 2012. [Cited 2014 February 7]. Available from: http://apps.who.int/iris/bitstream/10665/75146/1/9789241548441_eng.pdf . [Google Scholar]
- 20.Brożek JL, Akl EA, Compalati E, Kreis J, Terracciano L, Fiocchi A, et al. Grading quality of evidence and strength of recommendations in clinical practice guidelines part 3 of 3. The GRADE approach to developing recommendations. Allergy. 2011;66:588–595. doi: 10.1111/j.1398-9995.2010.02530.x. [DOI] [PubMed] [Google Scholar]
- 21.Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines:3. Rating the quality of evidence. J Clin Epidemiol. 2011;64:401–406. doi: 10.1016/j.jclinepi.2010.07.015. [DOI] [PubMed] [Google Scholar]
- 22.Andrews J, Guyatt G, Oxman AD, Alderson P, Dahm P, Falck-Ytter Y, et al. GRADE guidelines:14. Going from evidence to recommendations: the significance and presentation of recommendations. J Clin Epidemiol. 2013;66:719–725. doi: 10.1016/j.jclinepi.2012.03.013. [DOI] [PubMed] [Google Scholar]
- 23.Hughes RJ, Hopkins RJ, Hill S, Weatherall M, Van de Water N, Nowitz M, et al. Frequency of venous thromboembolism in low to moderate risk long distance air travellers: the New Zealand Air Traveller’s Thrombosis (NZATT) study. Lancet. 2003;362:2039–2044. doi: 10.1016/s0140-6736(03)15097-0. [DOI] [PubMed] [Google Scholar]
- 24.Philbrick JT, Shumate R, Siadaty MS, Becker DM. Air travel and venous thromboembolism: a systematic review. J Gen Intern Med. 2007;22:107–114. doi: 10.1007/s11606-006-0016-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Cesarone MR, Belcaro G, Nicolaides AN, Incandela L, De S, Geroulakos G, et al. Venous thrombosis from air travel: the LONFLIT3 study--prevention with aspirin vs low-molecular-weight heparin (LMWH) in high-risk subjects: a randomized trial. Angiology. 2002;53:1–6. doi: 10.1177/000331970205300101. [DOI] [PubMed] [Google Scholar]
- 26.Schreijer AJ, Cannegieter SC, Doggen CJ, Rosendaal FR. The effect of flight-related behaviour on the risk of venous thrombosis after air travel. Br J Haematol. 2009;144:425–429. doi: 10.1111/j.1365-2141.2008.07489.x. [DOI] [PubMed] [Google Scholar]
- 27.Clarke M, Hopewell S, Juszczak E, Eisinga A, Kjeldstrøm M. Compression stockings for preventing deep vein thrombosis in airline passengers. Cochrane Database Syst Rev. 2006;2:CD004002. doi: 10.1002/14651858.CD004002.pub2. [DOI] [PubMed] [Google Scholar]