

Abstract
Objectives:
To examin the effect of Ramadan fasting on worsening of renal function (WRF).
Method:
This was a single-arm prospective observational study including 65 patients with stage 3 or higher chronic kidney disease (CKD). By definition, WRF was considered to have occurred when serum creatinine levels increased by 0.3 mg/dL (26.5 µmol/l) from baseline during or within 3 months after Ramadan. The study was conducted in the Nephrology Clinic of King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia during the month of Ramadan 1436 AH (Hijiri), which corresponded to June 18-July 17, 2015.
Results:
This study included 65 adults with a mean age of 53 years. Overall, 33% of patients developed WRF. In the multivariate analysis, more advanced CKD stage, higher baseline systolic blood pressure and younger age were independently associated with WRF. Underlying cause of CKD, use of diuretics, use of renin angiotensin blockers, gender, and smoking status were not associated with WRF.
Conclusion:
In patients with stage 3 or higher CKD, Ramadan fasting during the summer months was associated with worsening of renal function. Clinicians need to warn CKD patients against Ramadan fasting.
Fasting during the holy month of Ramadan is one of the 5 pillars of Islam. During Ramadan, Muslims must abstain from eating or drinking from dawn to sunset every day for a whole month.1 Ramadan is the ninth month of the Islamic lunar calendar (Hijri) year, which consists of 354 days, whereas the Gregorian calendar year consists of 365 days. Accordingly, Ramadan can occur during any of the 4 seasons of the year. Moreover, the duration of fasting varies from 12-18 hours depending on the geographical location of the country. Although there is an exemption from fasting provided to sick people,2 many of these patients wish to fast. Physicians in Muslim countries are frequently consulted by their patients regarding the effects of fasting on their health, including patients with chronic kidney disease (CKD). Although many studies have shown that fasting during Ramadan has no adverse effect on healthy people,3-5 the few studies that have been conducted on the effect of Ramadan in patients with CKD have found inconsistent results.6-9 Moreover, some of these studies were conducted during the winter season, and others were conducted during the summer time. Therefore, we carried out this study on the effect of Ramadan fasting on worsening of renal function (WRF) in patients with more advance CKD during the period in summer with the longest days.
Methods
A single-arm prospective observational study was conducted, including 65 patients with stage 3 or higher CKD (glomerular filtration rate [GFR] <60 ml/min), as estimated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula.10,11 The definition and classification of CKD were based on the recommendations in the international guidelines published by Kidney Disease Improving Global Outcomes (KDIGO) in 2004.12 There were 40 male and 25 female patients included in the study. Our target population was patients recruited from the Nephrology Clinic of King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia during the month of Ramadan 1436 AH (Hijri), which corresponded to June 18-July 17, 2015. In 2015, Ramadan occurred during the summer season, and therefore the fasting period lasted 15 hours per day (3:30 AM-6:30 PM). Ethical approval was obtained from the Institutional Review Board of King Saud University, Riyadh, Kingdom of Saudi Arabia. Informed consent was obtained from the patients upon participation, and our study was performed according to the Declaration of Helsinki Principles. All patients were advised not to fast; however, patients frequently fasted against medical advice. Patients who elected to fast were offered blood testing to ensure their safety. We included patients with stage 3, stage 4, and stage 5 CKD, and an age of 18 years or older who fasted during Ramadan. We excluded patients with kidney transplants, current pregnancy, poorly controlled diabetes (HbA1C >9) and poorly controlled hypertension (defined as systolic blood pressure [SBP] of more than 180 or diastolic blood pressure [DBP] of more than 100 mm Hg) from the cohort.13-14
Clinical and biochemical variables were collected at 3 different time points. Blood samples for laboratory testing were collected during the daytime. Data were collected within the 3 months before fasting initiation, after fasting for at least 10 days, and 3 months after Ramadan, according to a previously described sampling frequency.15 Clinical variables included the following: SBP, DBP, weight, height, history of diabetes, history of hypertension, medications, history of smoking, and underlying cause of end stage renal disease. Serum creatinine was measured using a multipoint enzymatic spectrophotometric assay. We collected the following biochemical samples: serum urea and electrolyte, serum creatinine, glucose, HbA1C, serum uric acid and hemoglobin levels, and a lipid profile. The endpoint was the worsening of renal function. By definition, WRF was considered to have occurred when serum creatinine level increased by 0.3 mg/dl (26.5 µmol/L) from baseline during or within the 3 months after Ramadan based on the Kidney Disease Improving Global Outcomes (KDIGO) guidelines.16 We also examined changes in electrolyte levels and lipid and glucose control.
Statistical analysis
Continuous variables with normal or symmetrical distributions were expressed as the means and standard deviations (SD). Otherwise, medians and 25th and 75th percentiles (interquartile ranges) were used. Categorical variables were expressed as frequencies or percentages. Changes in the variables from baseline were examined using paired Student’s t-tests or Wilcoxon’s rank-sum tests for continuous variables and likelihood χ2 and Fisher’s exact tests for categorical variables. We analyzed the impact of gender, cause of CKD, age, diabetes, smoking status, history of hypertension, angiotensin-converting enzyme (ACE) or angiotensin receptor blocker (ARB) use, diuretic use and systolic blood pressure on WRF as a continuous variable and categorical variable (by quartiles) to identify predictors of worsening of renal function. Baseline factors associated with WRF were determined using Cox proportional hazard’s models. Repeated measures analysis of variance was used to study the within group change over time. A p value of ≤0.05 was considered significant. All analyses were conducted using the Statistical Analysis System software version 9.2 (SAS Institute, Inc., Cary, NC).
Results
In this study, we included a total of 65 patients with CKD. Table 1 shows the baseline characteristics of patients who were included in this analysis. Thirty-six patients had CKD stage 3 (55.4%), 24 patients had CKD stage 4 (36.9%), and 5 patients had CKD stage 5 (7.7%). The cause of CKD was diabetic nephropathy in 13 patients, hypertensive nephropathy in 14 patients, glomerular causes in 10 patients, and other causes in 28 patients. Mean serum creatinine (SD) was identified as 206 µmol/l (88) before Ramadan, 214 µmol/l (37) during Ramadan, and 209 µmol/l (101) 3 months after fasting. Twenty-two patients (33.8%) developed WRF; of the patients, 15 developed WRF during Ramadan and 7 in 3 months after Ramadan, as shown in Table 2. Of the 22 patients who developed WRF, 8 later improved, while 14 continued to have elevated serum creatinine. In the multivariate analysis, more advanced CKD stage, higher baseline systolic blood pressure, and younger age were independently associated with WRF. An improvement in mean systolic blood pressure and HbA1C was observed post-Ramadan compared with values before Ramadan, as shown in Table 3.
Table 1.
Baseline characteristics of the participants.
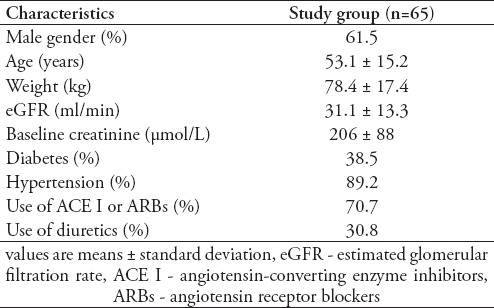
Table 2.
Effect of fasting on the development of worsening renal function in patients with different stages of chronic kidney disease.
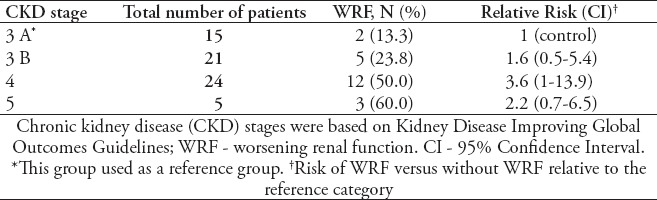
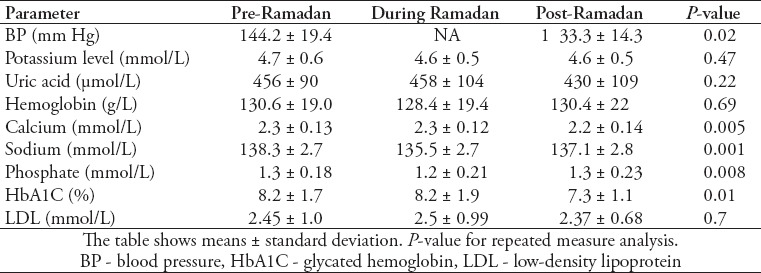
Table 3.
Systolic blood pressure and biochemical parameters before Ramadan, during Ramadan, and 3 months after Ramadan.
Impact of fasting on metabolic parameters
Fasting did not have any impact on potassium, sodium, calcium, phosphorous, or uric acid levels (Table 3). However, a significantly lower mean blood systolic pressure was observed post-fast. Mean SBP was 144 mm Hg before fasting and decreased to 133 mm Hg after Ramadan fasting. Similarly, mean HbA1c improved from 8.2% to 7.3% after fasting. No effect of fasting on cholesterol was identified. A significant difference in potassium level during fasting was not identified. Only 2 patients out of the whole cohort developed hyperkalemia, and the development of hyperkalemia was not associated with worsening of renal function. Calcium and phosphate levels were lower and higher during the post-fasting period (Table 3). We also observed a lower sodium level during fasting that returned to the baseline value post-fast. Table 4 shows the baseline data and clinical outcomes based on the gender. There were no differences between women and men in baseline creatinine level, age or prevalence of diabetes or hypertension. Similarly, there was no difference in the prevalence of hyperkalemia during fasting between men and women.
Discussion
According to the Quran, Allah has mandated fasting for every post-pubescent person who is physically fit enough to fast and has promised an abundant reward in return. He has, however, exempted those with illness from fasting, permitting them to break their fast until the reason for which they have been exempted is resolved.2-3 Nevertheless, many patients with CKD insist on fasting during Ramadan, thereby creating a medical challenge for themselves and their health care providers. It has become increasingly important that medical professionals are aware of the potential risks associated with fasting during Ramadan and potential approaches to mitigate those risks. These issues are rapidly becoming global issues, as Muslim have been found to account for up to one fifth of the global population.17 The effects of Ramadan fasting on kidney function among patients may create a challenge for clinicians treating patients with moderate to severe CKD, as information is sparse and no guidelines or standardized protocols exist. Similarly, it would not be ethical to conduct a controlled trial to monitor for potential adverse effects. In our institute, we routinely discourage patient with stage 3 or higher CKD against fasting; however, some patients do fast against medical advice. This study reports the impact of Ramadan fasting among patients with advanced CKD during the long, hot days of summer.
We observed WRF in 33.8% of patients who participated in Ramadan fasting. The proportion of patients with worsening renal function increased incrementally with increased CKD stage. Furthermore, we observed that in addition to more advance CKD stage, higher baseline systolic blood pressure, and younger age were independently associated with WRF. In contrast to our study, El-Wakil et al,6 Bernieh et al,7 and Alwakeel et al8 reported that Ramadan fasting was safe in CKD patients; however, these studies included smaller sample sizes and were conducted during the winter when the average temperature was 18 °C and the fasting duration was 12 hours. However, NasrAllah et al15 reported that renin angiotensin aldosterone system antagonist use and diuretic use were associated with increased serum creatinine at day 7 of fasting. Our results showed that the underlying cause of CKD and use of diuretics or renin angiotensin blockers was not associated with WRF. The change in creatinine identified in this study was persistent, as most patients continued to have elevated creatinine after Ramadan. This finding has also been reported by other investigators.6-7 The impact of fasting on blood pressure has been examined in other studies. Samad et al18 reported that intermittent fasting was associated with a drop in both systolic and diastolic blood pressure in normotensive males. Our data showed an improvement in mean systolic blood pressure post-Ramadan fasting (p=0.02), and similar findings were also observed in the study carried by Bernieh et al.7 Ramadan fasting has been found to lead to weight loss and fat-free mass reduction. Body composition changes have been found to vary depending on age and gender.19 Aksungar et al.20 demonstrated that intermittent fasting led to some beneficial changes in serum HDL, plasma homocysteine levels, and coagulation status. We noted that diabetic control improved with fasting, and HbA1c decreased significantly. The EPIDIAR study showed a 5-fold increase in the incidence of severe hyperglycemia among patients with diabetes during Ramadan, but did not report post-Ramadan HbA1C levels.21
It has also been recognized that major adverse cardiovascular events occurred more frequently among fasting CKD patients with pre-existing cardiovascular disease, and these events were hypothesized to be caused by an early increase in serum creatinine.15 Our study found that the adverse effects associated with Ramadan fasting also extended to worsening of renal function. It has been hypothesized that restricted fluid intake during fasting, especially if prolonged, may cause volume contraction and become severe as a result of excessive perspiration in hot and humid climates and among individuals who perform hard physical labor. In our study, sodium levels during Ramadan were lower than pre- and post-Ramadan levels. This was most likely associated with increased water intake at night during Ramadan to compensate for the fasting period during the day. The impact of fasting on various electrolytes was variable. Though fasting has been reported to cause hyperkalemia,22 we did not observe a significant change in hyperkalemia prevalence within our cohort. Most patients with worsening of renal function were identified during Ramadan and did not improve after Ramadan, indicating the possibility of permanent deleterious effects on kidney function caused by fasting. Though the association between gender and worsening of renal function among those who fasted during Ramadan did not reach statistical significance, there was a trend that indicated a higher prevalence of worsening of renal function among the female participants. A possible explanation for this result is that it may be associated with the higher total body water volume in women, making them more prone to volume contraction during fasting. However, a larger study is needed to address the finding. The strength of this study was that all subjects completed 30 days of fasting and were available at follow-up with complete data. Similarly, this study was conducted during a hot summer month and including patients with advanced kidney disease.
There are a few limitations to this study. The lack of a control cohort limits our ability to determine the causal effect of fasting on worsening of renal function and metabolic outcomes, and the use of a small convenience sample limits the generalizability of the findings to the wider population.
In conclusion, in patients with stage 3 or higher CKD, Ramadan fasting during the summer months was associated with worsening of renal function. The clinical implication of this study is that the physicians need to alert patients regarding the potential adverse effects of fasting on kidney function. These patients needed to undergo close monitoring of their kidney function during Ramadan. Since Ramadan fasting is common among patients with chronic kidney disease, further research is needed in this area. Additional knowledge regarding how to identify those at increased risk of worsening of renal function during fasting would be valuable. More research is also required to determine how to monitor this population, so that evidence-based guidelines for management of these patients may be developed.
Acknowledgment
The authors gratefully acknowledge Ms. Aileen Esteibar, King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia for her secretarial assistance.
Footnotes
References
- 1.The Holy Qur’an. Madina (KSA): King Fahd Complex; 2005. Chapter 2:28. [Google Scholar]
- 2.The Holy Qur’an. Madina (KSA): King Fahd Complex; 2005. Chapter 2:28. [Google Scholar]
- 3.Unalacak M, Kara IH, Baltaci D, Erdem O, Bucaktepe PG. Effects of Ramadan fasting on biochemical and hematological parameters and cytokines in healthy and obese individuals. Metab Syndr Relat Disord. 2011;9:157–161. doi: 10.1089/met.2010.0084. [DOI] [PubMed] [Google Scholar]
- 4.Vardarli MC, Hammes HP, Vardarli İ. Possible metabolic impact of Ramadan fasting in healthy men. Turk J Med Sci. 2014;44:1010–1020. doi: 10.3906/sag-1308-30. [DOI] [PubMed] [Google Scholar]
- 5.Guerrero-Morilla R, Ramírez-Rodrigo J, Ruiz-Villaverde G, Sánchez-Caravaca MA, Pérez-Moreno BA, Villaverde-Gutiérrez C. [Endocrine-metabolic adjustments during Ramadan fasting in young athletes] Arch Latinoam Nutr. 2013;63:14–20. Spanish. [PubMed] [Google Scholar]
- 6.El-Wakil HS, Desoky I, Lotfy N, Adam AG. Fasting the month of Ramadan by Muslims: could it be injurious to their kidneys? Saudi J Kidney Dis Transpl. 2007;18:349–354. [PubMed] [Google Scholar]
- 7.Bernieh B, Al Hakim MR, Boobes Y, Abu Zidan FM. Fasting Ramadan in chronic kidney disease patients: Clinical and biochemical effects. Saudi J Kidney Dis Transpl. 2010;21:898–902. [PubMed] [Google Scholar]
- 8.Al Wakeel JS. Kidney function and metabolic profile of chronic kidney disease and hemodialysis patients during Ramadan fasting. Iran J Kidney Dis. 2014;8:321–328. [PubMed] [Google Scholar]
- 9.Mbarki H, Tazi N, Najdi A, Tachfouti N, Arrayhani M, Sqalli T. Effects of fasting during Ramadan on renal function of patients with chronic kidney disease. Saudi J Kidney Dis Transpl. 2015;26:320–324. doi: 10.4103/1319-2442.152494. [DOI] [PubMed] [Google Scholar]
- 10.Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–612. doi: 10.7326/0003-4819-150-9-200905050-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Berger ML, Dreyer N, Anderson F, Towse A, Sedrakyan A, Normand SL. Prospective observational studies to assess comparative effectiveness: the ISPOR good research practices task force report. Value Health. 2012;15:217–230. doi: 10.1016/j.jval.2011.12.010. [DOI] [PubMed] [Google Scholar]
- 12.Levey AS, Eckardt KU, Tsukamoto Y, Levin A, Coresh J, Rossert J, et al. Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO) Kidney Int. 2005;67:2089–2100. doi: 10.1111/j.1523-1755.2005.00365.x. [DOI] [PubMed] [Google Scholar]
- 13.American Diabetes Association. Standards of medical care in diabetes 2014. Diabetes Care. 2014;37(Suppl1):S14–S80. doi: 10.2337/dc14-S014. [DOI] [PubMed] [Google Scholar]
- 14.Kessler CS, Joudeh Y. Evaluation and Treatment of Severe Asymptomatic Hypertension. Am Fam Physician. 2010;81:470–476. [PubMed] [Google Scholar]
- 15.NasrAllah MM, Osman NA. Fasting during the month of Ramadan among patients with chronic kidney disease: renal and cardiovascular outcomes. Clin Kidney J. 2014;7:348–353. doi: 10.1093/ckj/sfu046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kellum JA, Lameire N, KDIGO AKI Guideline Work Group Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1) Crit Care. 2013;17:204. doi: 10.1186/cc11454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Haub C, Kaneda T. World Population Data Sheet. 2012. [Accessed 2016 November 7]. Available from: http://www.prb.org/Publications/Datasheets/2012/2012-world-population-data-sheet.aspx .
- 18.Samad F, Qazi F, Pervaiz MB, Kella DK, Mansoor M, Osmani BZ, et al. Effects of Ramadan Fasting on Blood Pressure in Normotensive Males. J Ayub Med Coll Abbottabad. 2015;27:338–342. [PubMed] [Google Scholar]
- 19.Norouzy A, Salehi M, Philippou E, Arabi H, Shiva F, Mehrnoosh S, et al. Effect of fasting in Ramadan on body composition and nutritional intake: a prospective study. J Hum Nutr Diet. 2013;26(Suppl1):97–104. doi: 10.1111/jhn.12042. [DOI] [PubMed] [Google Scholar]
- 20.Aksungar FB, Eren A, Ure S, Teskin O, Ates G. Effects of intermittent fasting on serum lipid levels, coagulation status and plasma homocysteine levels. Ann Nutr Metab. 2005;49:77–82. doi: 10.1159/000084739. [DOI] [PubMed] [Google Scholar]
- 21.Salti I, Bénard E, Detournay B, Bianchi-Biscay M, Le Brigand C, Voinet C, et al. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care. 2004;27:2306–2311. doi: 10.2337/diacare.27.10.2306. [DOI] [PubMed] [Google Scholar]
- 22.Gifford JD, Rutsky EA, Kirk KA, McDaniel HG. Control of serum potassium during fasting in patients with end-stage renal disease. Kidney Int. 1989;35:90–94. doi: 10.1038/ki.1989.12. [DOI] [PubMed] [Google Scholar]