

Abstract
Objectives:
To assess the effect of wet cupping on health-related quality of life (HRQOL) of adult patients with chronic medical conditions, who were referred to the Cupping Clinic of King Abdulaziz University Hospital (KAUH), Jeddah, Kingdom of Saudi Arabia.
Methods:
A controlled, quasi-experimental study design was carried out among 629 patients referred for cupping from the KAUH Specialty Clinics, during the period from January to December 2014. Patients in the intervention group (309 patients) completed a pre-test included WHO quality of life-BREF, received one wet-cupping session, and filled-out the post-test (1 month later). Patients in the control group (320 patients) completed the pre-test during their enrollment in the study and post-test one month later. Both groups received their ordinary treatment. Descriptive and inferential statistics were performed.
Results:
Pain was the most common cause for cupping referral. After cupping intervention, the mean scores of most of the HRQOL domains, especially the physical domain, improved significantly among patients in the intervention group. The mean total score of physical HRQOL domain was 61.6 ± 13.6 before cupping, and reached 69.7 ± 12.6 after intervention (paired t-test=11.3, p=0.000). Improvements in HRQOL were noticed for almost all types of pain and other medical conditions.
Conclusion:
There are promising effects in favor of using wet cupping for improving HRQOL of patients with chronic conditions. Cupping is recommended as a complementary treatment modality for chronic medical conditions, especially pain.
Nowadays, there is a growing interest in the field of complementary and alternative medicine (CAM). This discipline includes a diverse set of approaches used for prevention and treatment of many diseases.1 Several benefits of CAM have been proven, and it may be considered an effective modality for disease prevention, treatment of non-communicable diseases (NCDs), and for improving the quality of life (QOL) of individuals with chronic medical conditions.2 Many patients who may not be satisfied with the outcomes of modern medicine, particularly those with chronic diseases, may be satisfied with the outcomes of CAM.3 Pain is the most common reason for seeking therapeutic alternatives of conventional medicine. Cupping, wet or dry, is an ancient treatment, which was broadly utilized in several communities, and it was recommended by the Islamic society.4 Wet cupping (Hijama) is an old medical technique, which has been broadly applied for treatment of numerous conditions, such as acute/chronic inflammation, communicable diseases, and the immune system diseases.5 Nowadays, the interest in conventional cupping has been escalated with the increasing evidence that it may be effective in decreasing different types of pain. In cupping, a glass cup is used to create suction over a painful part, after making skin incisions. It has been postulated that suction of the “congested” blood out of the skin will improve both lymphatic and blood circulation, hence relieve pain.4,6 Cupping has been used for the treatment and cure of a wide range of conditions, such as hematological disorders, rheumatic conditions, arthritis, sciatica, and back pain. It can be also used for anxiety, and other physical and mental conditions.6 Furthermore, cupping may be effective for migraine, tension headaches,4 post-herpetic pain,7 and other clinical conditions. Kim et al8 conducted a systematic review on the use of cupping for treating pain and reported that the rate of using alternative therapies increased with increasing the pain severity.8 Furthermore, Farhadi et al9 reported that compared with the standard care, cupping therapy significantly decreased pain, functional disability, and the use of pain medications within 3 months after treatment of their patients with low back pain. Health-related quality of life (HRQOL) refers to the perceptions of wellbeing, well-functioning, life satisfaction, and being healthy. Nowadays, HRQOL has been increasingly utilized as a parameter for evaluation of various treatment outcomes.10 Despite the growing evidence of the effects of wet cupping in many diseases, few intervention studies were carried out on its effect on chronic medical conditions. These researches were carried out on small samples and mainly addressed the non-specific pain.6,9,11 No adequate interventional studies has been conducted to assess the effects of wet cupping on different chronic medical conditions in Jeddah, Kingdom of Saudi Arabia (KSA). Similarly, no interventional study has described the effects of wet cupping on the HRQOL of patients with chronic medical conditions. There are unanswered questions about such areas of cupping research. So, a comprehensive intervention epidemiological study is therefore warranted to evaluate the effects of wet cupping on such patients, particularly its effect on their HRQOL. The objective of the current study was to assess the effects of wet cupping on the HRQOL of patients with chronic medical conditions who were referred to the cupping clinic from different specialty clinics at the King Abdulaziz University Hospital (KAUH), Jeddah, KSA.
Methods
Ethical statement
The study was carried out according to the ethical principles of Helsinki Declaration. The Committees of the Faculty of Medicine and King Abdulaziz University (KAU), Jeddah, KSA approved the initiation of the Cupping Clinic, as an outpatient clinic in KAUH. The proposal of the current intervention study was approved by the Institutional Review Board (IRB) of KAUH. The trials was successfully registered in the World Health Organization Clinical Trials Registrant (Registration Number: IRCT2015050322060N1).
The study adhered also to the principles of the WHO Code for the Responsible Conduct of Research. The study assured the confidentiality and freedom to participate in the research. A written informed consent was obtained from each participant upon enrollment in the study. All enrolled patients in the study received their usual ordinary treatment. All administrative approvals were obtained.
Searching strategy
Studies performed for evaluation of the effects of cupping therapy on chronic medical conditions, and those assessed its effect on HRQOL were searched and scrutinized. Electronic databases of PubMed, Google Scholar, Google, and Cochrane library were explored for the published researches from 2000 to 2015.
Study setting and location
The study was conducted at the Cupping Clinic of KAUH, Jeddah, KSA.
Study design
A non-randomized, controlled, prospective, quasi-experimental study design was carried out. Eligible subjects were allocated either to the intervention group or to the control group according to their referral number (to the Cupping Clinic). Patients in the control group filled-out the data collection sheet at the time of their enrollment in the study, and one month later (without receiving cupping). On the other hand, patients in the intervention group completed the pre-test assessments, received the intervention of a single wet cupping therapy, and then filled out the post-test HRQOL assessment (1 month later).
Patients and sampling
The target population was adult patients with chronic medical conditions who were referred to Yousef Abdul-Latif Jameel Cupping Clinic from different specialty clinics of KAUH. The study was performed during a one year period from January 2014 until the end of December 2014. All patients referred to the Clinic and fulfilled the eligibility criteria during this period, were included. A total of 629 eligible participants enrolled in the study; 309 participants were assigned to the intervention wet cupping group and 320 patients to the control group.
Inclusion criteria
All adult male and female patients aged 18-60 years referred to the Cupping Clinic from different speciality clinics of KAUH, referred with chronic medical conditions (disease lasting 3 months or more), completely understood the research process, accepted to participate, and was willing to sign the study written informed consent (after reading the protocol and accepting it).
Exclusion criteria
Patients were excluded from the study if they did not fulfill the eligibility criteria, did not accept to comply with the study protocol, and/or had mental illnesses that could interfere with study completion.
Pre-test assessments
Upon enrollment, each eligible participant (from both groups) completed a confidential, validated, interviewing data collection sheet. It asked regarding personal and socio-demographic data. They also inquired regarding their medical condition, presence of pain, and the type of it (if present). The HRQOL was assessed using the World Health Organization Quality of Life-BREF (WHOQOL-BREF). The WHOQOL-BREF instrument contains 26 questions; 2 general questions and 24 items used to assess the 4 HRQOL domains. Those domains are the physical health, the psychological health, the social relationships, and the environmental domains. The internal consistency reliability of WHOQOL-BREF and its 4 domains ranged from 0.66-0.92. The content validity, construct validity, and reliability of the WHOQOL-BREF were reported to be good.12,13
Intervention
Patients in the intervention group received a single session of wet cupping intervention. Cupping was performed by expert certified physicians, who regularly performed cupping in the clinical setting. The patient took a sitting position or lying position according to the affected site fully exploring the positions for bloodletting. The local hair of the patient was cut-off and then cupping was applied to the related points for 5-10 minutes. The physician wore sterilized gloves and a face mask. A mono-use surgical blade was used to superficially cut the skin (inside each of the cupping marks for about 10 cuts). The patients’ pain diagram and physical examination were used to identify the painful areas and the big geloses of the sub-skin.6 After the cup was removed, the mouth and internal wall of the cup were sterilized with 75% alcohol. Cupping was performed again at the local parts, with blood drawn into the cup. After 5-10 minutes, the blood in the cup became solid, the cup with the blood was removed and the skin was cleaned with 75% alcohol. The wounds were sterilized with 2% iodine, covered with gauze, and fixed with adhesive plaster for 24 hours.14
Post-test assessments
Patients from both intervention and control groups of the study completed the same data collection sheet, filled in the pre-test, one month after their enrollment in the study (1 month after cupping therapy for patients in the intervention group). Figure 1 presents the Consort flow diagram of the study design. Most of the patients came back for the post-test (very small loss of follow up), as they routinely came to the hospital every month to receive the ordinary treatment from the hospital.
Figure 1.
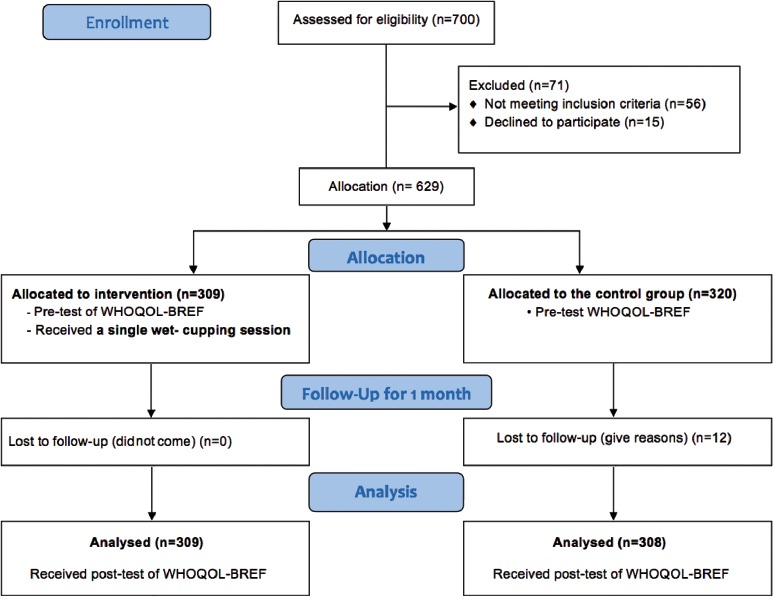
Consort flow diagram of the study design of wet cupping quasi-experimental design among patients with chronic medical conditions, King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia. WHOQOL - World Health Organization Quality of Life
Outcome measures Primary outcome
Changes (improvement) in the scores of WHOQOL-BREF domains 13 from the baseline level (before cupping) until one month after cupping (post-intervention).
Secondary outcome
Changes (improvement) in the scores of WHOQOL-BREF13 domains among patients in the intervention group compared with those in the control group, at the end of the study.
Statistical analysis
Data were analysed using the Statistical Package for Social Sciences version 20 (IBM Corp., Armonk, NY, USA). Descriptive and inferential statistics were performed. Descriptive statistics were performed in the form of frequency tables, means and standard deviations. As the data were normally distributed, paired t-tests were used to compare between means of the 4 different HRQOL domain scores before and after cupping. Student’s t-test was used for comparison between the mean scores of QOL domains of patients in the intervention group and those in the control group, at the end of the study. Student’s t-test and Chi-square tests were used for comparison of the baseline characteristics of both groups. Box and Whisker Plot was used to compare between different HRQOL domains before and after cupping. A p-value of <0.05 was considered statistically significant.
Results
A total of 629 patients enrolled in the study, and the mean age of all participants was 44.18 ± 13.53 years. Pain was the most common cause (70.6%) of referral to the Cupping Clinic among all patients from both groups (n=444 out of 629). Table 1 shows comparisons between the baseline characteristics of the patients enrolled in the intervention and the control group, at the start of the study. No statistical significant differences were found between patients from both groups regarding age, gender, marital status and presence of pain. The mean age of the participants in the intervention group was 44.32 ± 13.54 and the corresponding mean age among the control group was 44.03 ± 13.55, with no statistical significant difference (Student’s t-test=0.026, p=0.79).
Table 1.
The baseline characteristics of patients with chronic medical conditions in both the intervention (cupping) group and control group, at King Abdulaziz University Hospital.
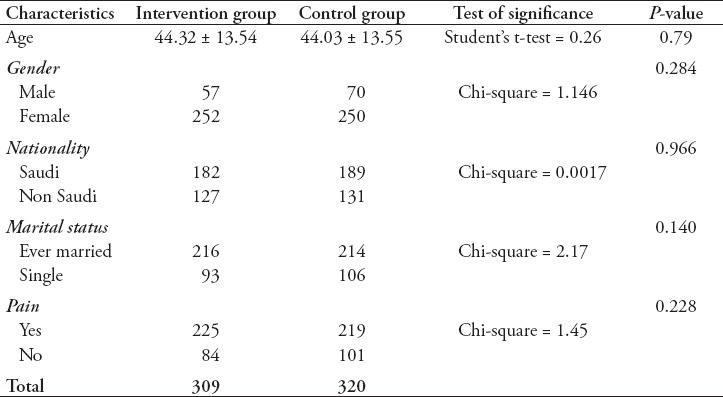
Table 2 shows that among patients in the intervention group, pain was the most common cause (72.8%) of referral to the Cupping Clinic, followed by headache (16.2%), infertility (7.1%) and allergy (5.2%). Each of the hypertension and diabetes mellitus represented 4.9% of the referral causes.
Table 2.
Causes for referral to Cupping Clinic among patients in the intervention group, who received cupping therapy.
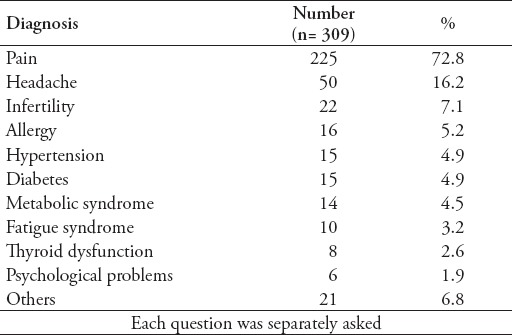
Figure 2 illustrates the types of pain among patients, who suffered from it in the intervention group. The most frequently reported types of pain were joint pain (48.4%), back pain (43.1%), neck and shoulder pain (26.2%), and pain related to peripheral neuropathy (8.4%).
Figure 2.
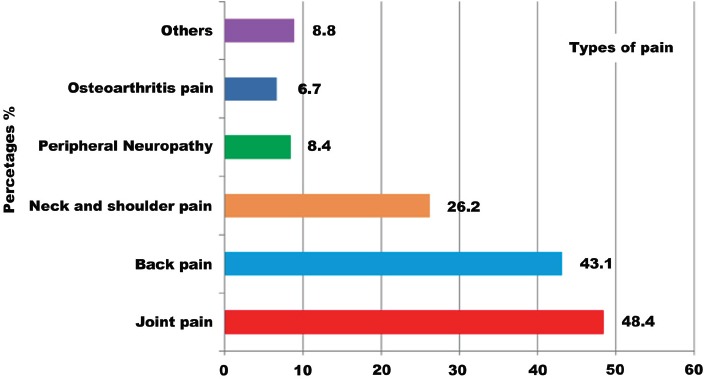
Types of pain among the patients who received cupping therapy intervention at King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia.
Table 3 illustrates comparisons between mean scores of the 4 HRQOL domains of participants enrolled in the intervention and those enrolled in the control group (at the end of the study). It is apparent from the table that patients assigned to the intervention group reported higher scores of all HRQOL domains compared with the controls. The mean score of the physical HRQOL domain was 69.7 ± 12.6 among participants received wet cupping intervention compared with 64.7 ± 15.9 among those in the control group. A highly statistical significant difference was present (Student’s t-test=3.59, p<0.001). Similarly, a highly statistical significant difference was found between the 2 groups regarding the mean score of the social HRQOL domain. On the other hand, no statistical significant differences were found between both groups regarding the scores of the psychological and environment HRQOL domains.
Table 3.
Comparisons between the scores of the quality of life (QOL) domains of patients in the control and intervention groups after one month of cupping.
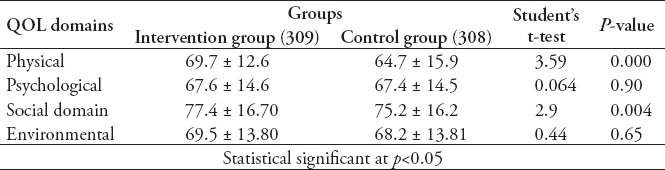
Figure 3 illustrates the box-plots of the changes in the scores of the 4 HRQOL domains after cupping compared with the baseline scores (among patients who received cupping). The scores of all domains improved after cupping therapy, and the greatest improvement was observed in the physical health domain (the median score was 61.6 before cupping and reached 69.7 after cupping), followed by the psychological health, environmental domains, and lastly the social relationships domain.
Figure 3.
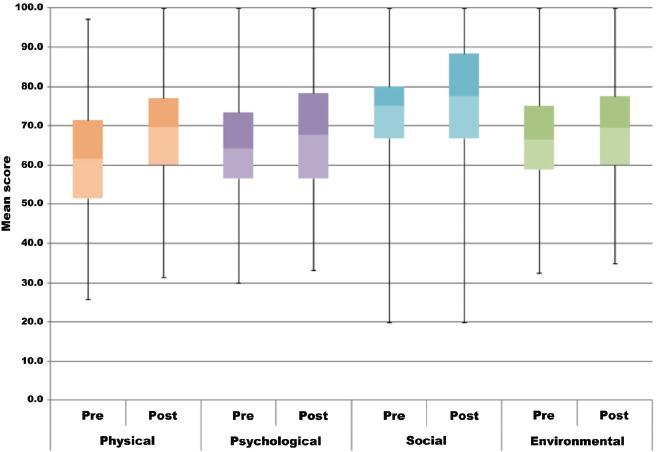
Box-plots of changes in the scores of 4 quality of life domains before and after cupping therapy among patients with chronic medical conditions at King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia. All pairwise p-values were <0.05.
Table 4A & B illustrates the changes in the mean scores of the 4 HRQOL domains after cupping compared with the pre-test levels, according to the study variables. The mean score of the physical HRQOL domain was 61.6 ± 13.6 before cupping, and improved to reach a mean of 69.7 ± 12.6 after intervention (paired t-test=11.3, p=0.000). Similarly, there are significant improvements in the mean scores of the all of the psychological, social, and environmental domains after cupping compared with the levels before it (p<0.01). Regarding gender, women demonstrated significantly better scores (p<0.01) across almost all 4 HRQOL domains after Hijama. On the other hand, men showed significant improvement only in the physical HRQOL score (p<0.01), after cupping. Concerning nationality, Saudis demonstrated better scores for the physical health and environmental domains after cupping. Furthermore, single patients showed a significant improvement across all HRQOL domains, while married patients showed significantly better scores for physical health, psychological health, and environmental domains. With regards to education, patients who held a University degree or above demonstrated significant improvements across all domains of the HRQOL scores. Compared with non-smokers, who showed significantly improved HRQOL scores across all 4 domains, smokers showed a significant improvement only in the psychological health domain.
Table 4A.
Changes in the scores of the physical and psychological quality of life domains before and after cupping therapy among patients with chronic medical conditions in the intervention group, according to study variables.
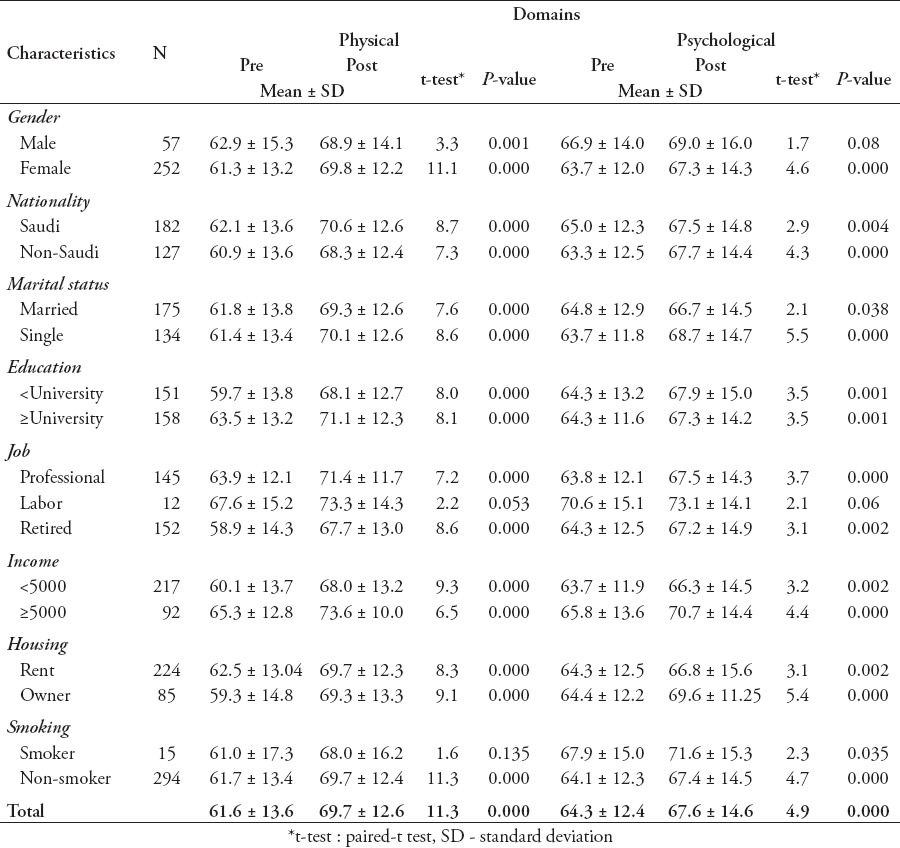
Table 4B.
Changes in the scores of the social and environmental quality of life domains before and after cupping therapy among patients with chronic medical conditions in the intervention group, according to study variables.
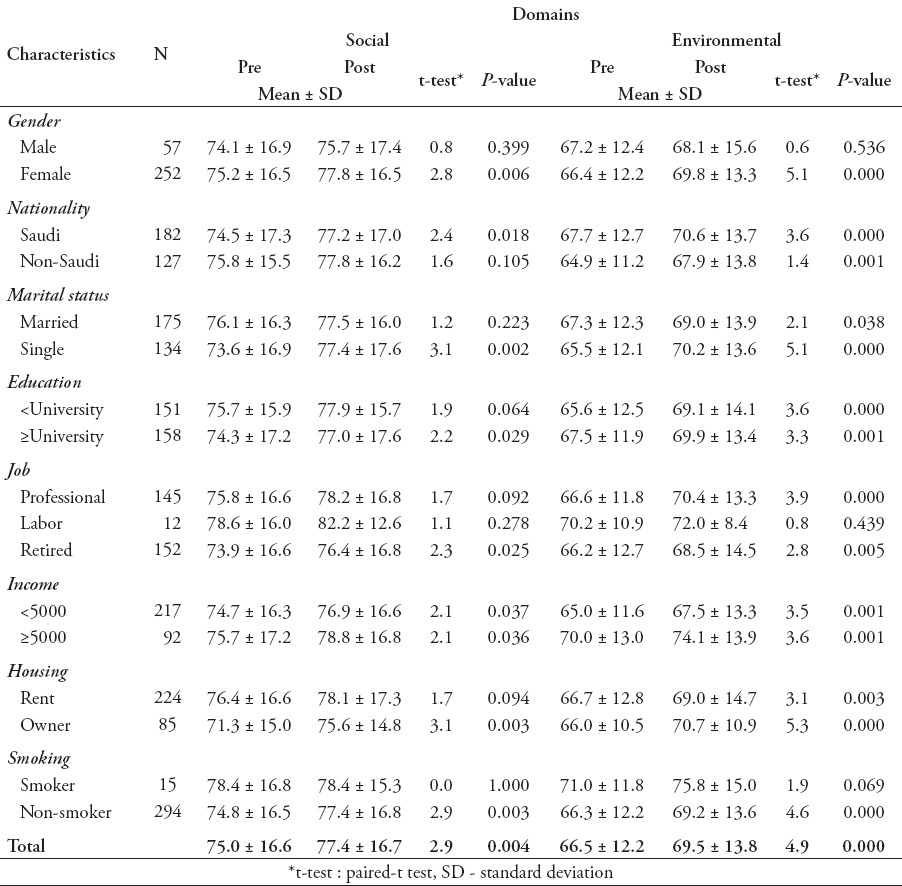
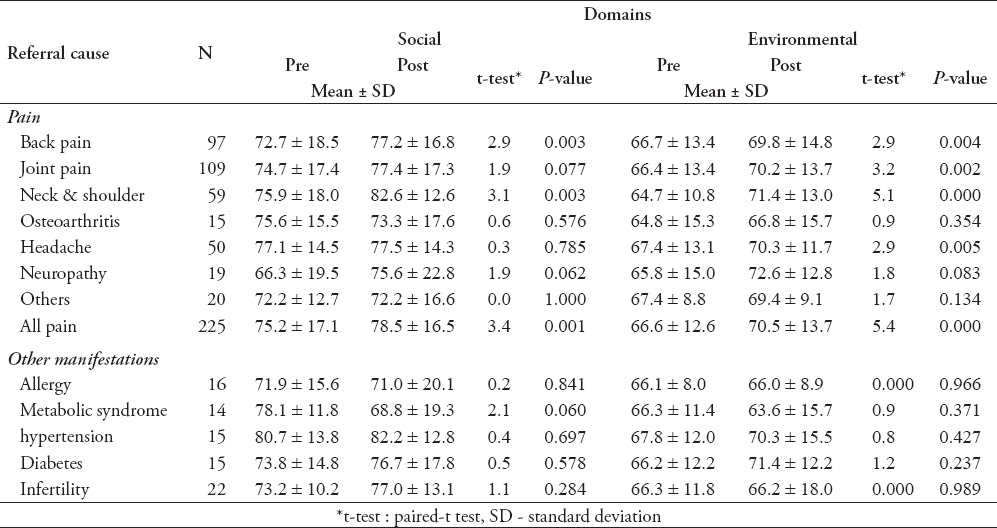
Table 5A & B shows that after receiving wet-cupping (Hijama) intervention, patients with almost all types of pain (except the pain related to osteoarthritis) reported significant improvements in the mean scores of the physical HRQOL domain compared with their baseline levels (p<0.001). Among patients who complained from headache, the mean score of physical function was 60.7 ± 14.9 before cupping and improved to reach 69.7 ± 10.2 after cupping (paired t -test=5.1, p<0.001). Correspondingly, the mean score of the psychological domain of all patients suffering from pain was 65.3 ± 12.4 before, and 69.1 ± 14.3 and after cupping intervention (paired t-test=5.2, p<0.001). Similarly, patients with almost all types of chronic medical conditions (except the metabolic syndrome) reported significant increases in the mean scores of the physical HRQOL after cupping compared with their reported scores before intervention. Similar associations were also observed regarding most of the other 3 HRQOL domains before and after cupping.
Table 5A.
Changes in the scores of the physical and psychological quality of life domains before and after cupping intervention according to the type of pain and medical condition among patients in the intervention group.
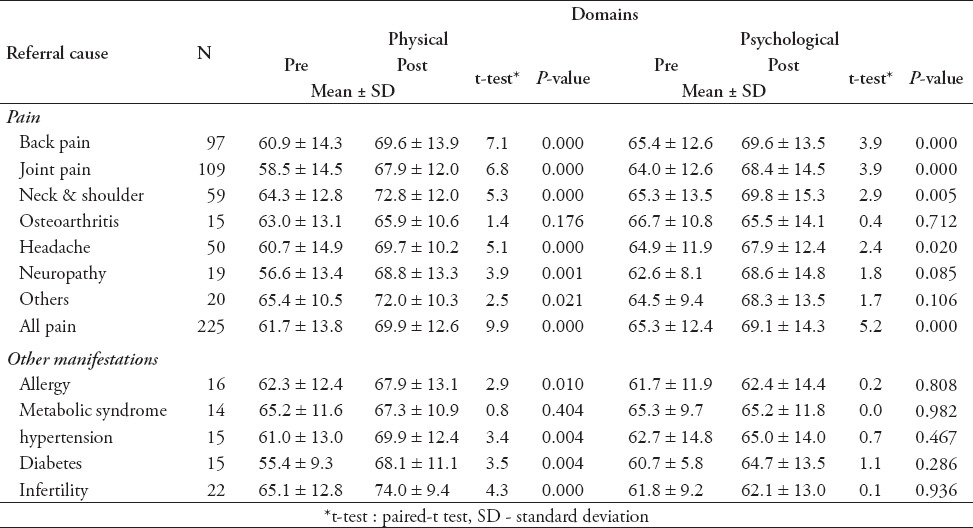
Table 5B.
Changes in the scores of the social and environmental quality of life domains before and after cupping intervention according to the type of pain and medical condition among patients in the intervention group.
Benefits and harm from the study
The benefit of cupping was apparent in improving the 4 different domains of HRQOL (especially the physical domain) after one month of receiving cupping. There was improvement in HRQOL of patients suffering from almost all types of pain and other chronic medical conditions. None of the participants complained or reported any adverse events after the cupping therapy.
Discussion
This study used the WHOQOL-BREF to identify the effects of wet cupping on HRQOL among a large sample of patients with different chronic medical conditions in Jeddah, KSA. This tool was found to be suitable for evaluating the effectiveness of the therapy (as it is an objective not a subjective assessment).13
Chronic pain is a common and universal symptom that occurs in all ages from all populations. Musculoskeletal pain and headache are possibly the most predominant types of chronic pain.15 It is the most common reason for seeking therapeutic alternatives of conventional medicine.16 Wet cupping has been used for the treatment of pain and several other conditions for many decades.6 This agrees with the results of the current study, as pain management was the most common cause of referral of our patients referred to the cupping clinic and those who received cupping intervention.
Analysis of the clinical studies published in the last decades revealed that cupping is an effective modality for pain management.16,17 Our study also revealed that after the wet cupping therapy there was a significant increase in the scores of physical HRQOL domain, and other domains, among patients who suffered from different types of pain. Our results agreed with those of Lauche et al,18 who reported that a series of cupping treatments significantly increased the scores for the physical function and QOL of patients with chronic non-specific neck pain in Tromsø, Norway. In 2012, they also reported that a single session of conventional cupping was found to be an effective treatment for improving pain and QOL (particularly physical function) in patients with chronic non-specific neck pain.6 Another study conducted in Iran9 found that conventional wet cupping performed in a primary care setting was safe and acceptable for patients with non-specific low back pain. In South Korea,11 a pilot study conducted for 32 participants provided preliminary data on the effectiveness and safety of wet cupping for pain management. However, their results included a small pilot sample.
Patients with headache who received cupping intervention in the current study reported significantly better scores of most of HRQOL domains after cupping, especially the physical domain. These results agrees with the findings of Ahmadi et al.4 Furthermore, Teut et al19 conducted a randomized controlled, exploratory pilot study to investigate the effectiveness of cupping therapy among 21 patients with pain of knee osteoarthritis. Their results showed significantly better component scores of the short form 36 of the physical domain in the cupping group than for the control group. In the current study, the score of the physical domain of HRQOL improved after cupping among patients with osteoarthritis pain, but without statistical significant difference. On the other hand, our study showed significant improvement in HRQOL scores of patients with chronic joint pain in general.
The current controlled quasi-experimental intervention study succeeded in improving the HRQOL of patients with chronic medical conductions referred to the cupping clinics compared with before performing it, and compared with the control group. The external validity of the current quasi-experimental clinical trial is considered good due to its large sample size (compared with other studies), fair length of follow-up, the university hospital setting, and involving many types of chronic medical conditions.
The findings of our trial responded to the study’s research objectives. This study has a programmatic and policy implication of the need to apply wet cupping as a complementary treatment, for treatment of clinical medical conditions, especially pain in the university hospitals. The implications of our findings for future research are based on the need to conduct big randomized clinical trials to assess HRQOL for patients with each chronic medical conditions, separately. The number of cupping sessions can be increased and the follow period can become longer. The limitation of the study is that there was no randomization. The main barrier of the study was the presence of a large number of referred patients to the clinic.
In conclusion, pain was the most common cause of referral to the Cupping Clinic. Wet cupping (Hijama) intervention improved most of the HRQOL domains of the adult patients with chronic medical conditions. Improvements were present after one month of intervention compared with their baseline scores. After cupping, the mean scores of most of the HRQOL domains, especially the physical function domain, improved significantly among patients who complained from almost all types of pain (except osteoarthritis pain), and among those who complained from most of the chronic medical conditions (except the metabolic syndrome). Furthermore, cupping was more effective among women and non-smokers compared with others. Post-test findings showed presence of significant improvements in the scores of the physical and social HRQOL domains among patients who received cupping intervention compared with those in the control group who did not receive cupping. Finally, the study added that there are promising effects in favor of using wet cupping for improving HRQOL of patients with chronic conditions. Cupping is recommended to be used as a complementary treatment modality for chronic medical conditions, which agrees with recomendations from Hadith.20
Acknowledgment
The authors would like to thank Sheikh Yousef Abdul Latif Jameel Scientific Chair and all doctors, nurses, and co-workers at the Hijama Clinic, and special thanks to our colleagues Prof. Mohsen Abdul Elalah, Dr. Amal Obied, Dr. Anhar Gazzaz, Dr. Manal Dahalawi, Dr. Mohammad Al Farrah, Dr. Asmaa, Ms. Rasha Ramadan, Ms. Zakia, Ms. Sabreen, Ms. Zahra, Mr. Mohammad Jumaah, Ms. Reham, Ms. Susana de Guzman, and Mr. Kelvin from King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia.
This study was funded by Sheikh Yousef Abdul Latif Jameel Prophetic Medicine Scientific Chair, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia (Grant No. MBK/5/437).
Footnotes
References
- 1.Kummet CM, Spector ML, Dawson DV, Fischer M, Holmes DC, Warren J, et al. Patterns of complementary and alternative medicine (CAM) use among dental patients. J Public Health Dent. 2015;75:109–117. doi: 10.1111/jphd.12078. [DOI] [PubMed] [Google Scholar]
- 2.Refaat B, El-Shemi AG, Ebid AA, Ashshi A, BaSalamah MA. Islamic Wet Cupping and Risk Factors of Cardiovascular Diseases: Effects on Blood Pressure, Metabolic Profile and Serum Electrolytes in Healthy Young Adult Men. Alternative & Integrative Medicine. 2014;3:1–7. [Google Scholar]
- 3.Bhalerao MS, Bolshete PM, Swar BD, Bangera TA, Kolhe VR, Tambe MJ, et al. Use of and satisfaction with complementary and alternative medicine in four chronic diseases: a cross-sectional study from India. Natl Med J India. 2013;26:75–78. [PubMed] [Google Scholar]
- 4.Ahmadi A, Schwebel DC, Rezaei M. The efficacy of wet-cupping in the treatment of tension and migraine headache. Am J Chin Med. 2008;36:37–44. doi: 10.1142/S0192415X08005564. [DOI] [PubMed] [Google Scholar]
- 5.Mehta P, Dhapte V. upping therapy: A prudent remedy for a plethora of medical ailments. J Trad Complement Med. 2015;5:127–134. doi: 10.1016/j.jtcme.2014.11.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lauche R, Cramer H, Hohmann C, Choi KE, Rampp T, Saha FJ, et al. The effect of traditional cupping on pain and mechanical thresholds in patients with chronic nonspecific neck pain: a randomised controlled pilot study. Evid Based Complement Alternat Med. 2012;2012:429718. doi: 10.1155/2012/429718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cao H, Zhu C, Liu J. Wet cupping therapy for treatment of herpes zoster: a systematic review of randomized controlled trials. Altern Ther Health Med. 2010;16:48–54. [PMC free article] [PubMed] [Google Scholar]
- 8.Kim JI, Lee MS, Lee DH, Boddy K, Ernst E. Cupping for treating pain: a systematic review. Evid Based Complement Alternat Med. 2011;2011:467014. doi: 10.1093/ecam/nep035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Farhadi K, Schwebel DC, Saeb M, Choubsaz M, Mohammadi R, Ahmadi A. The effectiveness of wet-cupping for nonspecific low back pain in Iran: a randomized controlled trial. Complement Ther Med. 2009;17:9–15. doi: 10.1016/j.ctim.2008.05.003. [DOI] [PubMed] [Google Scholar]
- 10.Barcaccia B, Esposito G, Matarese M, Bertolaso M, Elvira M, De Marinis MG. Defining Quality of Life: A Wild-Goose Chase? Europe’s Journal of Psychology. 2013;9:185–203. [Google Scholar]
- 11.Kim JI, Kim TH, Lee MS, Kang JW, Kim KH, Choi JY, et al. Evaluation of wet-cupping therapy for persistent non-specific low back pain: a randomised, waiting-list controlled, open-label, parallel-group pilot trial. Trials. 2011;12:146. doi: 10.1186/1745-6215-12-146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Trompenaars FJ, Masthoff ED, Van Heck GL, Hodiamont PP, De Vries J. Content validity, construct validity, and reliability of the WHOQOL-Bref in a population of Dutch adult psychiatric outpatients. Qual Life Res. 2005;14:151–160. doi: 10.1007/s11136-004-0787-x. [DOI] [PubMed] [Google Scholar]
- 13.Skevington SM, Lotfy M, O’Connell KA, WHOQOL Group The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual life Res. 2004;13:299–310. doi: 10.1023/B:QURE.0000018486.91360.00. [DOI] [PubMed] [Google Scholar]
- 14.Huang YL. [Cupping-bloodletting therapy of Saudi Arabia and its clinical application] Zhongguo Zhen Jiu. 2008;28:375–377. Chinese. [PubMed] [Google Scholar]
- 15.Toye F, Seers K, Allcock N, Briggs M, Carr E, Andrews J, et al. Patients’ experiences of chronic non-malignant musculoskeletal pain: a qualitative systematic review. Br J Gen Pract. 2013;63:e829–e841. doi: 10.3399/bjgp13X675412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cao H, Han M, Li X, Dong S, Shang Y, Wang Q, et al. Clinical research evidence of cupping therapy in China: a systematic literature review. BMC Complement Altern Med. 2010;10:70. doi: 10.1186/1472-6882-10-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cao HJ, Liu JP, Hu H, Wang NS. Using a partially randomized patient preference study design to evaluate the therapeutic effect of acupuncture and cupping therapy for fibromyalgia: study protocol for a partially randomized controlled trial. Trials. 2014;15:280. doi: 10.1186/1745-6215-15-280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lauche R, Cramer H, Langhorst J, Dobos G. Cupping for chronic nonspecific neck pain: a 2-year follow-up. Forsch Komplementmed. 2013;20:328–333. doi: 10.1159/000355634. [DOI] [PubMed] [Google Scholar]
- 19.Teut M, Kaiser S, Ortiz M, Roll S, Binting S, Willich SN, et al. Pulsatile dry cupping in patients with osteoarthritis of the knee - a randomized controlled exploratory trial. BMC Complement Altern Med. 2012;12:184. doi: 10.1186/1472-6882-12-184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Al-Bukhari M. Sahih Al-Bukhari. Hadith No. 5758. [Google Scholar]