

Sir,
Armored endotracheal tube (ETT) has reinforced metal coils which make it less likely to get obstructed.[1] Therefore, it is preferred for head and neck surgeries. Airway obstruction due to occlusion of armored ETT lumen after being bitten by patient is well known.[2] Postoperatively, the orally intubated armored ETT has to be replaced with polyvinyl chloride (PVC) ETT to prevent partial or total airway obstruction caused by biting. However, in patients who were intubated nasally with armored ETT, there is no risk of patient biting it. In such patients, postoperative ventilation can be continued with the nasal armored ETT till neurological recovery is adequate, and the airway edema subsides. Assessment of ETT tip in bedside chest radiography is different in PVC and armored tubes. PVC ETT has a radiopaque line till its tip which will be visualized in radiography [Figure 1]. However, armored ETT does not have any radiopaque line, and it is identified only by the radiopaque armored metal rings in radiography. These metal rings do not reach till the tip of ETT. Tip of armored ETT extends approximately 1.5–2 cm beyond the distal most radiopaque metal ring visualized in radiography [Figure 2]. In Figure 3 where ETT tip appears to be correctly placed well above the carina, if we consider the distal metal ring as the ETT tip. However, if we take into account the extra 1.5–2 cm from the distal most radiopaque metal ring, the ETT tip may be very close to carina or even beyond it. Unlike PACS system, digital X-rays have to be interpreted carefully while measuring the distance from ETT tip to carina as length measured in the film may not correspond to true length because of zooming effect. While using a PACS system, picture exposure can be adjusted, and even the lesser radiopaque part of ETT distal to the metal rings can be appreciated. When radiography is inconclusive, fiber-optic bronchoscope can be used to confirm the position of armored ETT tip.
Figure 1.
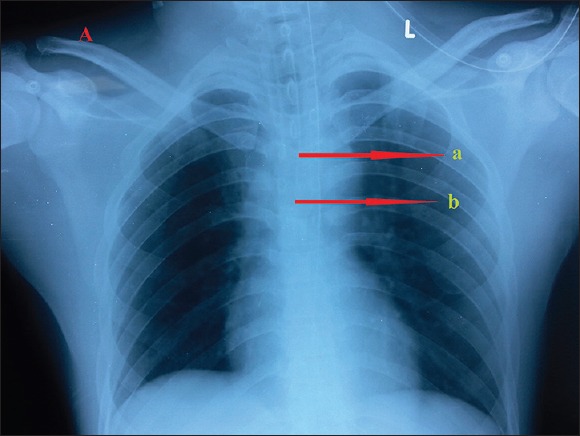
A chest radiography with polyvinyl chloride endotracheal tube in place. Arrow “a” is placed at the distal end of radiopaque line which will correspond to endotracheal tube tip. Arrow “b” is placed at carina.
Figure 2.
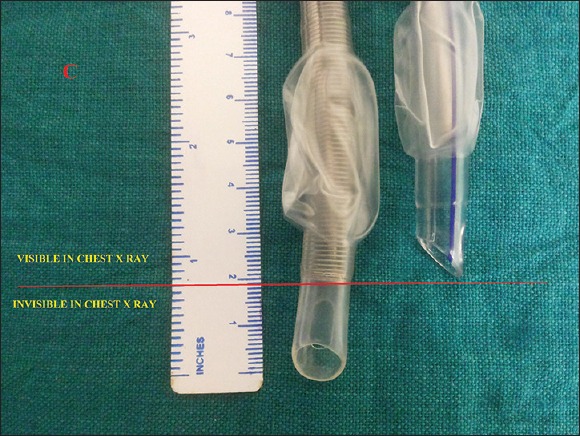
Tip of armored endotracheal tube is 2 cm distal to the distal most metal ring, and this portion may not be visualized in radiography.
Figure 3.
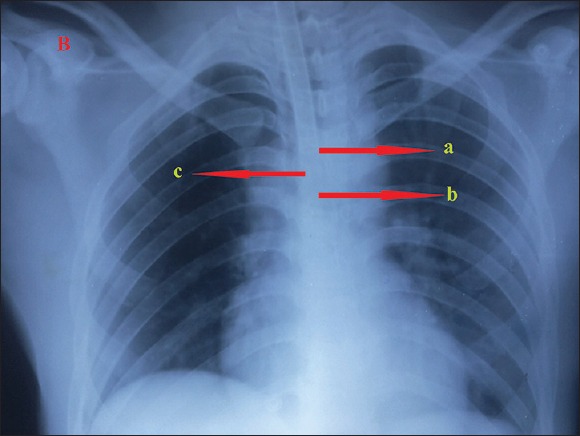
Chest radiography with an armored endotracheal tube in place. Arrow “a” is marked at the distal most radiopaque metal ring. Arrow “b” is marked at the carina. Arrow “c” represents the possible position of the endotracheal tube tip which is very close to the carina.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.King HK. Pharyngeal obstruction of a reinforced orotracheal tube. Anesth Analg. 1999;89:261. doi: 10.1097/00000539-199907000-00062. [DOI] [PubMed] [Google Scholar]
- 2.King KP, Stolp BW, Borel CO. Damage to an armored endotracheal tube introduced via the intubating laryngeal mask airway induced by biting. Anesth Analg. 1999;89:1324–5. [PubMed] [Google Scholar]