

Abstract
Objectives: This study examined the longitudinal associations of objectively measured physical activity, sedentary behavior, and diet quality with two measures of adiposity and a measure of weight status.
Methods: A total of 658 children from 21 elementary schools (45.1% boys; 40% white, 33% black, 9% Hispanic, and 18% other race/ethnicity) were assessed at least twice in fifth, sixth, and/or seventh grade. Fat mass index (FMI), percent body fat (PBF), and BMI were calculated from body weight, standing and seated heights, and bioelectrical impedance (BIA) measured each year.
Results: At follow-up, both FMI and PBF decreased among boys and increased among girls, while BMI increased in both boys and girls. After controlling for race/ethnicity, parent education, and maturity offset at baseline, growth curve analyses showed that moderate-to-vigorous physical activity (MVPA) was significantly and negatively associated with FMI, PBF, and BMI for both boys and girls. After forming tertiles of fifth grade MVPA, least-square means for FMI, PBF, and BMI were examined by grade and gender. For both boys and girls, higher MVPA was associated with lower FMI, PBF, and BMI at all three grade levels. The relationships between sedentary behavior and diet quality and FMI, PBF, and BMI were not consistent for boys or girls.
Conclusions: As boys and girls transitioned from elementary to middle school, children who participated in higher levels of MVPA maintained more favorable levels of two indicators of adiposity and a measure of weight status. These findings support the need for interventions to help children meet current public health guidelines for physical activity.
Keywords: : dietary intake, obesity, physical activity
Introduction
Rates of overweight and obesity increased dramatically in American children and youth between the 1970s and the 2000s.1,2 Despite signs of plateauing in some age groups, recent surveys indicate that the prevalence of obesity has continued to increase in US adolescents.2 There is broad agreement that these disquieting trends have resulted from multiple secular changes in American society,3 and it is clear that there are important short- and long-term health risks associated with excessive weight during childhood.4,5 For that reason, numerous authoritative organizations have recommended that steps be taken to prevent excessive weight gain during childhood and adolescence. These recommendations have consistently emphasized the need to promote healthy eating and physical activity in young people.6–9
While the need to prevent obesity in US youth is now recognized as an important societal goal,10 actions in the healthcare sector have focused primarily on treating existing childhood obesity rather than preventing the condition.11,12 In the public health and education sectors, professionals have mounted numerous initiatives aimed at preventing childhood obesity; however, few of those initiatives have succeeded in producing reductions in the prevalence of overweight and obesity in targeted groups.13 A key factor that limits the effectiveness of prevention efforts is a lack of research that identifies the modifiable factors that underlie excessive weight gain in children and youth. If those factors were well understood, public health interventions could be focused on addressing the precursors to overweight and obesity.14,15
Some previous studies have utilized prospective longitudinal designs to examine factors that may underlie excessive weight gain in young people.16–18 However, the number of such studies is modest, and the methods used in those studies have been highly variable.16–18 Many of the studies have included measures of physical activity and dietary behavior. Some studies have examined sedentary behavior as well as physical activity, but were limited by the use of self-report measures.19 BMI frequently was used as the measure of weight status,16 but in developing children, change in BMI may not be an accurate indicator of change in adiposity.20,21
This diversity in study methods is exemplified by two investigations, both of which used prospective observational designs with sizable cohorts.19,22 Fulton et al.19 followed more than 400 children and adolescents for 4 years and measured weight-related outcomes with bioelectrical impedance. Developmental status was assessed by Tanner staging, and estimated energy intake was considered in their statistical models. However, this study's protocol was limited by the use of self-report measures of physical activity and sedentary behavior. In contrast, Mitchell et al.,22 following more than 700 children between ages 9 and 15 years, used objective measurement of physical activity and sedentary behavior and included a healthy eating index (HEI) in the analyses. However, weight status was assessed only with BMI, and no measure of developmental status was included in the protocol.
To advance our knowledge of the factors that predispose children to excessive weight gain and to inform future initiatives aimed at reducing the prevalence of childhood obesity, research is needed that overcomes the limitations of previous studies. To our knowledge, no previous study has included measures of overall diet quality and objectively measured physical activity and sedentary behavior in examining change in adiposity in youth. Furthermore, there is a need for research using prospective, longitudinal study designs in sizable and diverse samples of children. Accordingly, the purpose of this study was to observe the longitudinal associations between diet quality, objectively measured physical activity, and sedentary behavior and two measures of adiposity and a measure of weight status in a diverse sample of youth during the transition from childhood to adolescence.
Methods
Participants and Setting
Data were drawn from the Transitions and Activity Changes in Kids (TRACK) study, a multilevel longitudinal study of factors that may influence changes in children's physical activity as they transition from elementary school to middle school. A total of 1083 children (n = 501 boys, n = 576 girls) were enrolled in TRACK at baseline (fifth grade). The self-reported racial/ethnic breakdown of the sample was 36.4% white, 35.1% black, 11.2% Hispanic, and 17.3% other race/ethnicity (including multiracial). Mean age and BMI were 10.6 ± 0.6 years and 21.2 ± 4.9 kg/m2, respectively.
In the present analyses, children were excluded if they did not have data at both baseline (fifth grade) and follow-up (sixth or seventh grade) (n = 725), parent-reported education (n = 658), or maturity offset (n = 658), resulting in a final analytic sample of n = 658. There were no differences in percent male, parent education, or average BMI at baseline between those who were included in the analytic sample and those who were not. However, the analytic sample had fewer Hispanic and more white children and was slightly younger.
Children were recruited from 21 elementary schools in 2 school districts in South Carolina in 2010. All enrolled fifth grade students were invited during school assemblies to participate in the study. Sixty-four percent of children were recruited from one district and 57% from the other. Participants were followed into middle school and measured again in sixth and/or seventh grades (2011 and 2012). Before beginning any study procedures, parents provided informed consent and children provided assent. The Institutional Review Board at the University of South Carolina approved all research protocols.
Data collection procedures occurred over two sessions at the school with each child and were administered by a trained measurement team. During Session 1, participants completed a survey on a laptop computer, had anthropometric measures taken, and received an accelerometer. Participants completed the measures in small groups (≤24 students) at a place and time determined by the school administration. During Session 2, participants returned their accelerometer and received a modest compensation.
Measures
Physical activity
Physical activity was measured through accelerometry (ActiGraph GT1M and GT3X models, Pensacola, FL). Each child wore an accelerometer on his/her right hip for seven consecutive days during waking hours, except while bathing, swimming, or sleeping. Data were collected and stored in 60-second epochs. Any period of 60 or more minutes of consecutive zeros was considered nonwear time and recoded to missing. Moderate-to-vigorous physical activity (MVPA) was calculated using an age-specific prediction equation23 generalized to the mean age of the TRACK cohort. The threshold for MVPA was 2200 counts per minute, corresponding to 4.0 metabolic equivalents (METs; 1 MET = 3.5 mL O2 kg−1 min−1). Data for Sundays were excluded from the analysis due to the shorter amount of average wear time on that day.
In fifth grade, 80% of children provided ≥8 hours of accelerometry data on 4 or more days. On average, 73% of total possible records from Monday to Saturday were available over the 3 years. Missing data were imputed by gender for participants with at least 2 days of ≥8 hours of wear time. Multiple imputation regressions in Proc MI in SAS (Version 9.3; SAS Institute, Inc., Cary, NC) using all 7 days of physical activity variables (sedentary, light, moderate-to-vigorous, and vigorous) were conducted. A total of five data sets were imputed and then averaged for each variable. MVPA time per day was divided by minutes of wear time to produce minutes per hour of MVPA.
Sedentary behavior
Sedentary behaviors are those that do not increase the rate of energy expenditure substantially above the resting level, and they include sitting, lying down, watching television, and other forms of screen-based entertainment.24 Sedentary behavior is best conceptualized as behavior that is distinct from all levels of physical activity, including light and moderate intensities.25 In the present study, time spent in sedentary behavior was measured through accelerometry, and the procedures for collection and reduction of the accelerometry data are described above. The accelerometry cut point for sedentary behavior was counts <100/min. As was the case for MVPA, the data for sedentary behavior were expressed as minutes per hour of observation.
Diet quality
Diet intake was assessed by the Block Food Screener for Kids, which has been validated with 24-hour recalls in 10–17-year-olds.26 The screener asks whether 41 specific food items were consumed in the last week. If a child responds yes to a food item, he/she is asked on how many days the item was consumed and the usual amount eaten. For the present study, a measure of diet quality using information from the food screener was created based on a protocol from the HEI-2010.27 Briefly, specific components were chosen to reflect healthy dietary patterns, including total vegetables, total fruit, whole grains, dairy, and total protein. The overall score was calculated on a per calorie basis and adjusted for energy intake. Values greater than 5000 kcal/day were considered implausible, and these children were excluded from the analysis.28 Higher scores indicated better diet quality, with a maximum score of 50 points.
Anthropometry
Height and weight were measured by trained staff after the child removed heavy clothing and shoes. Children's standing and seated heights were measured to the nearest 0.1 cm using a portable stadiometer (Seca, Hamburg, Germany). Weight was measured to the nearest 0.1 kg using an electronic scale (Model 770; Seca). The average of two measurements was used for both height and weight, and BMI was calculated using the standard equation (kg/m2). Total body bioelectrical impedance (RJL Quantum II BIA Systems, Clinton Township, MI) was measured according to the manufacturer's standard protocol on the right side (hand to foot). Fat-free mass (FFM) was calculated using the following equation: FFM = [3.474 + (0.459 × Height2/Resistance) + (0.064 × Weight)]/[0.769 − (0.009 × Age) −0.016 × Sex], where 1 = males and 0 = females.29 Fat mass was determined by subtracting FFM from body weight, and fat mass index (FMI) was calculated by dividing fat mass by height (m2). Percent body fat (PBF) was also calculated using the following equation: PBF = (Weight − FFM)/Weight × 100.
Maturity offset
Maturity offset was calculated using gender-specific equations.30,31 This noninvasive method predicts peak height velocity using anthropometric variables. A negative maturity offset represents the number of years the child is from reaching peak height velocity, while a positive maturity offset represents the number of years a child is beyond peak height velocity. Maturity offset at fifth grade was included as a covariate in the analyses.
Statistical Analysis
Descriptive statistics were calculated by gender. Chi-square analyses and t-tests were used to determine any significant differences between boys and girls in the demographic variables. Growth curve analyses32 using PROC MIXED (SAS Institute, Inc.) were used to study longitudinal change in FMI, PBF, and BMI. These models showed change over time by fitting the slope at the individual level (Level 1). A second level of analyses (Level 2) related predictors to interindividual differences in change.
Unconditional growth models (only time in the model) were calculated to provide baseline models of change in measures of adiposity and weight status (Model 1). A second set of models was calculated that also included the time-varying variables, MVPA, sedentary behavior, and diet quality, along with demographic variables, (race/ethnicity, parent education), time, and interaction terms for the time-varying variables by time (Model 2). A third set of models added fifth grade maturity offset with the other variables from Model 2 (Model 3). Nonsignificant interactions were deleted and models were rerun.
For ease of interpretation, the continuous variables were centered by subtracting sex-specific grand means of the variable, and time was coded as 0, 1, and 2. Child and child within school were modeled as random effects to accommodate the expected correlation among observations taken on children from the same school.33 In addition, the intercept and slope (i.e., time) were modeled as random effects. An unstructured covariance matrix was used for all models. Goodness of fit for each model was estimated using three statistics: deviance, Akaike's information criteria, and Bayesian information criteria.32 Lower values of each of these statistics indicate better fit.
To further examine the impact of low and high participation in MVPA on FMI, PBF, and BMI, sex-specific tertiles of minute per hour of fifth grade MVPA were created.34 Mixed model least-square means were calculated for FMI, PBF, and BMI at each grade for the lowest and highest tertiles of fifth grade MVPA after adjusting for race/ethnicity, parent education, and maturity offset (Model 3).
Results
The analysis sample included 658 children (45.1% boys), who provided data at both baseline (fifth grade) and follow-up at sixth and/or seventh grades; 60% had data at all three time points. Of this sample, 40.3% of the children were white, 32.8% black, 9.1% Hispanic, and 17.8% mixed or other race/ethnicity. Over 35% of parents had completed college or earned an advanced degree. Fifth grade girls, compared with boys, were taller and heavier and were closer to predicted peak height velocity (Table 1).
Table 1.
Baseline Characteristics of 658 Children Participating in the Transitions and Activity Changes in Kids Study (Fifth Grade)
| Characteristic | Boys (n = 297) | Girls (n = 361) | pa |
|---|---|---|---|
| Gender (%) | 45.1 | 54.9 | |
| Race (%) | |||
| White | 37.7 | 42.4 | 0.14 |
| Black | 37.0 | 29.4 | |
| Hispanic | 7.4 | 10.5 | |
| Other | 17.9 | 17.7 | |
| Parent education, college graduate, or higher (%) | 36.0 | 37.7 | 0.66 |
| Age, years, mean (SD) | 11.1 (0.4) | 11.0 (0.5) | 0.47 |
| Maturity offset, mean (SD) | −2.6 (0.6) | −0.8 (0.7) | <0.001 |
| Height, cm, mean (SD) | 145.6 (6.5) | 148.0 (8.1) | <0.001 |
| Weight, kg, mean (SD) | 44.5 (12.6) | 47.2 (13.0) | 0.01 |
p-Value for difference between boys and girls.
SD, standard deviation.
Mean (standard deviation) MVPA, sedentary time, diet quality, and adiposity measures as observed in children in fifth, sixth, and seventh grades are shown separately for boys and girls in Table 2. Height, weight, fat mass, and BMI increased over time in boys, while FMI and PBF declined. In girls, height, weight PBF, fat mass, FMI, and BMI increased over time. Minutes per hour of MVPA declined in both boys and girls, while minutes per hour of sedentary behavior increased. There was no change in diet quality over time for either boys or girls.
Table 2.
Longitudinal Mean (Standard Deviation) Adiposity, Physical Activity, Sedentary Behavior, and Diet Quality
| Boys | |||
|---|---|---|---|
| Fifth grade (n = 297) | Sixth grade (n = 252) | Seventh grade (n = 227) | |
| Height, cm | 145.6 (6.5) | 150.8 (7.5) | 158.2 (8.4) |
| Weight, kg | 44.5 (12.6) | 49.3 (13.9) | 55.3 (15.9) |
| BMI, kg/m2 | 20.7 (4.8) | 21.4 (4.8) | 21.8 (5.1) |
| PBF (%) | 23.3 (9.5) | 21.8 (9.5) | 20.9 (9.8) |
| Fat mass, kg | 11.4 (8.3) | 11.6 (9.1) | 12.1 (10.2) |
| FMI, kg/m2 | 5.2 (3.5) | 5.0 (3.7) | 4.7 (3.8) |
| MVPA, min/h | 3.7 (2.1) | 3.4 (1.8) | 3.3 (2.0) |
| Sedentary, min/h | 31.0 (4.2) | 34.1 (4.1) | 35.9 (4.1) |
| Diet quality | 29.8 (5.5) | 28.5 (6.0) | 29.0 (5.5) |
| Girls | |||
|---|---|---|---|
| Fifth grade (n = 361) | Sixth grade (n = 299) | Seventh grade (n = 283) | |
| Height, cm | 148.0 (8.1) | 153.2 (7.6) | 157.6 (7.0) |
| Weight, kg | 47.2 (13.0) | 52.2 (14.3) | 57.5 (15.4) |
| BMI, kg/m2 | 21.3 (4.8) | 22.1 (5.2) | 23.0 (5.6) |
| PBF (%) | 27.4 (8.0) | 27.8 (9.7) | 29.1 (9.4) |
| Fat mass, kg | 14.6 (8.8) | 15.8 (9.7) | 18.1 (10.7) |
| FMI, kg/m2 | 6.6 (3.7) | 6.6 (3.9) | 7.2 (4.1) |
| MVPA, min/h | 2.2 (1.2) | 1.9 (1.0) | 1.8 (1.1) |
| Sedentary, min/h | 32.8 (4.4) | 37.0 (4.5) | 38.8 (4.4) |
| Diet quality | 30.3 (5.4) | 29.5 (5.6) | 29.2 (6.0) |
FMI, fat mass index; MVPA, moderate-to-vigorous physical activity; PBF, percent body fat.
Unconditional growth models (Model 1) for FMI (Table 3), PBF (Table 4), and BMI (Table 5) are presented separately by gender. Among fifth grade boys, FMI was 5.2 kg/m2 and declined by 0.2 kg/m2 per year, PBF was 23.2% and declined by 1.2% per year, while BMI was 20.8 kg/m2 and increased by 0.6 kg/m2 per year. Among fifth grade girls, FMI was 6.5 kg/m2 and increased 0.3 kg/m2 per year, PBF was 27.2% and increased 0.9% per year, and BMI was 21.3 kg/m2 and increased by 0.8 kg/m2 per year.
Table 3.
Growth Curve Models of Fat Mass Index (kg/m2) for Boys and Girls
| Boys | Girls | |||||
|---|---|---|---|---|---|---|
| Predictors | Model 1 unconditional estimate (SE) | Model 2 estimate (SE) | Model 3 estimate (SE) | Model 1 unconditional estimate (SE) | Model 2 estimate (SE) | Model 3 estimate (SE) |
| Fixed effects | ||||||
| Intercept | 5.24 (0.21)*** | 5.33 (0.42)*** | 5.07 (0.35)*** | 6.49 (0.21)*** | 5.45 (0.36)*** | 5.63 (0.36)*** |
| Time | −0.22 (0.09)* | −0.28 (0.11)* | −0.26 (0.11)* | 0.29 (0.08)** | 0.31 (0.10)* | 0.33 (0.10)* |
| MVPA | −0.09 (0.03)* | −0.10 (0.03)** | −0.16 (0.05)** | −0.16 (0.05)** | ||
| Sedentary | 0.05 (0.02)* | 0.04 (0.02)* | −0.02 (0.01) | −0.04 (0.02)* | ||
| Sedentary × time | −0.03 (0.01)* | −0.03 (0.01)* | a | 0.02 (0.01)* | ||
| Diet quality | 0.03 (0.01)* | 0.03 (0.01)* | −0.01 (0.01) | −0.01 (0.01) | ||
| Diet quality × time | −0.03 (0.01)* | −0.03 (0.01)* | a | a | ||
| Race | ||||||
| Black | −0.08 (0.46) | 0.48 (0.38) | 1.75 (0.45)*** | 0.98 (0.40)* | ||
| Hispanic | 1.37 (0.80) | 1.55 (0.65)* | −0.61 (0.65) | 0.10 (0.57) | ||
| Other | −0.12 (0.57) | 0.09 (0.47) | 0.49 (0.53) | 0.30 (0.46) | ||
| White | Reference | Reference | Reference | Reference | ||
| Parent<college graduate | −0.08 (0.42) | −0.11 (0.34) | 0.81 (0.39)* | 0.64 (0.34) | ||
| Maturity offset | 3.49 (0.28)*** | 2.75 (0.25)*** | ||||
| Variance components (random effects) | ||||||
| Level 1 within child | 0.84 (0.08)*** | 0.82 (0.08)*** | 0.82 (0.08)*** | 0.52 (0.05)*** | 0.52 (0.05)*** | 0.51 (0.05)*** |
| Level 2 (Intercept) | 11.96 (1.05)*** | 11.08 (0.98)*** | 7.00 (0.64)*** | 13.15 (1.02)*** | 12.11 (0.94)*** | 8.89 (0.70)*** |
| Level 2 (Slope) | 0.45 (0.09)*** | 0.43 (0.09)*** | 0.43 (0.09)*** | 0.45 (0.07)*** | 0.44 (0.07)*** | 0.45 (0.07)*** |
| Goodness of fit | ||||||
| Deviance | 3338.3 | 3305.0 | 3180.1 | 3896.8 | 3860.0 | 3752.1 |
| AIC | 3352.3 | 3337.8 | 3214.1 | 3912.8 | 3888.0 | 3786.1 |
| BIC | 3356.2 | 3346.1 | 3223.7 | 3916.0 | 3893.5 | 3792.9 |
Predictors were centered and values reported are coefficients with standard errors in parentheses estimated using full maximum likelihood.
p < 0.05; **p < 0.01; ***p < 0.001.
Nonsignificant interaction removed from model.
AIC, Akaike's information criterion; BIC, Bayesian information criterion.
Table 4.
Growth Curve Models of Percent Body Fat for Boys and Girls
| Boys | Girls | |||||
|---|---|---|---|---|---|---|
| Predictors | Model 1 unconditional estimate (SE) | Model 2 estimate (SE) | Model 3 estimate (SE) | Model 1 unconditional estimate (SE) | Model 2 estimate (SE) | Model 3 estimate (SE) |
| Fixed effects | ||||||
| Intercept | 23.23 (0.55)*** | 22.97 (1.10)*** | 22.36 (0.93)*** | 27.15 (0.53)*** | 25.69 (0.87)*** | 26.05 (0.83)*** |
| Time | −1.16 (0.31)** | −1.37 (0.33)** | −1.30 (0.35)** | 0.87 (0.32)* | 0.80 (0.36) | 0.90 (0.36)* |
| MVPA | −0.29 (0.11)* | −0.33 (0.11)** | −0.60 (0.18)** | −0.60 (0.18)** | ||
| Sedentary | 0.09 (0.06) | 0.06 (0.05) | −0.03 (0.05) | −0.06 (0.05) | ||
| Sedentary × time | a | a | a | a | ||
| Diet quality | 0.12 (0.05)* | 0.11 (0.05)* | −0.03 (0.03) | −0.03 (0.03) | ||
| Diet quality × time | −0.11 (0.04)** | −0.11 (0.04)** | a | a | ||
| Race | ||||||
| Black | −0.45 (1.18) | 0.82 (1.01) | 2.64 (1.01)* | 1.10 (0.91) | ||
| Hispanic | 4.83 (2.05)* | 5.29 (1.73)** | −2.24 (1.44) | −0.74 (1.27) | ||
| Other | 0.04 (1.47) | 0.52 (1.24) | 0.29 (1.17) | −0.16 (1.03) | ||
| White | Reference | Reference | Reference | Reference | ||
| Parent<college graduate | 0.39 (1.06) | 0.36 (0.90) | 1.48 (0.87) | 1.28 (0.76) | ||
| Maturity offset | 8.29 (0.75)*** | 5.79 (0.56)*** | ||||
| Variance components (random effects) | ||||||
| Level 1 within child | 10.32 (1.00)*** | 10.12 (0.98)*** | 10.13 (0.99)*** | 8.81 (0.80)*** | 8.65 (0.78)*** | 8.64 (0.78)*** |
| Level 2 intercept | 81.09 (7.45)*** | 74.25 (6.94)*** | 48.88 (4.85)*** | 58.13 (5.01)*** | 53.54 (4.70)*** | 40.41 (3.70)*** |
| Level 2 slope | 3.53 (0.97)*** | 3.37 (0.94)*** | 3.30 (0.94)*** | 3.80 (0.83)*** | 3.90 (0.83)*** | 3.88 (0.83)*** |
| Goodness of fit | ||||||
| Deviance | 5051.4 | 5019.2 | 4918.0 | 6000.0 | 5969.5 | 5876.5 |
| AIC | 5065.4 | 5049.2 | 4950.0 | 6016.0 | 5999.5 | 5908.5 |
| BIC | 5069.4 | 5057.6 | 4959.1 | 6019.2 | 6005.5 | 5914.9 |
Predictors were centered and values reported are coefficients with standard errors in parentheses estimated using full maximum likelihood.
p < 0.05; **p < 0.01; ***p < 0.001.
Nonsignificant interaction removed from model.
Table 5.
Growth Curve Models Body–Mass Index (kg/m2) for Boys and Girls
| Boys | Girls | |||||
|---|---|---|---|---|---|---|
| Predictors | Model 1 unconditional estimate (SE) | Model 2 estimate (SE) | Model 3 estimate (SE) | Model 1 unconditional estimate (SE) | Model 2 estimate (SE) | Model 3 estimate (SE) |
| Fixed effects | ||||||
| Intercept | 20.79 (0.27)*** | 20.79 (0.57)*** | 20.49 (0.46)*** | 21.29 (0.30)*** | 19.93 (0.48)*** | 20.34 (0.48)*** |
| Time | 0.60 (0.06)*** | 0.57 (0.08)*** | 0.58 (0.07)*** | 0.83 (0.06)*** | 0.82 (0.08)*** | 0.84 (0.08)*** |
| MVPA | −0.08 (0.03)* | −0.09 (0.03)** | −0.16 (0.05)** | −0.16 (0.05)** | ||
| Sedentary | 0.04 (0.02) | 0.02 (0.02) | −0.01 (0.02) | −0.02 (0.02) | ||
| Sedentary × time | −0.03 (0.01)* | −0.03 (0.01)* | a | a | ||
| Diet quality | 0.01 (0.01) | −0.01 (0.01) | 0.001 (0.01) | −0.001 (0.01) | ||
| Diet quality × time | −0.02 (0.01)* | a | a | a | ||
| Race | ||||||
| Black | 0.29 (0.62) | 0.98 (0.47)* | 2.31 (0.59)*** | 1.19 (0.51)* | ||
| Hispanic | 1.39 (1.07) | 1.72 (0.80)* | −0.66 (0.85) | −0.21 (0.72) | ||
| Other | −0.15 (0.77) | 0.19 (0.58) | 0.65 (.69) | 0.30 (0.58) | ||
| White | Reference | Reference | Reference | Reference | ||
| Parent<college graduate | −0.17 (0.56) | −0.26 (0.42) | 1.07 (0.51)* | 0.77 (0.43) | ||
| Maturity offset | 5.42 (0.35)*** | 3.78 (0.06)*** | ||||
| Variance components (random effects) | ||||||
| Level 1 within | 0.75 (0.07)*** | 0.71 (0.07)*** | 0.71 (0.07)*** | 0.65 (0.06)*** | 0.65 (0.06)*** | 0.65 (0.06)*** |
| Level 2 Intercept | 21.30 (1.80)*** | 20.49 (1.74)*** | 10.92 (0.96)*** | 22.74 (1.75)*** | 20.94 (1.62)*** | 14.52 (1.14)*** |
| Level 2 slope | 0.53 (0.09)*** | 0.53 (0.09)*** | 0.56 (0.09)*** | 0.71 (0.09)*** | 0.70 (0.09)*** | 0.70 (0.09)*** |
| Goodness of fit | ||||||
| Deviance | 3480.2 | 3457.9 | 3287.0 | 4265.5 | 4229.8 | 4111.3 |
| AIC | 3492.2 | 3489.9 | 3321.0 | 4279.5 | 4259.8 | 4143.3 |
| BIC | 3495.6 | 3499.0 | 3330.6 | 4282.7 | 4265.7 | 4149.7 |
Predictors were centered and values reported are coefficients with standard errors in parentheses estimated using full maximum likelihood.
p < 0.05; **p < 0.01; ***p < 0.001.
Nonsignificant interactions removed from model.
For both boys and girls, conditional growth models (Model 2 and Model 3; Tables 3–5) indicated that for time-varying MVPA, there were significant negative associations with initial FMI, PBF, and BMI values that were maintained from fifth to seventh grade. These associations were independent of time-varying diet quality and sedentary behavior and maturity offset. Among boys, counterintuitively, initial higher diet quality was positively associated with both FMI and PBF. However, among girls, diet quality was unrelated to the adiposity variables. Among boys, sedentary behavior was positively associated with FMI in fifth grade, but a significant inverse association was demonstrated in fifth grade girls. Sedentary behavior was not related to PBF in either boys or girls.
Least-square means for FMI (Panel A), PBF (Panel B), and BMI (Panel C) comparing the lowest and highest tertiles of fifth grade MVPA are presented in Figure 1. For both boys and girls, least-square means of FMI, PBF, and BMI were significantly lower for the highest MVPA tertile compared with the lowest MVPA tertile at fifth, sixth, and seventh grades (p < 0.05).
Figure 1.
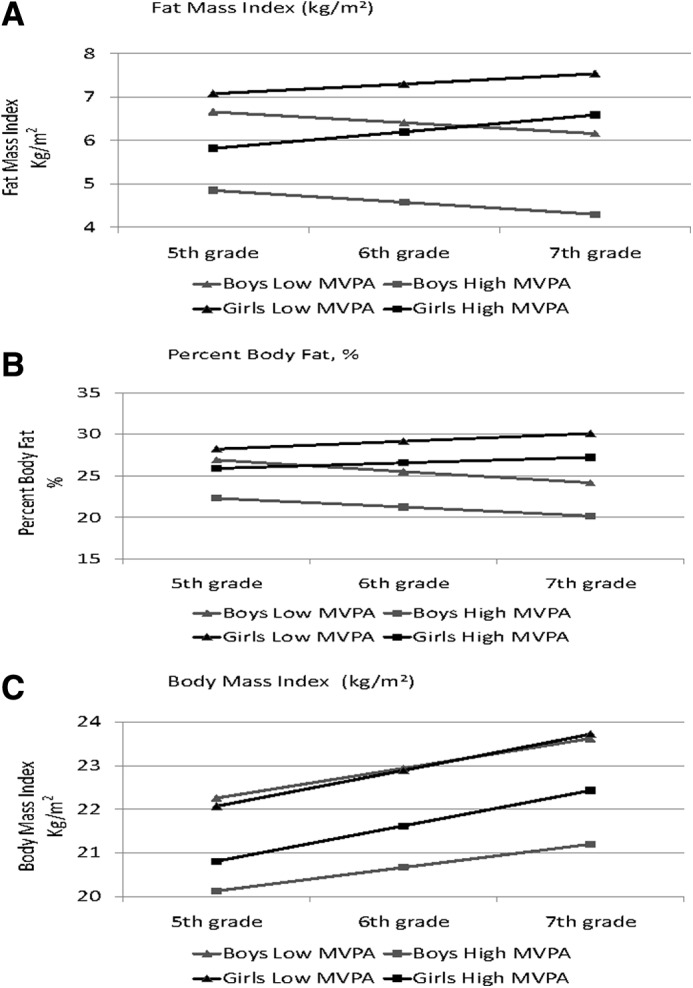
Least-square means for boys and girls in the lowest (n = 100 boys, <2.52 min/h; n = 120 girls, <1.56 min/h) and highest (n = 98 boys, ≥4.18 min/h; n = 121 girls, ≥2.44 min/h) tertiles of fifth grade MVPA. (A) At each grade, FMI in the high MVPA tertile was lower than in the low MVPA tertile (p < 0.05). (B) At each grade, PBF in the high MVPA tertile was lower than in the low MVPA tertile (p < 0.05). (C) At each grade, BMI in the high MVPA tertile was lower than in the low MVPA tertile (p < 0.05). FMI, fat mass index; PBF, percent body fat; MVPA, moderate-to-vigorous physical activity.
Discussion
The major finding of this study was that as boys and girls transitioned from elementary to middle school, children who participated in higher levels of MVPA maintained more favorable levels of adiposity. The study found significant inverse relationships between MVPA and FMI and PBF in both boys and girls that spanned the period from fifth to seventh grade. Comparable observations were made for BMI. These relationships were independent of sedentary behavior, diet quality, and maturity offset. Rates of change in adiposity and weight status were not significantly associated with MVPA, but parallel trajectories across the 3 years for each measure of adiposity (i.e., FMI and PBF) and MVPA indicated that children with higher levels of MVPA had lower levels of adiposity at each grade. Our findings indicate that the beneficial effect of MVPA on development of adiposity is manifested in children of elementary school age and continues as they progress into middle school.
The findings of the present study add to a growing scientific literature on the associations between physical activity and adiposity in children. Several studies, using prospective observational designs, have observed that higher levels of physical activity are longitudinally associated with adiposity and/or weight status in youth.35–37 Riddoch et al., working with the ALSPAC birth cohort in the United Kingdom, followed 12-year-old children for 2 years and found that higher levels of objectively measured MVPA at baseline were associated with lower levels of fat mass at follow-up.37 Neither diet nor sedentary behavior was considered in that study. Similar findings were reported by Fisher et al.,35 who observed that 8-year-old children with higher objectively measured MVPA at baseline showed smaller increases in FMI after 1 year. Adjustment was made for sedentary behavior, but no measure of diet was included. Likewise, Kwon et al. found that objectively measured MVPA was inversely associated with change in fat mass when children were followed from age 8 to age 15.36 Adjustment for sedentary behavior was included, but again diet was not incorporated into the models.
The findings of the present study are consistent with the findings of those three studies, in that objectively measured MVPA was inversely associated with adiposity. However, this study makes a unique contribution to this body of knowledge by focusing on objectively measured MVPA while controlling for the potential effects of sedentary behavior and diet quality. Furthermore, the study is unique in investigating these relationships in a diverse and relatively large cohort of US children. In addition, our finding that MVPA was longitudinally associated with adiposity and weight status is consistent with the results of research on the role of physical activity in regulating body weight and composition.38 That research has demonstrated that physical activity, particularly higher levels of activity at vigorous intensity, is associated with a tight coupling between energy intake and energy expenditure.38,39 These findings point to a critical role for MVPA in prevention of excessive weight gain during the transition from childhood to adolescence.
BMI is a measure of weight status that is widely used in both epidemiological research and clinical practice, and BMI-based standards for overweight and obesity have been adopted and disseminated by the US Centers for Disease Control and Prevention and the World Health Organization.40,41 BMI is an attractive metric, in part, because it is calculated from unobtrusive and low-burden measures of height and weight. Furthermore, in cross-sectional analyses, BMI is known to be highly correlated with measures of adiposity, including PBF and FMI.20,42 For these reasons, BMI has come into wide application in public health and medicine.21 However, BMI can be a poor measure of adiposity in some persons, particularly those whose lean body weight is divergent from age–gender norms.43 In addition, there is a concern that change in BMI may not be a valid reflection of change in adiposity during critical developmental periods such as puberty.21,44 In this context, it is important to note that in the present study, BMI performed in growth curve analyses in a manner that was very similar to the behavior of PBF and FMI. MVPA was found to be consistently inversely related to all three measures. This finding supports utilization of BMI in longitudinal studies aimed at identifying behavioral factors that influence development of adiposity.
Over the past decade, health and medical researchers have shown increasing interest in the health effects of sedentary behavior,24,45 and some have hypothesized that excessive time spent in sedentary behavior may have contributed to the secular increase in the prevalence of overweight and obesity.46 However, the research on sedentary behavior and its impact on health has not yet produced a clear consensus. As the findings of a recent National Institutes of Health workshop emphasized, much remains to be learned about the amounts and patterns of sedentary behavior that may increase the risk of negative health outcomes in children.25 In particular, there is uncertainty regarding an effect of sedentary behavior on health independent of physical activity.17,47
The results of the present study reflect the inconsistent findings reported in the existing literature. We found some significant associations between sedentary behavior and measures of adiposity, but there was no clear consistent pattern in those associations. If sedentary behavior does indeed impact health outcomes in youth, it is possible that longer periods of observation and more sophisticated expressions of sedentary behavior will be needed to detect them.
As with sedentary behavior, our observations regarding the relationship of diet quality to measures of adiposity were also inconsistent. While there is broad consensus in the public health and medical communities that dietary behavior exerts an important influence on weight status in children, the related scientific literature is far from compelling on this issue. Recent reviews of prospective observational studies have concluded that measures of dietary behavior have not been strong consistent predictors of change in weight and adiposity.47,48 In the present study, we found inverse associations between diet quality and change in adiposity in boys, but not girls. To elucidate the impact of diet on the development of adiposity during childhood, future epidemiological research should employ longer follow-up periods, the best available measures of dietary behavior, and state-of-the-art measures of adiposity. Furthermore, as was done in the present study, future research on diet and adiposity should include adjustment for objectively measured physical activity and sedentary behavior.
The major strengths of this study include a sizable and racially/ethnically diverse sample of children that was followed during an important developmental period, the transition from elementary school to middle school. Additional strengths include measuring MVPA and sedentary behavior by accelerometry, including two adiposity variables, and adjusting observed relationships for the children's maturity status. Dietary behavior was measured with an index of diet quality, and we consider this to be both a strength and a limitation. It is a strength that the diet quality index was derived from data collected using the Block Food Screener for Kids, an instrument with established measurement properties.26 Furthermore, the diet quality index used in this study is similar to indices used in previous studies that have observed significant associations with weight status in children.49,50 However, it should be noted that this procedure is limited by the recall bias that is typically associated with self-report of diet.51 The analyses were not adjusted for potential influences of seasonality or day-to-day weather conditions. Other limitations include a sample of children drawn from only two communities in one state and a follow-up period of only 2 years.
Conclusions
In summary, this study found that boys and girls who participated in higher levels of MVPA maintained more favorable levels for two measures of adiposity and a measure of weight status. The children were observed across a 2-year period that spanned their transition from elementary school to middle school. Sedentary behavior and diet quality were inconsistently related to the adiposity variables. The findings of this study contribute to a growing body of research that supports the important role of physical activity in maintaining normal weight status and preventing overweight and obesity. These results emphasize the importance of interventions targeting the age-related decline in physical activity that often accompanies the transition from childhood to adolescence.
Acknowledgments
The authors would like to thank the children and parents who participated in this study and Gaye Groover Christmus, MPH, who provided editorial assistance in the preparation of the manuscript. This study was funded by the National Heart, Lung, and Blood Institute (R01HL091002-01A1; PI: R.R.P.).
Author Disclosure Statement
No competing financial interests exist.
References
- 1.Troiano RP, Flegal KM, Kuczmarski RJ, et al. . Overweight prevalence and trends for children and adolescents. The National Health and Nutrition Examination Surveys, 1963 to 1991. Arch Pediatr Adolesc Med 1995;149:1085–1091 [DOI] [PubMed] [Google Scholar]
- 2.Ogden CL, Carroll MD, Fryay CD, Flegal KM. Prevalence of Obesity Among Adults and Youth: United States, 2011–2014. NCHS Data Brief, No 219. National Center for Health Statistics: Hyattsville, MD, 2015 [PubMed] [Google Scholar]
- 3.Institute of Medicine. Preventing Childhood Obesity: Health in the Balance. The National Academies Press: Washington, DC, 2005 [PubMed] [Google Scholar]
- 4.Daniels SR. The consequences of childhood overweight and obesity. Future Child 2006;16:47–67 [DOI] [PubMed] [Google Scholar]
- 5.Reilly JJ. Obesity in childhood and adolescence: Evidence based clinical and public health perspective. Postgrad Med J 2006;82:429–437 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Institute of Medicine. Early Childhood Obesity Prevention Policies. The National Academies Press: Washington, DC, 2011 [Google Scholar]
- 7.Centers for Disease Control and Prevention. Strategies to Prevent Obesity and Other Chronic Diseases: The CDC Guide to Strategies to Increase Physical Activity in the Community. US DHHS: Atlanta, 2011 [Google Scholar]
- 8.Centers for Disease Control and Prevention. Strategies to Prevent Obesity and Other Chronic Diseases: The CDC Guide to Strategies to Increase the Consumption of Fruits and Vegetables. US DHHS: Atlanta, 2011 [Google Scholar]
- 9.Institute of Medicine. Accelerating Progress in Obesity Prevention: Solving the Weight of the Nation. The National Academies Press: Washington, DC, 2012 [PubMed] [Google Scholar]
- 10.World Health Organization. Interventions on Diet and Physical Activity: What Works. Summary Report. WHO: Geneva, 2008 [PubMed] [Google Scholar]
- 11.Chen A. On childhood obesity prevention: “Exercise is medicine” vs “Exercise is vaccine”. J Sport Sci 2012;1:172–173 [Google Scholar]
- 12.Centers for Disease Control and Prevention. The Power of Prevention: Chronic Disease…The Public Health Challenge of the 21st Century. US DHHS: Atlanta, 2009 [Google Scholar]
- 13.Waters E, de Silva-Sanigorski A, Hall BJ, et al. . Interventions for preventing obesity in children. Cochrane Database Syst Rev 2011:CD001871. [DOI] [PubMed] [Google Scholar]
- 14.Eisenmann JC. Insight into the causes of the recent secular trend in pediatric obesity: Common sense does not always prevail for complex, multi-factorial phenotypes. Prev Med 2006;42:329–335 [DOI] [PubMed] [Google Scholar]
- 15.Visscher TL, Kremers SP. How can we better prevent obesity in children? Curr Obes Rep 2015;4:371–378 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Must A, Tybor DJ. Physical activity and sedentary behavior: A review of longitudinal studies of weight and adiposity in youth. Int J Obes (Lond) 2005;29(Suppl 2):S84–S96 [DOI] [PubMed] [Google Scholar]
- 17.Pate RR, O'Neill JR, Liese AD, et al. . Factors associated with development of excessive fatness in children and adolescents: A review of prospective studies. Obes Rev 2013;14:645–658 [DOI] [PubMed] [Google Scholar]
- 18.Ramires VV, Dumith SC, Goncalves H. Longitudinal association between physical activity and body fat during adolescence: A systematic review. J Phys Act Health 2015;12:1344–1358 [DOI] [PubMed] [Google Scholar]
- 19.Fulton JE, Dai S, Steffen LM, et al. . Physical activity, energy intake, sedentary behavior, and adiposity in youth. Am J Prev Med 2009;37(1 Suppl):S40–S49 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Freedman DS, Wang J, Maynard LM, et al. . Relation of BMI to fat and fat-free mass among children and adolescents. Int J Obes (Lond) 2005;29:1–8 [DOI] [PubMed] [Google Scholar]
- 21.Going S, Lee V, Blew R, et al. . Top 10 research questions related to body composition. Res Q Exerc Sport 2014;85:38–48 [DOI] [PubMed] [Google Scholar]
- 22.Mitchell JA, Pate RR, Beets MW, Nader PR. Time spent in sedentary behavior and changes in childhood BMI: A longitudinal study from ages 9 to 15 years. Int J Obes (Lond) 2013;37:54–60 [DOI] [PubMed] [Google Scholar]
- 23.Freedson P, Pober D, Janz KF. Calibration of accelerometer output for children. Med Sci Sports Exerc 2005;37(11 Suppl):S523–S530 [DOI] [PubMed] [Google Scholar]
- 24.Pate RR, O'Neill JR, Lobelo F. The evolving definition of “sedentary”. Exerc Sport Sci Rev 2008;36:173–178 [DOI] [PubMed] [Google Scholar]
- 25.Boyington J, Joseph L, Fielding R, Pate R. Sedentary behavior research priorities—NHLBI/NIA Sedentary Behavior Workshop summary. Med Sci Sports Exerc 2015;47:1291–1294 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hunsberger M, O'Malley J, Block T, Norris JC. Relative validation of Block Kids Food Screener for dietary assessment in children and adolescents. Matern Child Nutr 2015;11:260–270 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Guenther PM, Casavale KO, Reedy J, et al. . Update of the Healthy Eating Index: HEI-2010. J Acad Nutr Diet 2013;113:569–580 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Willett W. Nutritional Epidemiology, 2nd ed. Oxford University Press: New York, 1998 [Google Scholar]
- 29.Horlick M, Arpadi SM, Bethel J, et al. . Bioelectrical impedance analysis models for prediction of total body water and fat-free mass in healthy and HIV-infected children and adolescents. Am J Clin Nutr 2002;76:991–999 [DOI] [PubMed] [Google Scholar]
- 30.Mirwald RL, Baxter-Jones AD, Bailey DA, Beunen GP. An assessment of maturity from anthropometric measurements. Med Sci Sports Exerc 2002;34:689–694 [DOI] [PubMed] [Google Scholar]
- 31.Malina RM, Koziel SM. Validation of maturity offset in a longitudinal sample of Polish boys. J Sports Sci 2014;32:424–437 [DOI] [PubMed] [Google Scholar]
- 32.Singer JD, Willett JB. Applied Longitudinal Data Analysis. Modeling Change and Event Occurrence. Oxford University Press: New York, 2003 [Google Scholar]
- 33.Murray DM. Design and Analysis of Group-Randomized Trials. Oxford University Press: New York, 1998 [Google Scholar]
- 34.Janz KF, Kwon S, Letuchy EM, et al. . Sustained effect of early physical activity on body fat mass in older children. Am J Prev Med 2009;37:35–40 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fisher A, Hill C, Webber L, et al. . MVPA is associated with lower weight gain in 8–10 year old children: A prospective study with 1 year follow-up. PLoS One 2011;6:e18576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kwon S, Burns TL, Levy SM, Janz KF. Which contributes more to childhood adiposity-high levels of sedentarism or low levels of moderate-through-vigorous physical activity? The Iowa Bone Development Study. J Pediatr 2013;162:1169–1174 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Riddoch CJ, Leary SD, Ness AR, et al. . Prospective associations between objective measures of physical activity and fat mass in 12–14 year old children: The Avon Longitudinal Study of Parents and Children (ALSPAC). BMJ 2009;339:b4544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Chaput JP, Klingenberg L, Rosenkilde M, et al. . Physical activity plays an important role in body weight regulation. J Obes 2011;2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Gutin B. Diet vs exercise for the prevention of pediatric obesity: The role of exercise. Int J Obes (Lond) 2011;35:29–32 [DOI] [PubMed] [Google Scholar]
- 40.Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, et al. . CDC Growth Charts: United States. Adv Data 2000:1–27 [PubMed] [Google Scholar]
- 41.WHO. Obesity: Preventing and Managing the Global Epidemic. WHO Technical Report Series No. 894. Geneva, 2000 [PubMed] [Google Scholar]
- 42.Flegal KM, Shepherd JA, Looker AC, et al. . Comparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adults. Am J Clin Nutr 2009;89:500–508 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Sopher AB, Thornton JC, Wang J, et al. . Measurement of percentage of body fat in 411 children and adolescents: A comparison of dual-energy X-ray absorptiometry with a four-compartment model. Pediatrics 2004;113:1285–1290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Horlick M. Body mass index in childhood—measuring a moving target. J Clin Endocrinol Metab 2001;86:4059–4060 [DOI] [PubMed] [Google Scholar]
- 45.Gibbs BB, Hergenroeder AL, Katzmarzyk PT, et al. . Definition, measurement, and health risks associated with sedentary behavior. Med Sci Sports Exerc 2015;47:1295–1300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Bassett DR, John D, Conger SA, et al. . Trends in physical activity and sedentary behaviors of United States youth. J Phys Act Health 2015;12:1102–1111 [DOI] [PubMed] [Google Scholar]
- 47.Basterfield L, Pearce MS, Adamson AJ, et al. . Physical activity, sedentary behavior, and adiposity in English children. Am J Prev Med 2012;42:445–451 [DOI] [PubMed] [Google Scholar]
- 48.Bleich SN, Ku R, Wang YC. Relative contribution of energy intake and energy expenditure to childhood obesity: A review of the literature and directions for future research. Int J Obes (Lond) 2011;35:1–15 [DOI] [PubMed] [Google Scholar]
- 49.Jennings A, Welch A, van Sluijs EM, et al. . Diet quality is independently associated with weight status in children aged 9–10 years. J Nutr 2011;141:453–459 [DOI] [PubMed] [Google Scholar]
- 50.Lazarou C, Newby PK. Use of dietary indexes among children in developed countries. Adv Nutr 2011;2:295–303 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Livingstone MB, Robson PJ, Wallace JM. Issues in dietary intake assessment of children and adolescents. Br J Nutr 2004;92(Suppl 2):S213–S222 [DOI] [PubMed] [Google Scholar]