

Abstract
Background
Research has shown that health literacy may be a stronger predictor of health than age, employment status, education level, race, and income. Evidence supports a strong link between low health literacy and poor dietary management of chronic diseases.
Objective
The aim was to evaluate the relationship of micronutrient quality of diet, health numeracy and health literacy in White and African American adults randomly selected from 13 Baltimore neighborhoods.
Design
Cross-sectional analysis of Wave 3 (2009–2013) of the longitudinal Healthy Aging in Neighborhoods of Diversity across the Life Span (HANDLS) study initiated in 2004.
Main Outcome Measures
Health literacy was measured using the Rapid Estimate of Adult Literacy in Medicine (REALM). Health numeracy was measured using the numeracy subscale of the Test of Functional Health Literacy in Adults (TOFHLA). Nutrient-based diet quality was measured using Mean Adequacy Ratio (MAR-S) scores calculated from 17 micronutrients from diet plus dietary supplement intake.
Statistical Analyses
The relationship of MAR-S scores to the health literacy measures were explored with multiple ordinary least square regression models, adjusting for a number of potential confounders.
Results
REALM but not numeracy was associated with MAR-S; significant covariates included age, current cigarette smoking status, and energy intake. The interactions of race and educational attainment, and REALM and educational attainment were significant, with the relationship between REALM and MAR-S becoming stronger as education level increased.
Conclusion
There is a synergistic relationship between health literacy and educational attainment in predicting nutrient-based diet quality. Education was a stronger predictor for Whites compared to African Americans emphasizing the need for health professionals to focus on both education and literacy when creating and providing diet and health-related interventions and resources.
Keywords: Health Literacy, Diet Quality, Numeracy, Dietary Supplement, African Americans
Introduction
Health literacy is defined as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” [1]. To be health literate, comprehensions as well as numeracy are needed [2]. Health numeracy is defined as “the degree to which individuals have the capacity to access, process, interpret, communicate, and act on numerical, quantitative, graphical, biostatistical, and probabilistic health information needed to make effective health decisions” [3]. Health numeracy is not only about understanding but also functioning with numeric concepts in terms of health. Analytical and decision-making skills in addition to the ability to read and comprehend prescription medication dosages, appointment forms, consent forms, and preparations for diagnostic testing require functional health literacy.
The National Assessment of Adult Literacy (NAAL) 2003 is still the United States’ most recent measure of adult health literacy for the nation’s population. This assessment found that 75 million adults had either basic or below basic health literacy [4]. The average health literacy for women, younger adults, Whites, and those living above the poverty threshold was higher than men, adults over 65 years old, African Americans, and those below the poverty threshold; respectively [5]. Lower health literacy was shown to be associated with uncontrolled blood pressure as well as decreased knowledge of symptoms of hypoglycemia in patients with diabetes [6, 7].
Health literacy and diet quality – assessed by the Healthy Eating Index (HEI-2005) and healthful eating practices – are associated positively [8, 9]. In addition, limited health literacy was associated with less dietary variety as well as limited preventive health behaviors such as low frequency of medical check-ups in older Japanese adults, residing in rural Japan [9]. Other studies found that health literacy correlated with nutrition skills such as estimation of portion size, understanding food labels, and seeking/trusting nutrition sources, all of which affect dietary quality [8, 10].
Diet quality can be evaluated based on food choices or nutrient intakes. The HEI, a primarily food-based quality index, measures compliance to the US Dietary Guidelines. However it does not assess micronutrient adequacy. The Mean Adequacy Ratio (MAR) is a method that compares nutrient intake of an individual to their Recommended Dietary Allowances (RDA). Since approximately half of the US population consumes dietary supplements, the use of the MAR method enables one to study the association of literacy with diet based on nutrients from only foods and from foods plus supplements.
To the best of our knowledge after a comprehensive literature review, there are no studies that evaluated the relationship between nutrient-based diet quality, calculated from total nutrient intakes (diet plus dietary supplements), and health literacy. The objective of the present study was to define the relationship between nutrient-based diet quality and health numeracy and literacy levels in Wave 3 participants of the Healthy Aging in Neighborhoods of Diversity across the Life Span (HANDLS) study. It was hypothesized that the association of health literacy with nutrient quality of the diet would be positive and statistically significant when dietary supplements were included in the assessment since the variance in nutrient intake would be increased between users and nonusers of dietary supplements.
Methods
Background on HANDLS Study
The HANDLS study, a National Institute on Aging sponsored longitudinal study that focuses on the influences of race and socioeconomic status (SES) on health in an urban population, was initiated in 2004. The baseline population was comprised of White (W) and African American (AA) men and women aged 30–64 years living in Baltimore, Maryland. A heuristic design was used to provide an equal sampling of four factors: age (7, 5-year age bands from 30–64 years), sex, race (AA and W), and SES (operationalized by household incomes below or above the 2004 125% of the Federal poverty guidelines). Further detailed information on the study design, eligibility and recruitment of participants can be found elsewhere [12].
The data collected for Wave 3 occurred in between 2009 and 2013. Participants were scheduled for two appointments approximately one week apart. The first appointment occurred on the Medical Research Vehicles and included a medical examination, first 24-hour dietary recall, cognitive evaluation, echocardiography, assessments of bone density and muscle strength, health literacy measures and laboratory measurements. The second appointment consisted of a telephone interview. The second 24-hour dietary recall and dietary supplement questionnaire were collected during this interview [13]. Study protocol was approved by human IRBs at MedStar Health Research Institute, the National Institute of Environmental Health Sciences, NIH and University of Delaware. All HANDLS participants provided written informed consent and were compensated monetarily.
Wave 3 HANDLS Study Population
The present sample consisted of 1,818 individuals who completed two 24-hour dietary recalls, the dietary supplement questionnaire, the Rapid Estimate of Adult Literacy in Medicine (REALM) and the Test of Functional Health Literacy in Adults (TOFHLA)(Figure 1). Those who did not meet these criteria were excluded from analysis. The study sample was compared to those excluded. There were no significant differences in terms of sex, race, drug use, smoking status, education, and marital status. However, the study sample had more participants above 125% of the Federal poverty guidelines and also had higher Mean Adequacy Ratio with Supplements (MAR-S), and REALM scores than those not included in this study sample.
Figure 1.
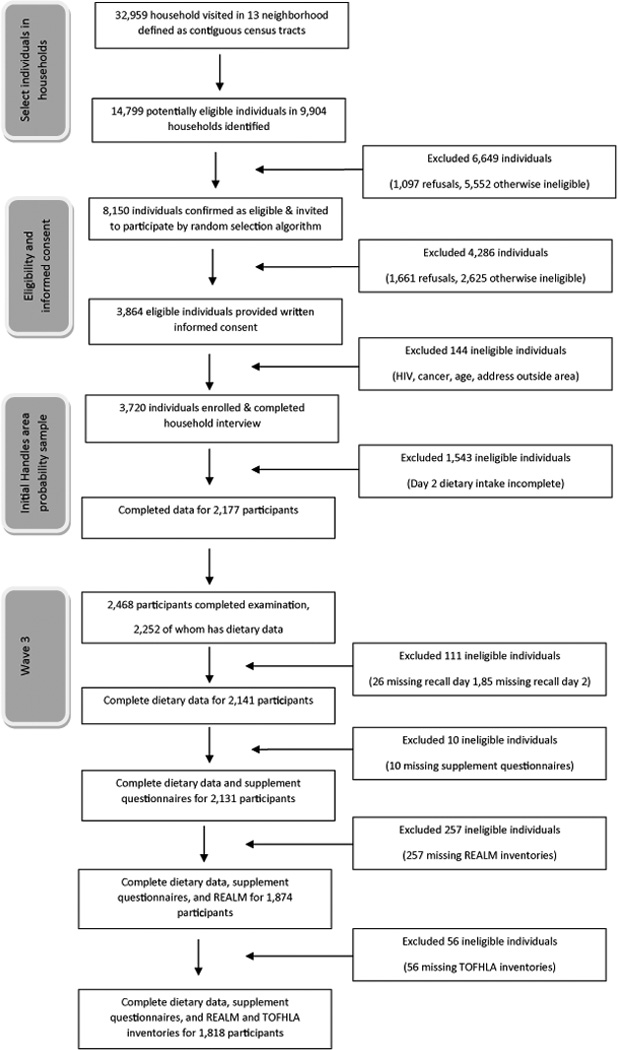
Healthy Aging in Neighborhoods of Diversity across the Life Span (HANDLS) study household screening, participant eligibility, and response rates from Baseline to Wave 3 to Current Analyses.
Dietary Intake Measures
Wave 3 of the HANDLS study used the United States Department of Agriculture’s Automated Multiple-Pass Method for collecting dietary data. Trained dietary interviewers collected the dietary intake of the person being interviewed for the previous 24-hour period from midnight to midnight. For both interviews, a food model booklet was given to the respondents in order to increase accuracy in measuring portion sizes [13]. After interviews were completed, recalls were processed through the Post-Interview Processing System and then foods were coded using Survey Net to match food from the Food and Nutrient Database for Dietary Studies, version 5.0, and assign nutrient values [14].
Dietary supplement information was collected from participants immediately after completion of the second 24-hour dietary recall [15]. This questionnaire gathered information on over-the-counter vitamin and mineral supplements, antacids, prescription supplements and antacids, and botanicals over the past month as well as the past 24-hours. Description of the calculation of nutrients obtained from dietary supplements is found on the HANDLS website [16].
Assessment of Nutrient Quality of Diet
Nutrient-based diet quality was assessed using the Nutrient Adequacy Ratio, MAR and MAR-S scores [17]. Nutrient Adequacy Ratio is defined as the ratio of the participant’s daily intake of a nutrient to his/her current Recommended Dietary Allowance (RDA) for that nutrient [18]. Thus RDA was adjusted for the age and sex of participants and vitamin C was adjusted for smokers [19]. Scores for 17 micronutrients: Vitamins A, C, D, E, B6, B12, folate, iron, thiamin, riboflavin, niacin, copper, zinc, calcium, magnesium, phosphorus, and selenium were calculated.
For this study, ratios were calculated based on nutrients contributed only by food (NAR) and contributed by foods plus dietary supplements (NAR-S). For individuals who did not consume dietary supplements their NAR-S score would be the same as their NAR score. The NAR and NAR-S scores were then converted into a percent with values exceeding 100 truncated to 100. The MAR and MAR-S formulas were: MAR= (∑NAR scores)/17 and MAR-S= (∑NAR-S scores)/17 [17]. All ratios were calculated for each recall day and then averaged.
Assessment of Health Literacy and Numeracy
The two inventories used to assess health literacy in Wave 3, namely the REALM and the TOFHLA numeracy were administered during the MRV examination. These tools were selected because they were well validated in a variety of populations, the items seemed relevant to HANDLS study participants and they best fit into the time available for their administration without adding significantly to the participant burden. The REALM is a word recognition test which focuses on medical-words and pronunciation from simple to more complex, multisyllabic words. A score of 66 is the highest, meaning all words were pronounced correctly [20]. TOFHLA-Numeracy was measured through 17 questions using prescription medication bottle labels, education information, registration forms, and diagnostic test instructions. The numeracy score was scaled to be out of 50 by multiplying by 2.941 [21].
In baseline HANDLS study no measures of health literacy were performed. Instead, general literacy was assessed measured by Wide Range Achievement Test, Version 3 (WRAT-3). The WRAT-3 was highly correlated with REALM. As a result, WRAT-3 was not included in the models used for this study to avoid multicollinearity.
Statistical Analyses
Descriptive statistics were calculated for demographic, literacy, and dietary data. REALM and TOFHLA were only moderately correlated, (r = 0.349), so both were included in the same model. Additionally, educational attainment and REALM (r = 0.320) and education attainment and TOFHLA (r = 0.182) were not highly correlated.
Multiple regression models were used to explore the relationship of MAR and MAR-S scores to the health literacy measures, after adjusting for potential confounders. Model one included all the main effects (sex, race, SES, age, education, current smoking status, current illicit drug use, and energy intake), model two included main effects and the health literacy and numeracy measures. Model three included all the main effects, health literacy and numeracy measure and the interactions between sex, education, and race. Illicit drug use was defined as current use of marijuana, opiates and/or cocaine. All model assumptions, normality, multicollinearity, linearity, and homoscedasticity were evaluated. These assumptions were tested using the Shapiro-Wilk test, Box-Cox test, inspection of residuals, and examining the condition index and variance inflation factor, respectively. A reflected square root transformation was done on the MAR and MAR-S scores to achieve normal distribution, therefore, the lower the transformed value the higher the MAR and MAR-S scores. Only the results for models with MAR-S will be presented since neither REALM nor TOHFLA were significant predictors of MAR.
An additional analysis examined whether health literacy and numeracy were related to supplement use (any use vs. none) differently between races. HANDLS study supplement users tended to be White, women, more educated, more likely to be >50 years old and non-smokers. A 2×2 between-subjects ANOVA was used for this analysis. Alpha was set to 0.05 as the level of significance for all tests.
Results
Sample Population
The sample was comprised of 1,105 African Americans (60.8%) and 713 Whites (39.2%) (Table 1). Approximately 41% of the sample was male and 59% female. Mean age was 53.1 years. Whites and men were more likely to be married compared to African Americans and women, respectively. White adults had significantly more years of education completed and fewer had incomes < 125% Federal poverty guidelines compared to African American adults (Table 1).
Table 1.
Characteristics of HANDLS cohort who participated in Wave 3 of the Healthy Aging in Neighborhoods of Diversity across the Life Span study and completed two 24-hour dietary recalls and health literacy measures. (n=1,818).
| Characteristics | African American | White | Race Comparison by Sex |
|||||
|---|---|---|---|---|---|---|---|---|
| Men n= 455 |
Women n= 650 |
P value | Men n= 293 |
Women n= 420 |
P value | P value Men |
P value Women |
|
| Demographics | ||||||||
| Age, year, X ± SE | 52.39 ± 0.42 | 53.29 ± 0.35 | 0.103 | 53.57 ± 0.53 | 53.04 ± 0.44 | 0.436 | 0.070 | 0.662 |
| Education, years, X±SE | 12.42 ± 0.14 | 12.42 ± 0.12 | 0.986 | 13.03 ± 0.18 | 12.96 ± 0.15 | 0.774 | 0.011 | 0.004 |
| SESa, <125% Federal poverty guidelines, % |
40% | 45.8% | 0.054 | 25.6% | 32.4% | 0.051 | <0.001 | <0.001 |
| Employed in last month, % | 63.6% | 54.9% | 0.004 | 69.5% | 57.9% | 0.002 | 0.099 | 0.355 |
| Currently married, % | 33% | 21.8% | <0.001 | 44.8% | 40.3% | 0.275 | 0.003 | <0.001 |
| Health Behaviors | ||||||||
| Current cigarette smoker, % | 54.1% | 40.1% | <0.001 | 33.2% | 38.6% | 0.209 | <0.001 | 0.279 |
| Current illicit drugb use, % | 27.4% | 15.6% | <0.001 | 14.4% | 9.5% | 0.082 | <0.001 | 0.015 |
| Literacy Measures | ||||||||
| REALMc, X ± SE | 56.11 ± 0.50 | 58.73 ± 0.41 | <0.001 | 61.20 ± 0.62 | 62.38 ± 0.51 | 0.137 | <0.001 | <0.001 |
| TOFHLAd, X ± SE | 44.13 ± 0.32 | 44.25 ± 0.27 | 0.768 | 44.62 ± 0.40 | 45.75 ± 0.33 | 0.028 | 0.347 | <0.001 |
| WRAT-3e, X ± SE | 41.14 ± 0.52 | 40.48 ± 0.43 | 0.330 | 44.25 ± 0.60 | 44.08 ± 0.50 | 0.829 | <0.001 | <0.001 |
| Health Status | ||||||||
| MARf X ± SE | 75.71 ± 0.63 | 71.18 ± 0.53 | <0.001 | 79.32 ± 0.79 | 75.08 ± 0.66 | <0.001 | <0.001 | <0.001 |
| MAR-Sg, X ± SE | 79.81 ± .535 | 77.94 ± .484 | 0.037 | 83.96 ± 0.607 | 81.18 ± .605 | 0.014 | <0.001 | 0.001 |
| Supplement user, % | 36.9% | 50.3% | <0.001 | 47.8% | 55.0% | 0.058 | 0.003 | 0.134 |
SES =Socioeconomic status;
Illicit drugs defined as marijuana, opiates, or cocaine;
REALM = Rapid Estimate of Adult Literacy in Medicine;
TOFHLA = Test of Functional Health Literacy in Adults;
WRAT-3 = Wide Range Achievement Test-version 3, determined in baseline wave;
MAR = Mean Adequacy Ratio based on nutrients from food;
MAR-S = Mean Adequacy Ratio with nutrients from supplements added
Significantly more African American men were current smokers compared to White men (Table 1). Within African Americans there was a significant difference between men and women, with a higher percentage of men being smokers and illicit drug users. There was also a significant difference between races within sex for illicit drug use. More African American adults were illicit drug users compared to White adults (Table 1).
On the REALM, African American women scored significantly higher than African American men. In addition, Whites scored significantly higher than African Americans (Table 1). White adults had health literacy scores indicative of > 9th grade reading level; African American adults had scores that indicated 7th–8th grade reading level. White women scored significantly higher on the TOFHLA-numeracy component compared to White men and African American women (Table 1). Similar to the REALM completed in Wave 3, Whites scored significantly higher than African Americans on the WRAT-3, measured at baseline (Table 1).
Approximately half of the African American women, White men and White women were supplement users compared to 37% of African American men. Men had significantly higher Mean Adequacy Ratios than women and Whites scored significantly higher than African Americans (Table 1).
Nutrient Quality of Diet and Health Literacy
After adjusting for total energy intake, REALM but not numeracy was a significant predictor of diet quality. In interpreting the main effects in context of the transformation of the nutrient quality scores, a negative association in the coefficient from Table 2, would be regarded as positive relationship. For example, the higher the energy intake the lower the reflected square root MAR-S; therefore, the higher the energy intake the higher the MAR-S. However, to interpret the direction of an interaction the directions of the main effects that comprise the interaction term must also be examined (Figure 2).
Table 2.
Multiple ordinary least square regression models revealed diet quality, measured by MAR-Sa Score was predicted by health literacy, measured by REALMb and selected demographics and lifestyles (n=1,818).
| Predictor | Model 1c | Model 2d | Model 3e | |||
|---|---|---|---|---|---|---|
| B (SE) | P value | B (SE) | P value | B (SE) | P value | |
| Sex (Men vs. Women) | 0.348 (0.091) | <0.001 | 0.322 (0.092) | <0.001 | −0.341 (0.387) | 0.378 |
| Race (African American vs. White) | 0.265 (0.088) | 0.003 | 0.229 (0.089) | 0.010 | −0.372 (0.372) | 0.317 |
| SESf (< 125% vs. ≥125% Federal poverty guidelines) |
−0.211 (0.090) | 0.019 | −0.169 (0.091) | 0.063 | 0.158 (0.091) | 0.081 |
| Age, years | −0.027 (0.005) | <0.001 | −0.027 (0.005) | <0.001 | −0.027 (0.005) | <0.001 |
| Education, years | −0.104 (0.014) | <0.001 | −0.091 (0.015) | <0.001 | 0.093 (0.107) | 0.386 |
| Current cigarette smoker | −0.096 (0.031) | 0.002 | −0.098 (0.031) | 0.001 | −0.094 (0.031) | 0.002 |
| Current Illicit drugg use | 0.092 (0.120) | 0.443 | 0.114 (0.120) | 0.343 | 0.116 (0.120) | 0.332 |
| Energy Intake | −0.001 (0.000) | <0.001 | −0.001 (0.000) | <0.001 | −0.001 (<0.001) | <0.001 |
| REALM | −0.011 (0.004) | 0.011 | 0.026 (0.017) | 0.142 | ||
| TOFHLAh | −0.003 (0.007) | 0.694 | −0.004 (0.007) | 0.600 | ||
| Sex* Race | −0.066 (0.174) | 0.705 | ||||
| Sex* Education | 0.046 (0.028) | 0.098 | ||||
| Race* Education | 0.055 (0.027) | 0.045 | ||||
| REALM* Education | −0.004 (0.002) | 0.025 | ||||
| R2 | 0.305 | <0.001 | 0.309 | <0.001 | 0.318 | <0.001 |
| ΔR2 | 0.005 | 0.021 | 0.009 | 0.005 | ||
MAR-S = Mean Adequacy Ratio based on diet and dietary supplements. Note: A reflected square root transformation was performed on MAR to achieve normal distribution;
REALM = Rapid Estimate of Adult Literacy in Medicine;
Model 1 includes all the main effects;
Model 2 includes the main effects, REALM and TOFHLA;
Model 3 includes all main effects, REALM, TOFHLA, and interactions between sex, education and race;
SES = Socioeconomic status;
Illicit drugs defined as marijuana, opiates, or cocaine;
TOFHLA = Test of Functional Health Literacy in Adults.
Figure 2.
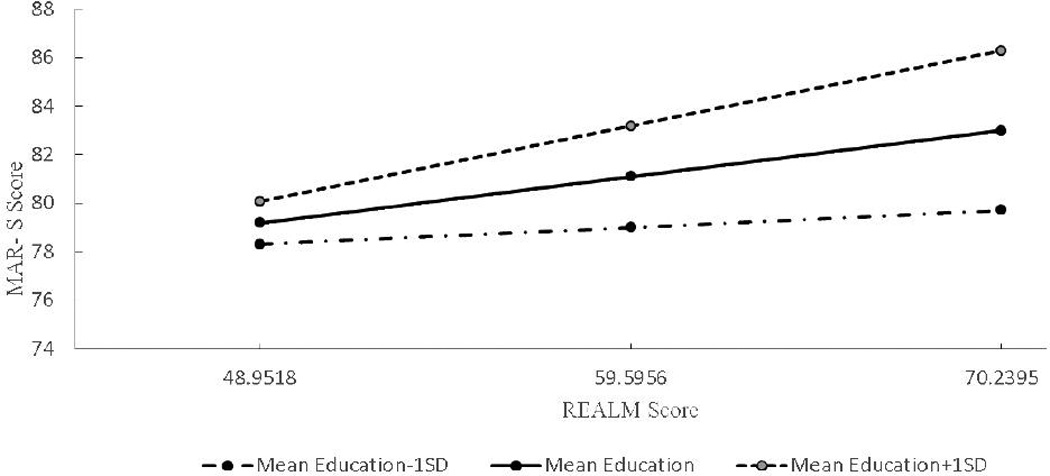
Moderation plot for the interaction between health literacy measured by REALMa and education for the Untransformed Mean Adequacy Score with Supplements (MAR-S) scores for African Americans and White adults in Wave 3 of the Healthy Aging in Neighborhoods of Diversity across the Life Span study. (a REALM = Rapid Estimate of Adult Literacy in Medicine)
There was a significant positive association between education and MAR-S, and between REALM and MAR-S. Since both of these effects were significant, their interaction was also examined (Table 2). As shown in Figure 2, there was a statistically significant relationship between REALM and MAR-S as education level increased. A significant interaction was also observed between race and education, revealing that education was a stronger predictor for Whites compared to African Americans (Table 2).This finding was also seen for the model using MAR (b(SE) = 0.038 (0.017), p = 0.028) and means micronutrient quality can vary more drastically based on educational levels, making a focus on educational level vital.
Discussion
To our knowledge, this is the first study to investigate the relationship of health literacy and numeracy on nutrient-based diet quality scores derived from both food plus dietary supplements. The findings provide evidence that health literacy was a significant predictor of diet quality based on total micronutrient intakes. The relationship between health literacy and diet quality was also stronger as education level increased. The findings of our study corroborate the synergistic relation of education with literacy reported by Kuczmarski et al [22]. An independent and synergistic association between literacy, measured by WRAT-3, and educational attainment in predicting diet quality assessed by the HEI-2010 was reported for participants examined in the baseline HANDLS study [22]. Thus two studies using the same lower income urban population over separate waves of a longitudinal study reveal that literacy impacts diet quality regardless of the evaluation approach, namely the HEI or MAR.
In our study, health literacy, measured by REALM, was significantly higher in urban White men and women compared to urban African American men and women, respectively. Zoellner et al [10] also found Whites had significantly higher health literacy scores compared to African Americans within a rural population. Although no health outcomes were examined in our study, researchers have found health literacy to impact health outcomes. McNaughton et al [6] evaluated the association between health literacy and blood pressure control. Results indicated that low health literacy, measured by REALM, was associated with uncontrolled blood pressure.
Patient education materials written at levels that exceed the literacy skills of target audiences are ineffective [7, 23]. Among HANDLS participants, approximately 48% of African Americans and 26% of Whites read at or below an 8th grade level [17]. These results are comparable to the NAAL which found most adults read at an 8th grade level, and almost 20% of adults read at a 5th grade level [24, 25]. Others have reported health materials are written at 9th grade level, a level above the literacy of approximately 37% of HANDLS study participants [4, 26]. Therefore, these participants may not understand brochures describing ways to improve their diet.
The National Cancer Institute’s National Work Group on Literacy and Health recommended preparing health education materials at the 5th grade reading level to target low literacy/low education audiences [27, 28]. If materials are targeted to the 5th grade level it would meet the needs of almost 92% of HANDLS participants, based on REALM scores. Avoiding medical jargon, especially polysyllabic words, and breaking down information into simple concrete ideas may increase the likelihood of comprehension [29]. The study findings emphasize the need for dietitians, nutritionists, and other health educators to be aware of their clients’ literacy abilities, using appropriate language and nutrition education materials to encourage improvement in dietary intakes. Our data suggest how important it is to create well designed health education materials targeted to vulnerable populations given eliminating health disparities and achieving health equity among all American sub-populations is a goal of Healthy People 2020.
There are several strengths of this study. The HANDLS study targets a large, understudied population of socioeconomically diverse African American and White adults. Independent demographic analysis found that the HANDLS study population is representative of 14 other US cities with similar population densities and racial distributions [30]. Also, the method of dietary collection was based on two 24-hour dietary recalls which allowed for analysis of typical dietary intake in normal and overweight individuals [31]. Another strength is this study evaluated the relationship between health literacy and numeracy with diet quality measured from nutrients from food plus nutrients from dietary supplements, providing a more complete picture of nutrient intake.
There are also limitations to this study. These data were cross-sectional making it impossible to determine the direction of effects. In addition, although two 24-hour recalls were used for dietary collection, there is still the possibility of bias due to underreporting by participants. Another limitation is the omission of food insecurity in the regression model, which could affect diet quality. The findings are limited in generalizability to persons slightly above the Federal poverty guidelines since the analytical sample included more Wave 3 HANDLS participants with incomes above compared to below 125% of the Federal poverty guidelines.
Conclusion
Health literacy was a predictor of nutrient-based diet quality with higher literacy associated with higher quality scores for HANDLS study participants. Those with higher education levels had significantly higher diet quality compared to those with lower education levels. The study’s findings support the indisputable influence of educational attainment and health literacy in nutritional and health status and outcomes. Furthermore, they highlight the need to provide relevant, comprehensible materials to improve diet quality which may ultimately diminish the prevalence of obesity and obesity-related disorders among poor and minority communities.
Acknowledgments
This work is supported by the Intramural Research Program, National Institute on Aging, National Institutes of Health, grant Z01-AG000194.
References
- 1.Ratzan SC, Parker RM. Selden C, Zorn M, Ratzan S, Parker R. Health literacy (CBM 2000-1). Current Bibliographies in Medicine 2000-1. US National Library of Medicine; [cited 2016 Mar 31]. Introduction, page vi. Updated 2000; Available from: https://www.nlm.nih.gov/archive/20061214/pubs/cbm/hliteracy.pdf. [Google Scholar]
- 2.Boswell C, Cannon S, Aung K, Eldridge J. An application of health literacy research. Appl Nurs Res. 2004;17(1):61–64. doi: 10.1016/j.apnr.2003.12.001. [DOI] [PubMed] [Google Scholar]
- 3.Golbeck AL, Ahlers-Schmidt CR, Paschal AM, Dismuke SE. A definition and operational framework for health numeracy. Am J Prev Med. 2005;29(4):375–376. doi: 10.1016/j.amepre.2005.06.012. [DOI] [PubMed] [Google Scholar]
- 4.National assessment of adult literacy (NAAL): Health literacy component. National Center for Education Statistics; [cited 2016 Mar 31]. Updated 2003; Available from: http://nces.ed.gov/naal/fct_hlthliteracy.asp. [Google Scholar]
- 5.Nielsen-Bohlman L, Panzer A, Kindig D. Health literacy: A prescription to end confusion. Institute of Medicine of the National Academies; 2004. [cited 2016 Mar 31]. Available from: http://www.nap.edu/openbook.php?record_id=10883&page=32. [PubMed] [Google Scholar]
- 6.McNaughton CD, Jacobson TA, Kripalani S. Low literacy is associated with uncontrolled blood pressure in primary care patients with hypertension and heart disease. Patient Educ Couns. 2014;96(2):165–170. doi: 10.1016/j.pec.2014.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ad hoc committee on health literacy for the council on scientific affairs, American Medical Association. Health Literacy: Report of the council on scientific affairs. JAMA. 1999;281(6):552–557. [PubMed] [Google Scholar]
- 8.Cha E, Kim KH, Lerner HM, Dawkins CR, Bello M, Umpierrez G, et al. Health literacy, self-efficacy, food label use, diet in young adults. Am J Health Behav. 2014;38(3):331–339. doi: 10.5993/AJHB.38.3.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Yoshida Y, Iwasa H, Kumagai S, Suzuki T, Yoshida H. Limited functional health literacy, health information sources, and health behavior among community-dwelling older adults in Japan. ISRN Geriatrics. 2014 Doi: http://dx.doi.org/10.1155/2014/952908. [Google Scholar]
- 10.Zoellner J, You W, Connell C, Smith-Ray RL, Allen K, Tucker KL, et al. Health literacy is associated with healthy eating index scores and sugar-sweetened beverage intake: Findings from the rural lower Mississippi delta. J Am Diet Assoc. 2011;111(7):1012–1020. doi: 10.1016/j.jada.2011.04.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bailey RL, Gahche JJ, Lentino CV, Dwyer JT, Engel JS, Thomas PR, et al. Dietary supplement use in the United States, 2003–2006. J Nutr. 2011;141(2):261–266. doi: 10.3945/jn.110.133025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Evans MK, Lepkowski JM, Powe NR, LaVeist T, Kuczmarski MF, Zonderman AB. Healthy Aging in Neighborhoods of Diversity Across the Life Span (HANDLS): overcoming barriers to implementing a longitudinal, epidemiologic, urban study of health, race, and socioeconomic status. Ethn Dis. 2010;20(3):267–275. [PMC free article] [PubMed] [Google Scholar]
- 13.Evans MKZA. Healthy Aging in Neighborhoods of Diversity Across the Life Span (HANDLS) Study Wave 3 Protocol. National Institute on Aging; [cited 2016 Mar 31]. Updated 2009; Available from: http://handls.nih.gov/pdf/02Protocol-Wave03-2013-05-17.pdf. [Google Scholar]
- 14.USDA automated multiple-pass method. United States Department of Agriculture; [cited 2016 Mar 31]. Available from: http://www.ars.usda.gov/News/docs.htm?docid=7710. [Google Scholar]
- 15.Healthy Aging in Neighborhoods of Diversity across the Life Span Homepage. National Institute on Aging. [cited 2016 Mar 31];HANDLS Dietary Supplement Data. Available from: http://Handls.nih.gov/06Coll-w03DietSupplements.htm.
- 16.Healthy Aging in Neighborhoods of Diversity across the Life Span Study Dietary Supplement Documentation Codebook. [cited 2016 Mar 31];Appendix 13. Description of Statistical Analysis to Create Supplemental Nutrient File. Available from: https://handls.nih.gov/06Coll-w03DietSupplements.htm.
- 17.Fanelli Kuczmarski M, Mason MA, Beydoun MA, Allegro D, Zonderman AB, Evans MK. Dietary patterns and sarcopenia in an urban African American and white population in the united states. J Nutr Gerontol Geriatr. 2013;32(4):291–316. doi: 10.1080/21551197.2013.840255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Murphy SP, Foote JA, Wilkens LR, Basiotis PP, Carlson A, White KK, et al. Simple measures of dietary variety are associated with improved dietary quality. J Am Diet Assoc. 2006;106(3):425–429. doi: 10.1016/j.jada.2005.12.003. [DOI] [PubMed] [Google Scholar]
- 19.Institute of Medicine. Dietary reference intakes for vitamin C, vitamin E, selenium, and carotenoids. Washington DC: National Academies Press; 2000. Chapter 5. Vitamin C; p. 95. [PubMed] [Google Scholar]
- 20.Davis TC, Long SW, Jackson RH, Mayeaux EJ, George RB, Murphy PW, et al. Rapid estimate of adult literacy in medicine: A shortened screening instrument. Fam Med. 1993;25(6):391–395. [PubMed] [Google Scholar]
- 21.Parker RM, Baker DW, Williams MV, Nurss JR. The test of functional health literacy in adults: a new instrument for measuring patients' literacy skills. J Gen Intern Med. 1995;10(10):537–541. doi: 10.1007/BF02640361. [DOI] [PubMed] [Google Scholar]
- 22.Fanelli Kuczmarski M, Beydoun MA, Cotugna N, Pryor L, Mason MA, Zonderman AB, et al. Literacy contributes to greater diet quality in a socioeconomically diverse urban population. Top Clin Nutr. 2016;31(1):47–58. [Google Scholar]
- 23.Byun J, Golden DW. Readability of patient education materials from professional societies in radiation oncology: Are we meeting the national standard? Int J Radiat Oncol Biol Phys. 2015;91(5):1108–1109. doi: 10.1016/j.ijrobp.2014.12.035. [DOI] [PubMed] [Google Scholar]
- 24.Kirsch IS, Jungeblut A, Jenkins L, Kolstad A. Adult literacy in America: A first look at the results of the National Adult Literacy Survey. Washington, DC: National Center for Education Statistics, Educational testing service; 1993. [Google Scholar]
- 25.Dreger V, Tremback T. Optimize patient health by treating literacy and language barriers. AORN J. 2002;75(2):280–285. 287, 289–293. [PubMed] [Google Scholar]
- 26.Cotugna N, Vickery CE, Carpenter-Haefele KM. Evaluation of literacy level of patient education pages in health-related journals. J Community Health. 2005;30(3):213–219. doi: 10.1007/s10900-004-1959-x. [DOI] [PubMed] [Google Scholar]
- 27.Communicating with patients who have limited literacy skills. Report of the National Work Group on Literacy and Health. J Fam Pract. 1998;46(2):168–176. [PubMed] [Google Scholar]
- 28.Carbone ET, Zoellner JM. Nutrition and health literacy: A systematic review to inform nutrition research and practice. J Acad Nutr Diet. 2012;112(2):254–265. doi: 10.1016/j.jada.2011.08.042. [DOI] [PubMed] [Google Scholar]
- 29.Hersh L, Salzman B, Snyderman D. Health literacy in primary care practice. Am Fam Physician. 2015;92(2):118–124. [PubMed] [Google Scholar]
- 30.Lepkowski J. HANDLS Generalizabiliy, 2010 and HANDLS principle cities cluster analysis. National Institutes on Aging. 2011 [Google Scholar]
- 31.Moshfegh AJ, Rhodes DG, Baer DJ, Murayi T, Clemens JC, Rumpler WV, et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am J Clin Nutr. 2008;88(2):324–332. doi: 10.1093/ajcn/88.2.324. [DOI] [PubMed] [Google Scholar]