

Abstract
Objective:
To determine the amount of sugar and pH in commercially available soft drinks in Jazan, Saudi Arabia. This was further compared with their labeled values in order to inform the regulations. The effects of these drinks on teeth is reviewed.
Materials and Methods:
Ten brands of popular soft drinks including 6 regular carbonated drinks and 4 energy drinks were obtained from the local markets. Their pH was determined using a pH meter. The amount of total sugar, glucose, fructose, and sucrose was estimated using high performance liquid chromatography (using Dionex ICS 5000 ion chromatography) at the Saudi Food and Drug Authority. Descriptive statistics was done to obtain the mean and standard deviation. Intergroup comparison was performed using independent t-test, and the labeled and estimated values within the group were compared with paired t-test.
Results:
The labeled and estimated sugar in energy drinks (14.3 ± 0.48 and 15.6 ± 2.3, respectively) were higher than the carbonated drinks (11.2 ± 0.46 and 12.8 ± 0.99), which was statistically significant. In addition, there was a significant difference in the concentration of glucose in energy drinks (5.7 ± 1.7) compared to carbonated drinks (4.1 ± 1.4). The pH of these drinks ranged from 2.4 to 3.2. The differences between the estimated and labeled sugar in carbonated drinks showed statistical significance. Mild variation was observed in total sugar, glucose, fructose, and sucrose levels among different bottles of the same brand of these drinks.
Conclusion:
The low pH and high sugar content in these drinks are detrimental to dental health. Comparison of the estimated sugar with their labeled values showed variation in most of the brands. Preventive strategies should be implemented to reduce the health risks posed by these soft drinks.
Key words: Dental caries, energy drinks, pH, Saudi Arabia, soft drinks, sucrose, sugars, tooth erosion
INTRODUCTION
There is a drastic change in food consumption pattern in Saudi Arabia. In recent years, soft drinks have become increasingly available in the market, with a surge in their usage, especially among young people and children.[1] This has resulted in a major concern considering their health implications. The increasing incidence of obesity and type II diabetes among children is mostly associated with the consumption of excessive amount of sugar present in these beverages.[2] It is also associated with increased risk of bone fractures or osteoporosis, probably because of decreased calcium absorption due to the presence of phosphorus in these drinks. Moreover, the intake of dairy products is reduced by soft drink consumption, which has an impact on bone mineral density.[3] From the dental perspective, the inherent acids and sugars in the soft drinks have both erosive and cariogenic potential.[4,5,6,7,8,9,10,11,12,13]
A dynamic relationship exists between the sugars in these drinks and teeth. They affect the integrity of the teeth by altering the pH of the saliva as well as dental plaque. These sugars are metabolized to acids by plaque bacteria, which in turn lowers plaque and salivary pH, causing tooth demineralization. Several studies have shown direct relationship between dental caries and soft drinks.[4,5,10,11,12,13] Tooth erosion is progressive loss of tooth substance by acids that does not involve bacteria. The erosive potential of soft drinks depends on total titrable acids along with their pH.[9] A positive correlation has been shown between the excessive consumption of these drinks and dental erosion.[4,6,7,8,9]
A recent review on dental caries has reported an increase in the prevalence and severity in Saudi Arabian population during the last decade. Moreover, secular trends also show a striking increase in the dmft/DMFT index and caries prevalence rates over the past few decades.[14] The sugars present in soft drinks are one of the contributing factors to dental caries. In view of the increased consumption of soft drinks, this study aims to determine the quantity of total sugar, glucose, fructose, sucrose, and pH in a range of commercially available soft drinks in Jazan, Saudi Arabia. In order to further inform regulation, we also compared the estimated values with the labeled concentration. A brief review of the effect of these drinks on dental tissue is presented.
MATERIALS AND METHODS
Ten popular brands of soft drinks including 6 regular carbonated drinks and 4 energy drinks were obtained randomly from local markets/supermarkets of Jazan, Saudi Arabia. Two bottles from each brand with a different batch number and date of production were purchased. All the 20 study samples had 10-month usage period from their production date. The amount of sugar mentioned in their labels was noted. Except for two brands of carbonated drinks, all the other brands had printed their values on the label. A sample of bottled water was taken as control. All the bottles were stored in their original closed containers at room temperature until analysis. The pH was measured immediately after removing the bottle cap using a pH meter (Mi 150, Martini Instruments). Later, a 100 ml sample was transferred to a sterile container and coded so that the type and brand was unknown to the technician to avoid bias. The concentration of total sugar, glucose, fructose, and sucrose in these samples were determined. The measurement was done twice for each sample to check the reliability. The analysis was done using high performance liquid chromatography on a Dionex ICS 5000 ion chromatography system. All the measurements were made at the Riyadh Food control laboratory, Saudi Food and Drug authority (SFDA).
The data were entered in a Microsoft excel sheet and statistically analyzed using the SPSS Statistics for Windows, Version 17.0. Chicago: SPSS Inc. Descriptive statistics was done to obtain the mean and standard deviation. Independent t-test was done to check the significant differences for sugar, glucose, fructose, sucrose, and pH between the sample groups, whereas the difference between the labeled and estimated sugar among the sample group was analyzed using the paired t-test.
RESULTS
The mean comparison of sugar, glucose, fructose, sucrose, and pH between the sample groups is displayed in Table 1. Both the labeled and estimated sugar in energy drinks (14.3 ± 0.48 and 15.6 ± 2.3, respectively) were higher than the regular carbonated drinks (11.2 ± 0.46 and 12.8 ± 0.99, respectively), which was statistically significant. In addition, there was a significant difference in the concentration of glucose between energy drinks (5.7 ± 1.7) and carbonated drinks (4.1 ± 1.4). Though insignificant, the amount of fructose was comparatively more in energy drinks (5.6 ± 1.6), whereas the sucrose content and pH was almost the same for both the drinks. The pH of these soft drinks ranged from 2.4 to 3.2, which is well below the critical pH level for enamel dissolution. The pH of bottled water was approximately neutral and their sugar concentration was negligible. Comparison of estimated sugar value with those printed on their labels is presented in Table 2. The paired differences between the estimated and labeled sugar in carbonated drinks was statistically significant. Meanwhile, two brands of carbonated drinks did not display their values on the label. The amount of estimated sugar among different bottles of the same brand showed variation ranging from 0.05 to 2 g/dl for carbonated drinks and 0.8 to 5 g/dl for energy drinks. Variation was also observed in the concentration of glucose, fructose, and sucrose among different bottles of the same brand of soft drinks.
Table 1.
Comparison of labeled and estimated total sugar, levels of estimated sugar components, and pH within the sample groups
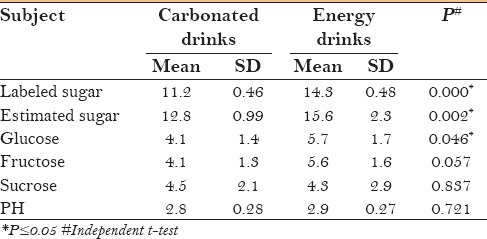
Table 2.
Comparison between labeled and estimated sugar levels

DISCUSSION
World Health Organization has recommended to limit the daily intake of sugars to just 5% of total calories which is equivalent to 6 teaspoons or 25 grams of sugar per day.[15] The American Heart Association (AHA) recommends that the daily intake of sugar should be 25 grams for women, 38 grams for men, and 12 grams for children.[16]
The first study that describes the effect of fermentable carbohydrates on plaque pH dates back to 1943 by Stephan and Miller.[17] Though the total amount of sugar does not considerably affect the caries process, it is well recognized that factors such as frequency of consumption, duration of exposure, quantity and quality of saliva, and oral hygiene determines the cariogenicity. Dietary sugars upon consumption will diffuse rapidly into plaque which are then metabolized to acids or stored as extra and intracellular polysaccharides by cariogenic bacteria. All monosaccharides and disaccharides are fermented at the same rate and are highly cariogenic.[18] Sucrose, however, is unique and regarded as arch criminal for dental caries initiation. It acts as a substrate for the production of extracellular storage of polysaccharides (glucans and fructans) and insoluble matrix polysaccharides (mutans), which increase the stickiness of the plaque.[19] The colonization of cariogenic Streptococcus mutans on teeth is also enhanced by sucrose.[20] It further reduces the concentration of calcium and phosphate in the oral biofilm, thereby limiting the remineralization of the initial carious lesion. All these factors together contribute to the high cariogenicity of sucrose.[21] Moreover, sucrose is the most common sugar in the human diet. Its cariogenicity is high upon fermentation followed by glucose and fructose.[22,23] In this study, despite the presence of almost equal concentration of sucrose in both carbonated and energy drinks, their level was slightly higher than glucose and fructose in carbonated drinks. Though the total amount of sugar was more in energy drinks, the concentration of glucose and fructose was higher than sucrose.
Mild variation was observed in the levels of sugar, glucose, fructose, and sucrose in different bottles of the same brand of carbonated and energy drinks. This variation is due to the fact that the acidic pH of these drinks can cause hydrolysis of sugar upon storage, which can reduce their concentration.[24] Comparison of the estimated values of sugar with those printed on their label showed variation in most of the brands. This difference was statistically significant for carbonated drinks. This may be probably due to printing of labels in bulk by the manufacturers to label their products. The pH of these drinks determines the degree of saturation of hydroxyapatite mineral in tooth enamel.[25] When the pH is less than the critical pH (5.5), the solution is unsaturated and the mineral from tooth enamel will tend to dissolve until the solution becomes saturated. However, it is not only the pH but also the presence of minerals such as calcium, phosphate, and fluoride in these drinks that determine the degree of saturation with respect to tooth minerals. A recent study conducted by Tadakamadla et al. showed that carbonated drinks have more enamel solubility due to their pH and titrable acidity.[26] All the samples in this study had very low pH, below the critical value, and can cause demineralization of calcium phosphates of tooth mineral. Furthermore, research has shown that pH is a crucial factor that can cause dental erosion and caries more than the sucrose present in these drinks.[25]
The total carbohydrate content of the tested soft drinks was rather high (11.28 ± 0.23 to 16.46 ± 3.52 g/dl). Frequent intake of these beverages pose a major risk for dental caries, which is further influenced by their intake pattern. Constant sipping or holding the drinks in contact with the teeth for prolonged duration aggravates the cariogenicity of these beverages.[12] Dental caries is highly prevalent in this country, especially among adults.[27] A population-based study showed increase in prevalence and severity of dental caries among children involving 80% of their primary dentition and 70% of their permanent dentition.[28] It, therefore, requires immediate action by the health officials of Saudi Arabia. This is only possible by devising appropriate preventive strategies, which requires a thorough understanding of the factors that cause dental caries. As the colonization of S. mutans in dental plaque appears to be sucrose dependent, measures that reduce sugar intake constitute effective preventive measures in caries control. It is advisable to reduce the intake of fermentable carbohydrates, especially the sugared beverages. Consumption of moderate amount of these drinks is acceptable, especially during mealtime, which should be followed immediately by intake of foods that buffer the acids. Artificial sweeteners or sugar substitutes have been developed as an alternative to fermentable sugars to overcome their health issues. The beverage industry has introduced the diet form of carbonated drinks by substituting added sugars with artificial sweeteners. They are non-cariogenic as oral bacteria cannot ferment these sugar substitutes to produce acids. However, diet drinks have erosive potential equivalent to sugared carbonated drinks.[29]
Dental caries can be prevented primarily by reduction in the consumption of soft drinks, increasing the intake of mineral rich drinking water and foods, and oral health education and promotion. Preventive strategies should be implemented to reduce the health risks posed by soft drinks and explore the use of sugar substitutes and dairy products to prevent dental caries and erosion.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
The authors would like to express their gratitude to Riyadh food control laboratory at Saudi Food and Drug Authority (SFDA) for carrying out the analysis for sugar component levels, and the Medical Research Centre at Jazan University for pH measurement, both were done free of cost. The study did not receive financial support from any source.
REFERENCES
- 1.Özen AE, Bibiloni MM, Pons A, Tur JA. Fluid intake from beverages across age groups: A systematic review. J Hum Nutr Diet. 2015;28:417–42. doi: 10.1111/jhn.12250. [DOI] [PubMed] [Google Scholar]
- 2.Imamura F, Connor L, Ye Z, Mursu J, Hayashino Y, Bhupathiraju SN, et al. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: Systematic review, meta-analysis and estimation of population attributable fraction. BMJ. 2015;351:h3576. doi: 10.1136/bmj.h3576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Høstmark AT, Søgaard AJ, Alvær K, Meyer HE. The Oslo health study: A dietary index estimating frequent intake of soft drinks and rare intake of fruit and vegetables is negatively associated with bone mineral density. J Osteoporos. 2011:102686. doi: 10.4061/2011/102686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tahmassebi JF, Duggal MS, Kotru GM, Curzon MEJ. Soft drinks and dental health: A review of the current literature. J Dent. 2006;34:2–11. doi: 10.1016/j.jdent.2004.11.006. [DOI] [PubMed] [Google Scholar]
- 5.Kumar S, Acharya S, Vasthare R, Singh SK, Gupta A, Debnath N. Dental caries experience in high risk soft drinks factory workers of South India: A comparative study. Ind J Dent Res. 2014;25:174–7. doi: 10.4103/0970-9290.135913. [DOI] [PubMed] [Google Scholar]
- 6.Johansson AK, Johansson A, Birkhed D, Omar R, Baghdadi S, Carlsson GE. Dental erosion, soft-drink intake, and oral health in young Saudi men, and the development of a system for assessing erosive anterior tooth wear. Acta Odontol Scand. 1996;54:369–78. doi: 10.3109/00016359609003554. [DOI] [PubMed] [Google Scholar]
- 7.Araújo NC, Massoni ACLT, Katz CRT, Rosenblatt A. Dental erosion and consumption of industrialized beverages in a group of children in Recife/Pernambuco, Brazil. Rev Odonto Ciênc. 2009;24:120–3. [Google Scholar]
- 8.Kannan A, Ahmed MAA, Duraisamy P, Manipal S, Adusumillil P. Dental hard tissue erosion rates and soft drinks - A gender based analysis in Chennai city, India. Saudi J Dent Res. 2014;5:21–7. [Google Scholar]
- 9.Jawale BA, Bendgude V, Mahuli AV, Dave B, Kulkarni H, Mittal S. Dental plaque pH variation with regular soft drink, diet soft drink and high energy drink: An in vivo study. J Contemp Dent Pract. 2012;13:201–4. doi: 10.5005/jp-journals-10024-1121. [DOI] [PubMed] [Google Scholar]
- 10.Quadri FA, Hendriyani H, Pramono A, Jafer M. Knowledge, attitudes and practices of sweet food and beverage consumption and its association with dental caries among schoolchildren in Jazan, Saudi Arabia. East Mediterr Health J. 2015;21:403–11. doi: 10.26719/2015.21.6.403. [DOI] [PubMed] [Google Scholar]
- 11.Al-Malik MI, Holt RD, Bedi R. The relationship between erosion, caries and rampant caries and dietary habits in preschool children in Saudi Arabia. Int J Paediatr Dent. 2001;11:430–9. [PubMed] [Google Scholar]
- 12.Decker RT, Loveren CV. Sugars and dental caries. Am J Clin Nutr. 2003;78:881S–92S. doi: 10.1093/ajcn/78.4.881S. [DOI] [PubMed] [Google Scholar]
- 13.Cheng R, Yang H, Shao MY, Hu T, Zhou X. Dental erosion and severe tooth decay related to soft drinks: A case report and literature review. J Zhejiang Univ Sci B. 2009;10:395–9. doi: 10.1631/jzus.B0820245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Al-Ansari AA. Prevalence, severity, and secular trends of dental caries among various saudi populations: A literature review. Saudi J Med Sci. 2014;2:142–50. [Google Scholar]
- 15.Guideline: Sugars intake for adults and children. Geneva: World Health Organization; 2015. [PubMed] [Google Scholar]
- 16.Johnson RK, Appel L, Brands M, Howard B, Lefevre M, Lustig RH, et al. Dietary sugars intake and cardiovascular health: A scientific statement from the American Heart Association. Circulation. 2009;120:1011–20. doi: 10.1161/CIRCULATIONAHA.109.192627. [DOI] [PubMed] [Google Scholar]
- 17.Stephan RM, Miller BF. A quantitative method for evaluating physical and chemical agents which modify production of acids in bacterial plaques on human teeth. J Dent Res. 1943;22:45–53. [Google Scholar]
- 18.Neff D. Acid production from different carbohydrate sources in human plaque in situ. Caries Res. 1967;1:78–87. doi: 10.1159/000259502. [DOI] [PubMed] [Google Scholar]
- 19.Gupta P, Gupta N, Pawar AP, Birajdar SS, Natt AS, Singh HP. Role of Sugar and Sugar Substitutes in Dental Caries: A Review. ISRN Dent. 2013:519421. doi: 10.1155/2013/519421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Roshan NM, Sakeenabi B. Practical problems in use of sugar substitutes in preventive dentistry. J Int Soc Prev Community Dent. 2011;1:1–8. doi: 10.4103/2231-0762.86373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Paes Leme AF, Koo H, Bellato CM, Bedi G, Cury JA. The Role of Sucrose in Cariogenic Dental Biofilm Formation-New Insight. J Dent Res. 2006;85:878–87. doi: 10.1177/154405910608501002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cury JA, Rebelo MA, Del Bel Cury AA, Derbyshire MT, Tabchoury CP. Biochemical composition and cariogenicity of dental plaque formed in the presence of sucrose or glucose and fructose. Caries Res. 2000;34:491–7. doi: 10.1159/000016629. [DOI] [PubMed] [Google Scholar]
- 23.Utreja D, Tewari A, Chawla HS. A study of influence of sugars on the modulations of dental plaque pH in children with rampant caries, moderate caries and no caries. J Indian Soc Pedod Prev Dent. 2010;28:278–81. doi: 10.4103/0970-4388.76158. [DOI] [PubMed] [Google Scholar]
- 24.Martin-Villa MC, Vidal-Valverde C, Rojas-Hidalgo E. Soluble sugars in soft drinks. Am J Clin Nutr. 1981;34:2151–3. doi: 10.1093/ajcn/34.10.2151. [DOI] [PubMed] [Google Scholar]
- 25.Inukai J, Nakagaki H, Itoh M, Tsunekawa M, Watanabe K. Recent trends in sugar content and pH in contemporary soft drinks. J Dent Child. 2011;78:138–42. [PubMed] [Google Scholar]
- 26.Tadakamadla J, Kumar S, Ageeli A, Vani NV, Babu M. Enamel solubility potential of commercially available soft drinks and fruit juices in Saudi Arabia. Saudi J Dent Res. 2015;6:106–9. [Google Scholar]
- 27.Khan SQ, Khan NB, Ar Rejaie AS. Dental caries. A Meta analysis on a Saudi population. Saudi Med J. 2013;34:744–9. [PubMed] [Google Scholar]
- 28.Al Agili DE. A systematic review of population-based dental caries studies among children in Saudi Arabia. Saudi Dent J. 2013;25:3–11. doi: 10.1016/j.sdentj.2012.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Roberts MW, Wright JT. Nonnutritive, low Caloric Substitutes for Food Sugars: Clinical Implications for Addressing the Incidence of Dental Caries and Overweight/Obesity. Int J Dent. 2012:625701. doi: 10.1155/2012/625701. [DOI] [PMC free article] [PubMed] [Google Scholar]