

Abstract
Objectives:
Diabetes mellitus (DM) is a common chronic metabolic disorder which affects millions of people. At present, India has the highest incidence of diabetes worldwide. Several oral lesions and conditions are associated with diabetes. However, there is a lack of consensus among researchers regarding the relationship between DM and dental caries. Hence, the present study was carried out to assess the dental caries prevalence among type II diabetic and nondiabetic adults attending a hospital in Ahmedabad city.
Materials and Methods:
A hospital-based cross-sectional study was conducted. One hundred and twenty diabetics individuals attending the diabetic Outpatient Department (OPD) and age and sex-matched 120 nondiabetic individuals from general OPD were included in the study. The data were gathered through semi-close-ended questionnaire and clinical examination. Dental caries was assessed by using the World Health Organization's 2013 proforma. Data was analyzed by applying Student's independent t-test or one-way analysis of variance.
Results:
Dental caries prevalence among the diabetic group was 73.33% and 33.33% among the nondiabetic group. Dental caries prevalence and mean dental caries was significantly higher among uncontrolled diabetic individuals than that among controlled diabetic individuals. Duration of the disease and dental caries prevalence did not show any significant difference.
Conclusion:
Dental caries prevalence was significantly high among diabetic individuals compared with nondiabetic individuals. Close collaboration between the patients, healthcare units, and oral health professionals could be a way of improving diabetic patients' general and oral health.
Key words: Dental caries, diabetes, oral health
INTRODUCTION
Diabetes mellitus (DM) is a common chronic metabolic disorder affecting millions of people. According to the World Health Organization (WHO), any disease having a prevalence of more than 1% should be considered as a disease of public health importance.[1] The prevalence of diabetes for all age groups worldwide was estimated to be 2.8% in 2000 and may reach 4.4% by 2030.[2] According to Roglic et al.[3] almost 3 million deaths per year are attributed to diabetes, which is equivalent to 5.2% of all deaths. India, with 32 million diabetic individuals, currently has the highest incidence of diabetes worldwide; these numbers are predicted to increase to 80 million by the year 2030.[4] The two broad categories of DM are type I and type II. Type II DM which is characterized by increased blood glucose level and obesity is mostly seen after 30 years of age.[5]
Oral cavity and contagious structures can be dramatically affected by diabetes. These oral complications have important effects on quality of life of patients with diabetes and can also directly and indirectly affect glycemic control.[6] Oral lesions and conditions associated with diabetes include xerostomia, burning mouth, gingivitis, periodontal disease, dental caries, and candidal infection.[7] The relationship between diabetes and dental caries, particularly among adults, has received less attention so far despite of the fact that both the diseases are associated with ingestion of carbohydrates[8,9] and that insulin deficiency in diabetes may lead to hyposalivation and elevated salivary glucose level, which may put diabetic patients at a high risk of developing caries.[10]
Taylor et al. concluded in their literature review that there was insufficient evidence to determine whether a relationship exists between diabetes and coronal or root caries risk and recommended that further investigations should be carried out.[11] Published literature clearly suggests that previous caries experience is one of the best predictor to know about future caries development.[10] So far none of the studies attempted to assess the burden of dental caries among diabetic individuals in Ahmedabad city. Hence, the present study was carried out to assess the dental caries prevalence among type II diabetic and nondiabetic adults in Ahmedabad city.
MATERIALS AND METHODS
A hospital-based cross-sectional study was conducted among diabetic and nondiabetic population attending the V.S. General Hospital, Ahmedabad, India. This hospital is managed by Ahmedabad Municipal Corporation and receives patients mainly from the low and middle social class. Ethical clearance was obtained from the Institutional Review Board, and permission to examine the patients and record their personal data was obtained from the concerned authorities of the hospital.
Inclusion and exclusion criteria
Individuals in the age group of 35–74 years without any major health problems were included in the study. Individuals having type I or gestational diabetes or any mental or physical disorders not permitting oral examination were excluded. The control group included age and gender-matched healthy volunteers with no history of diabetes.
Sampling methodology
To evaluate the proportion of dental caries in people with type II diabetes and nondiabetics with a P < 0.05 and 90% power, the required sample size was calculated. The prevalence of dental caries was calculated from the pilot study, which yielded a sample size of 205. However, to achieve a power of 95% for the present study, a total of 240 participants were examined, which included 120 diabetics and 120 nondiabetics. A simple random sampling method was followed. Patients attending the diabetic OPD and who fulfilled the inclusion criteria were selected for the study. For diabetic patients, the glycosylated hemoglobin concentration (HbA1c) level was used to assess the glycemic control.[12] Those with levels less than or equal to 7 mmol/ml were classified as indicating satisfactory (good) control of diabetes while the values more than 7 mmol/ml were classified as poor control of diabetes.[13]
Nondiabetics (control group) were selected from general OPD and were matched by age and sex. Nondiabetics were tested for random blood sugar level using a glucometer (Acu-Check Active), and participants with random blood sugar level less than 200 mg/dl were included in the study.
Data collection
The data were collected through semi-close-ended questionnaire and clinical examination. The study participants were first explained regarding the purpose and nature of the study. After obtaining informed consent, they were involved in a face-to-face interview to get information regarding demographic details and medical history. Medical history records included were duration of the diabetes, physician follow-up, and degree of the control of the diabetic state. The questionnaire was filled by the examiner to ensure uniformity in data collection as well as to avoid misinterpretation of the questions by the study subjects. The questionnaire was pretested during the pilot study.
Dental caries was assessed using WHO 2013 proforma.[14] The interview was followed by the clinical examination, which was conducted by a single examiner who was trained and calibrated in the Department of Public Health Dentistry, AMC Dental College and Hospital, Ahmedabad. The kappa value for the intraexaminer reliability was calculated to be 0.85. Participants were seated comfortably on an ordinary chair for the examination. The examination was done under natural daylight using a plain mouth mirror and CPITN “C” probe. Data collection was done from June 2014 to December 2014.
Statistical analysis
Statistical analysis was done using the Statistical Package for the Social Sciences software version 16. Prevalence of dental caries was compared between the study groups using Chi square test, and mean values were compared between the study groups using either Student's independent t-test or one-way analysis of variance to identify the significant groups. The level of significance was kept at 0.05%.
RESULTS
Table 1 shows prevalence of dental caries among the study participants. Dental caries prevalence among the diabetic group was 73.33% and 30.83% among the nondiabetic group. The result was statistically significant.
Table 1.
Prevalence of dental caries among the study participants
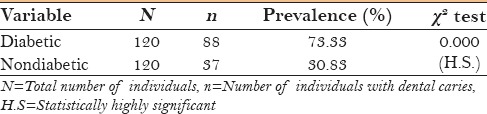
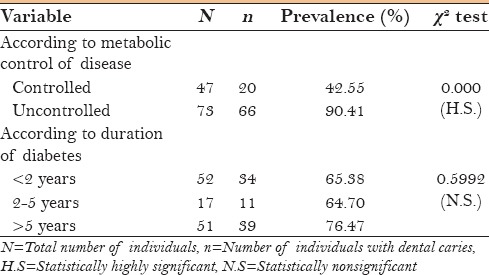
Table 2 shows the prevalence of dental caries among diabetic individuals according to the metabolic control of the disease and duration of the disease. Uncontrolled diabetic individuals had a significantly higher prevalence of dental caries (90.41%) than controlled diabetic individuals (42.55%). Participants were divided into three groups (<2 years, 2–5 years, and >5 years) according to the duration of diabetes. No significant difference in caries prevalence was found among the diabetic individuals according to the duration of diabetes.
Table 2.
Prevalence of dental caries among the diabetic individuals according to metabolic control of disease and duration of diabetes
The caries experience and its components showed the mean of Decayed Teeth (DT), Missing Teeth (MT), and Filled Teeth (FT) component, as well as mean DMFT for diabetes group was higher than the mean for the nondiabetic group. The statistical comparison showed that there were significant differences among caries experience for MT and DMFT components (P < 0.05), whereas mean DT and FT components did not show significant difference (P > 0.05) [Table 3].
Table 3.
Mean dental caries experience among the study participants

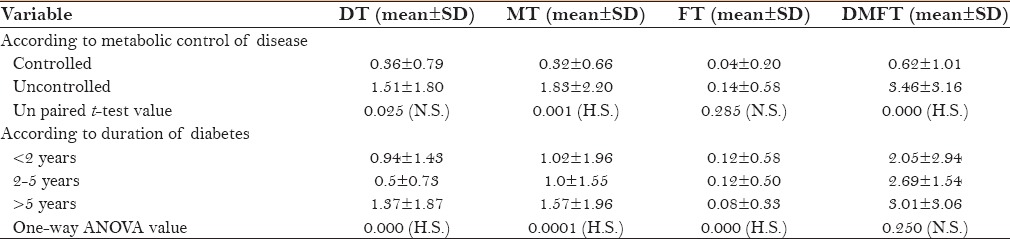
Table 4 shows mean dental caries experience among diabetic individuals according to the metabolic control of the disease and the duration of the diabetes. Mean dental caries experience among uncontrolled diabetic individuals was 3.46 ± 3.16 whereas it was 0.62 ± 1.01 in controlled diabetic individuals. The result was statistically significant. Mean number of missing teeth was significantly higher among metabolically uncontrolled individuals whereas the mean number of decayed and filled teeth did not show any significant difference among uncontrolled and controlled individuals. Mean DT and MT was significantly increasing as the duration of disease increased, whereas mean FT was significantly higher among people having diabetes less than 2 years. Mean DMFT component was higher among people having diabetes more than 5 years but it did not show any statistical significant difference.
Table 4.
Mean dental caries experience among the diabetic individuals according to metabolic control of disease and duration of diabetes
DISCUSSION
The prevalence of dental caries and its burden on the general population is of significant public health interest. Reduction of untreated dental caries and tooth extractions as a consequence of dental caries among adults by 15% are among the Healthy People 2010 objectives for oral health.[15] Therefore, it is important to identify patients who may be at particularly high risk of dental caries. DM, a significant public health problem in its own right, may increase one's susceptibility to dental caries.[16] In addition, people with diabetes are also more prone to infections, including dental abscesses that result from progressive dental caries. Therefore, the present hospital-based cross-sectional study was conducted to assess and compare dental caries of diabetic patients with that of nondiabetics to add additional information to the existing literature.
The prevalence of dental caries was significantly higher among diabetic patients than nondiabetic patients. Several other authors have reported similar findings[8,10,13,17,18,19,20,21,22] while some authors have reported no difference[4,7,23,24,25] and few have reported low prevalence of dental caries among diabetics.[1,26,27] Regarding differences in caries indicators, in the present study, patients with diabetes had significantly more DMFT and more teeth missing due to caries compared to the patients not diagnosed with diabetes. These findings are consistent with the studies reported by Reddy et al.,[8] Singh et al.,[9] Taylor et al.,[11] Kanjirath et al.,[17] and Lalla et al.,[28] whereas they are not in agreement with the studies reported by Hawraa[7] and Gupta et al.[26] The high caries might be because of more frequent meals in diabetic patients than normal patients and repeated intakes of even small amount of carbohydrates may be cariogenic when coupled with elevated blood glucose level and hyposalivation.[29,30] Another reason might be because the patients with diabetes do not have access to oral health services as often as individuals without diabetes. The reasons for disparity were not explored but may be because of lack of awareness on the part of patients with diabetes regarding the oral complications of the disease and a perceived lack of time for this additional health care activity when patients are busy with management of their diabetes.[6]
In this study, it was observed that the severity of dental caries increased with increase in the blood glucose level with positive correlation, and dental caries prevalence was significantly higher in metabolically uncontrolled patients compared to metabolically well-controlled patients. The results are in agreement with the studies reported by Chavez et al.[31] and not in agreement with the studies reported by Hawraa,[7] Arreita-Blannco et al.,[32] and Sandberg et al.[33] The result may be attributed to elevated salivary glucose levels and low salivary flow, which may predispose this population to increased caries risk because of lack of insulin or insulin resistance.[10,18] Elevated salivary glucose level favors the growth of Lactobacilli and Streptococcus mutans bacteria,[9,18,23] and hyposalivation may result in low buffering activity which is needed for remineralization of early carious lesions.[34]
Regarding the effect of the duration of the disease on caries experience, the results showed that there was no significant difference in caries prevalence as well as DMFT teeth between the groups based on duration of the disease. These results were consistent with some studies that reported that there was no relationship between the duration of diabetes and caries experience,[7,32,35] whereas disagreed with other studies which reported greater experience in individuals with a longer disease duration.[9,17]
It must be emphasized that the results of this study may not be directly comparable with the results of others. This is due to many differences such as the population size and selection criteria for diabetic and nondiabetic groups. Because this was a hospital-based study, the results may not be generalized which suggests a larger scale, community level research in this field. Oral microbial counts, quantity and flow rate of saliva, dental visits, and oral hygiene data which may be useful were not considered in the present study. Within the limitations of the present study, the results indicated that type II DM patients were at a high risk of caries development. Close collaboration between the patient, the healthcare units, and oral health professionals could be a way of improving diabetic patients' general and oral health.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Puranik MA, Hiremath SS. Oral health status and treatment needs among adult diabetic and non diabetic patients in Banglore city- A comparative study. J Indian Assoc Public Health Dent. 2006;4:31–7. [Google Scholar]
- 2.Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–53. doi: 10.2337/diacare.27.5.1047. [DOI] [PubMed] [Google Scholar]
- 3.Roglic G, Unwin N, Bennett PH, Mathers C, Tuomilehto J, Nag S, et al. The burden of mortality attributable to diabetes realistic estimates for the year 2000. Diabetes Care. 2005;28:2130–5. doi: 10.2337/diacare.28.9.2130. [DOI] [PubMed] [Google Scholar]
- 4.Reddy CVK, Kesavan R, Ingle N. Dentition status and treatment needs among type II diabetic and non diabetic individuals in Chennai City- A comparative study. J Oral Health Comm Dent. 2011;5:79–85. [Google Scholar]
- 5.Bangash RY, Khan AU, Tariq KM, Yousaf A. Oral aspects and complications in type 2 diabetes mellitus – A study. Pak Oral Dent J. 2012;32:296–9. [Google Scholar]
- 6.Ira BL. Diabetes and oral health- current concepts regarding periodontal disease and dental caries. US Endocrinol. 2012;8:93–7. [Google Scholar]
- 7.Hawraa KA. The relationship between the dental caries and the blood glucose level among type II non insulin dependent diabetic patients. J Bagh Coll Dent. 2012;24:108–14. [Google Scholar]
- 8.Reddy CVK, Maurya M. A comparative study to assess the oral health status and treatment needs of diabetic and non diabetic population attending some of the hospitals in Mysore city. J Indian Assoc Public Health Dent. 2008;12:1–14. [Google Scholar]
- 9.Singh A, Thomas S, Dagli R, Katti R, Solanki J, Bhateja GA. To access the effects of salivary factors on dental caries among diabetic patients and non diabetic patients in Jodhpur city. J Adv Oral Res. 2014;5:10–4. [Google Scholar]
- 10.Moin M, Malik A. Frequency of dental caries and level of risk among type II diabetics. Dentistry. 2015;5:334–8. [Google Scholar]
- 11.Taylor GW, Manz MC, Borgnakke WS. Diabetes, periodontal disease, dental caries and tooth loss: A review of the literature. Compend Contin Educ Dent. 2004;25:179–88. [PubMed] [Google Scholar]
- 12.American Diabetes Association. Standard medical care on patients with diabetes mellitus. Diabetes Care. 2005;28:4–36. [Google Scholar]
- 13.Sadia I, Farhat K, Saad A, Muhammad M, Ayyaz AK. Dental caries and diabetes. Pak Oral Dent J. 2011;31:58–61. [Google Scholar]
- 14.World Health Organization. Oral Health Surveys- Basic Methods. 5th ed. Geneva: 2013. [Google Scholar]
- 15.Healthy People 2010: Oral health objectives. 2008. Oct. [Last accessed on 2016 Jan 07]. Available from: http://www.cdc.gov/oralhealth/topics/healthy_people.htm#2 .
- 16.Ship JA. Diabetes and oral health: An overview. J Am Dent Assoc. 2003;134:4S–10. doi: 10.14219/jada.archive.2003.0367. [DOI] [PubMed] [Google Scholar]
- 17.Kanjirath PP, Inglehart MR, Habil P. Diabetes and oral health: The importance of oral health related behavior. The Journal of Dental Hygiene. 2011;85:264–72. [PubMed] [Google Scholar]
- 18.Singh I, Singh P, Singh A, Singh T, Kaur R. Diabetes an inducing factor for dental caries: A case control analysis in Jammu. J Int Soc Prev Community Dent. 2016;6:125–9. doi: 10.4103/2231-0762.178748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Pearce EI, Dong YM, Yue L, Gao XJ, Purdie GL, Wang JD. Plaque minerals in the prediction of caries activity. Community Dent Oral Epidemiol. 2002;30:61–9. doi: 10.1034/j.1600-0528.2002.300109.x. [DOI] [PubMed] [Google Scholar]
- 20.Cao X, Wang D, Zhou J, Yuan H, Chen Z. Relationship between dental caries and metabolic syndrome among 13998 middle-aged urban Chinese. J Diabetes. 2016 doi: 10.1111/1753-0407.12424. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 21.Seethalakshmi C, Reddy RC, Asifa N, Prabhu S. Correlation of Salivary pH, Incidence of Dental Caries and Periodontal Status in Diabetes Mellitus Patients: A Cross-sectional Study. J Clin Diagn Res. 2016;10:12–4. doi: 10.7860/JCDR/2016/16310.7351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kampoo K, Teanpaisan R, Ledder RG, McBain AJ. Oral bacterial communities in individuals with type 2 diabetes who live in southern Thailand. Appl Environ Microbiol. 2014;80:662–71. doi: 10.1128/AEM.02821-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hintao J, Teanpaisan R, Chongsuvivatwong V, Dahlen G, Ratarasan C. Root surface and coronal caries in adults with type 2 diabetes mellitus. Community Dent Oral Epidemiol. 2001;35:302–9. doi: 10.1111/j.1600-0528.2007.00325.x. [DOI] [PubMed] [Google Scholar]
- 24.Ribeiro LS, Santos JN, Vieira CL, Caramelli B, Ramalho LM, Cury PR. Association of dental infections with systemic diseases in Brazilian Native Indigenous: A cross-sectional study. J Am Soc Hypertens. 2016;10:413–9. doi: 10.1016/j.jash.2016.02.012. [DOI] [PubMed] [Google Scholar]
- 25.Kogawa EM, Grisi DC, Falcao DP, Amorim IA, Rezende TM, da Silva IC, et al. Impact of glycemic control on oral health status in type 2 diabetes individuals and its association with salivary and plasma levels of chromogranin A. Arch Oral Biol. 2016;62:10–9. doi: 10.1016/j.archoralbio.2015.11.005. [DOI] [PubMed] [Google Scholar]
- 26.Gupta VK, Malhotra S, Sharma V, Hiremath SS. The Influence of Insulin Dependent Diabetes Mellitus on Dental Caries and Salivary Flow. Int J Chronic Dis. 2014;2014:790898. doi: 10.1155/2014/790898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bissong M, Azodo CC, Agbor MA, Nkuo-Akenji T, Fon PN. Oral health status of diabetes mellitus patients in Southwest Cameroon. Odontostomatol Trop. 2015;38:49–57. [PubMed] [Google Scholar]
- 28.Lalla RV, D’Ambrosio JA. Dental management considerations for the patients with diabetes mellitus. J Am Dent Assoc. 2001;132:1425–32. doi: 10.14219/jada.archive.2001.0059. [DOI] [PubMed] [Google Scholar]
- 29.Al-Khateeb TL, AL-Amoudi NH, Fatani HH, Mira SA, Ardawi MS. Periodontal disease and caries experience of diabetic patients in Arabian community. Saudi Dent J. 1990;2:91–5. [Google Scholar]
- 30.Novotna M, Podzimek S, Broukal Z, Lencova E, Duskova J. Periodontal Diseases and Dental Caries in Children with Type 1 Diabetes Mellitus. Mediators Inflamm. 2015;2015:379626. doi: 10.1155/2015/379626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Chavez EM, Taylor GW, Borrell LN, Ship JA. Salivary function and glycemic control in older persons with diabetes. Oral Sur Oral Med Oral Path Oral Radio Endod. 2000;89:305–11. doi: 10.1016/s1079-2104(00)70093-x. [DOI] [PubMed] [Google Scholar]
- 32.Arrieta-Blanco JJ, Bartolome-Villar B, Jimenez- Martinez E, Saavedra-Vallejo P, Arrieta-Blanco FJ. Bucco-dental problems in patients with diabetes mellitus: Index of plaque and dental caries. Med Oral. 2003;8:97–109. [PubMed] [Google Scholar]
- 33.Sandberg GE, Sundberg HE, Fjellstrom CA, Wikblad KF. Type 2 diabetes and oral health. A comparison between diabetic and non-diabetic subjects. Diabetes Res Clin Pract. 2000;50:27–34. doi: 10.1016/s0168-8227(00)00159-5. [DOI] [PubMed] [Google Scholar]
- 34.Yeh CK, Harris SE, Mohan S, Horn D, Fajardo R. Hyperglycemia and xerostomia are key determinants of tooth decay in type 1 diabetic mice. Lab Invest. 2012;92:868–82. doi: 10.1038/labinvest.2012.60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lin BP, Taylor GW, Allen DJ, Ship A. Dental caries in older adults with diabetes mellitus. Spec Care Dentist. 1999;19:8–14. doi: 10.1111/j.1754-4505.1999.tb01361.x. [DOI] [PubMed] [Google Scholar]