

Abstract
Current recommendations for diagnosing myelodysplastic syndromes endorse flow cytometry as an informative tool. Most flow cytometry protocols focus on the analysis of progenitor cells and the evaluation of the maturing myelomonocytic lineage. However, one of the most frequently observed features of myelodysplastic syndromes is anemia, which may be associated with dyserythropoiesis. Therefore, analysis of changes in flow cytometry features of nucleated erythroid cells may complement current flow cytometry tools. The multicenter study within the IMDSFlow Working Group, reported herein, focused on defining flow cytometry parameters that enable discrimination of dyserythropoiesis associated with myelodysplastic syndromes from non-clonal cytopenias. Data from a learning cohort were compared between myelodysplasia and controls, and results were validated in a separate cohort. The learning cohort comprised 245 myelodysplasia cases, 290 pathological, and 142 normal controls; the validation cohort comprised 129 myelodysplasia cases, 153 pathological, and 49 normal controls. Multivariate logistic regression analysis performed in the learning cohort revealed that analysis of expression of CD36 and CD71 (expressed as coefficient of variation), in combination with CD71 fluorescence intensity and the percentage of CD117+ erythroid progenitors provided the best discrimination between myelodysplastic syndromes and non-clonal cytopenias (specificity 90%; 95% confidence interval: 84–94%). The high specificity of this marker set was confirmed in the validation cohort (92%; 95% confidence interval: 86–97%). This erythroid flow cytometry marker combination may improve the evaluation of cytopenic cases with suspected myelodysplasia, particularly when combined with flow cytometry assessment of the myelomonocytic lineage.
Introduction
Discriminating between cytopenia due to myelodysplastic syndromes (MDS) and cytopenia due to other (non-clonal) causes can be challenging, especially when dysplasia as assessed by cytomorphology does not fulfill the diagnostic criteria of MDS according to WHO1, and when other MDS-associated features are absent (e.g., >15% ring sideroblasts (RS) and/or cytogenetic aberrations). Current recommendations for the diagnosis of MDS endorse flow cytometry (FC) as a valuable additional diagnostic tool. In this respect, it has been recommended to follow the guidelines set down by the International/European LeukemiaNet Working Group for FC in MDS (IMDSFlow).2–4
Despite the fact that FC for MDS correlates with cytomorphology, the sensitivity of current validated FC scores for diagnosing MDS requires improvement.5–8 So far, most of the designed FC scores have comprised the analysis of the (im)mature myelomonocytic lineage with a median sensitivity of 75% for identifying MDS (median specificity, 94%; see Westers et al.4). Since anemia is frequently observed in MDS, often accompanied by erythroid dysplasia, analysis of immunophenotypic changes of nucleated erythroid cells (NEC) may complement current FC analysis.9,10 Thus far, this has not been studied in great detail. Integration of results from analysis of the erythroid lineage to the primarily myelomonocytic and progenitor cell-based FC scores may improve sensitivity of FC analysis in MDS.8;11–13
Incorporating erythroid markers in FC protocols requires knowledge of normal erythroid differentiation, and of potential aberrancies and pitfalls. The characteristic morphological stages of normal erythroid differentiation are reflected by their light scatter properties and by their differential expression of CD45, CD117, CD105, CD36, CD71 and/or CD235a (Figure 1).14–17 Some of the FC aberrancies that have been reported to reflect MDS-related dyserythropoiesis are: a) an increased number of NEC within total nucleated cells; b) an altered proportion of consecutive erythroid differentiation stages, such as an increased number of immature erythroid cells (CD117+ and/or CD105+) or, by contrast, a decrease in erythroid progenitors; c) an abnormal pattern of CD71 versus CD235a; d) a reduced expression of CD71 and/or CD36; and e) an overexpression of CD105. Most of these aberrancies are present in 70–80% of MDS cases.8,11–13,15,18–22 However, a number of features may be shared across the spectrum of non-clonal cytopenias.23–25
Figure 1.
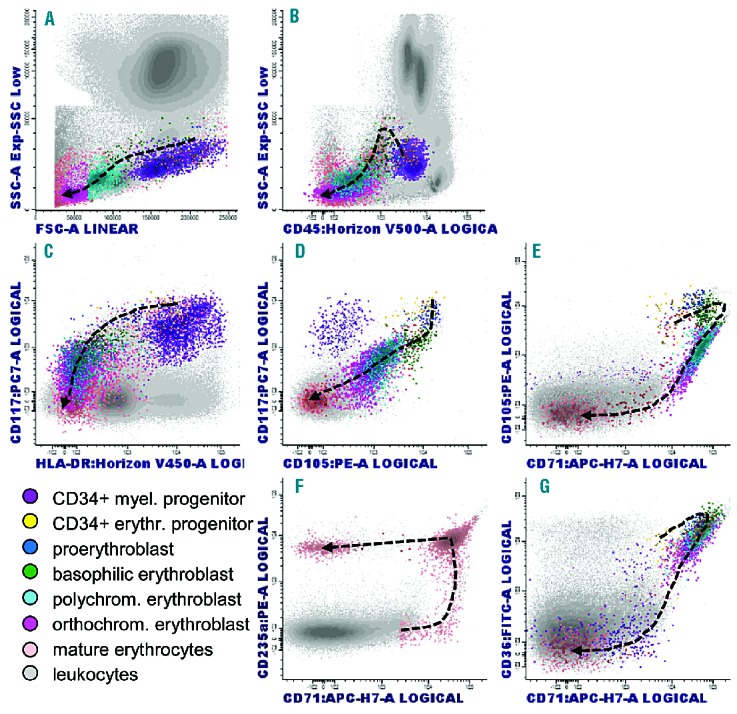
Flow cytometric profiles of normal erythroid differentiation. Early erythroid precursors are defined as CD45dim/SSCint/CD34+/CD117+/CD105+/CD235a−, proerythroblasts as CD45dim/−/SSCint/CD34−/CD117+/CD105+/CD36+/CD71+/CD235a+, basophilic erythroblasts as CD45dim/−/SSCint/CD117−/CD105+/CD36++/CD71+/CD235a+, polychromatic erythroblasts as CD45−/SSClow/FSCint/CD105−/CD36+/CD71+/CD235a+ and orthochromatic erythroblasts CD45−/SSClow/FSClow/CD36+/−/CD71+/CD235a+. Indicated colors reflecting erythroid subsets are not visible in the CD71 vs. CD235a plot (Fig 1F). Herein, pink colored cells represent the total erythroid lineage in this plot. Mature erythrocytes (CD45−/CD36−/CD71−/CD235a++) can be seen in improperly lysed cell preparations (Figure 1F). Reticulocytes are not covered in these graphs, but they may appear as CD71dim-to-negative in non-lysed cell preparations. Myeloid progenitors are CD34+/CD117+/HLA-DR+/CD105− (Figure 1C and D.); these cells have slightly higher CD45 expression than erythroid precursors; moreover, in contrast to myeloid progenitors erythroid cells do not express HLA-DR (adapted from references14–16).
The multicenter study reported herein focused on defining the erythroid FC parameters that enable distinction of dyserythropoiesis associated with MDS from non-clonal cytopenias. Hereto, data from a learning cohort were compared between MDS patients and controls, and the results were validated in a separate cohort.
Methods
MDS patients and controls
Nineteen centers (members of the IMDSFlow group) collected FC data on the erythroid lineage in low grade MDS cases (<5% blasts) and controls. Data were acquired from bone marrow samples taken from 1008 patients and healthy controls after informed consent in accordance with the Declaration of Helsinki; where required, local ethics committee approval was obtained. The learning cohort comprised 677 cases (18 centers, data collected between October 2012 and September 2013), and the validation cohort comprised 331 cases (9 centers, data collected between December 2013 and April 2014). Inclusion criterion for pathological controls was cytopenia not associated with MDS. In total, data on 374 MDS cases, 443 pathological and 191 normal controls were collected (specified in Tables 1 and 2). Information regarding age, gender, cytomorphology and cytogenetics was requested. One center with limited access to cytomorphology results only included MDS patients with typical features of MDS as the presence of more than 15% RS and/or MDS-associated cytogenetic anomalies. In 325/374 MDS cases, sub-classification according to the WHO-20081 was provided. The median contribution per center to the total study cohort was 47 cases (range 6–100); the median number of erythroid FC markers analyzed per case was 7 (range 1–9 of 10 proposed markers).
Table 1.
Characteristics of MDS patients and controls in the learning and validation cohorts.
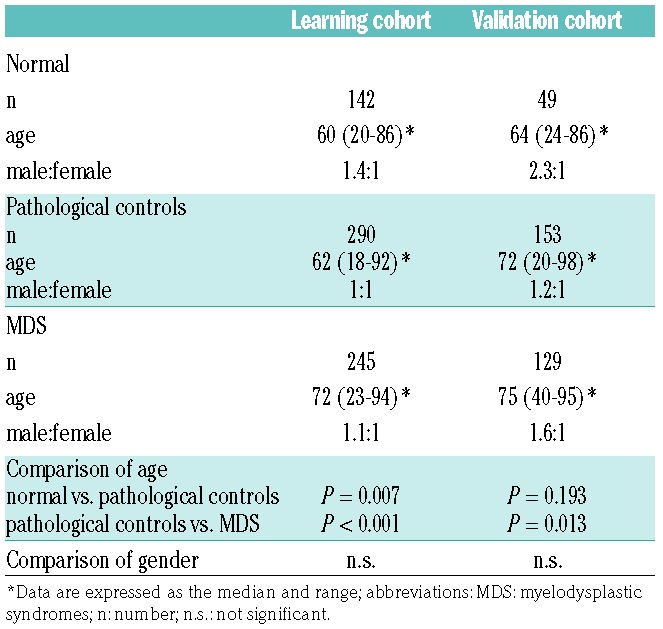
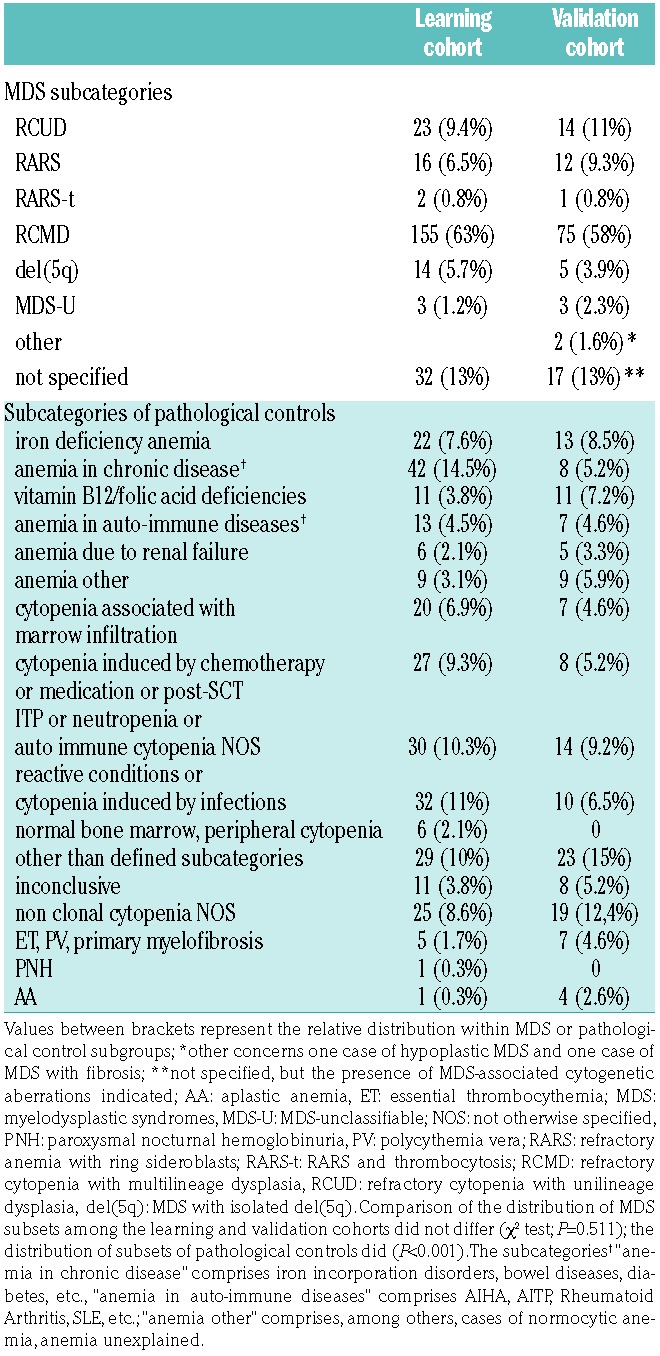
Table 2.
Subcategories of MDS and pathological controls in the learning and validation cohort.
Sample preparation and antibody combinations
Flow cytometric analysis in MDS requires the removal of mature, enucleated erythrocytes through the use of lysis protocols. The vast majority of centers used ammonium chloride-based solutions, either home-made or commercial (e.g., PharmLyse; BD Biosciences, San Jose, CA); two centers used FACSLyse (BD Biosciences), and one other used VersaLyse (Beckman Coulter, Miami, FL). FACSLyse contains a fixative, whereas VersaLyse is recommended for use with a fixative when the sample contains anticoagulants other than EDTA. The duration of lysis and temperature varied among centers (5–25 minutes and 4–37°C, respectively), but most lysed for 10 minutes (n=10) at room temperature (n=16). Two centers reported the use of an additional fixative in their staining protocols, both in combination with an ammonium chloride-based lysing solution. Detailed information can be found in Online Supplementary Information. Most centers used the IMDSFlow-recommended stain-lyse-wash procedure; five centers performed stain-lyse-wash. Antibody combinations were similar between centers, but clones and fluorochromes differed. Most centers used a backbone of CD45 and CD34 and/or CD117, and added antibodies such as CD235a, CD71, CD36, and CD105. Examples of antibody combinations and panels have been described previously.3,26,27 Nuclear dyes were not routinely included in the panels, and only one center applied the live/dead stain 7-AAD. The flow cytometers used included: FACSCalibur (BD Biosciences; n=3); FACS CANTO-II (BD Biosciences; n=10); a combination of FACSCalibur and FACS CANTO-II (both BD Biosciences; n=2); and Navios (Beckman Coulter; n=4). Panels comprised 4-, 5-, 6-, 8- and/or 10-color FC; WinList7.0 (Verity Software House, Topsham, ME), Kaluza (Beckman Coulter), CellQuestPro, FACS-DIVA (both BD Biosciences), and/or Infinicyt (Cytognos, Salamanca, Spain) software packages were used for data analysis.
Gating strategy and data collection
The gating strategy was discussed during the IMDSFlow meeting in 2011 and re-evaluated in 2012. All participants performed FC analysis of the erythroid lineage defined as CD45dim-to-negative and SSClow-to-intermediate. It is noteworthy that the initially proposed gating strategy (erythroid lineage defined by CD45 negativity) was altered to include early erythroid precursors that are within the CD45dim cell population.3,4,13 Six or more color panels enabled the inclusion of a myeloid-defining marker such as CD13 or CD33, and a more accurate separation of myeloid and erythroid progenitors. Moreover, to exclude platelets and platelet aggregates, a combination of scatter properties and CD36high/CD71− was suggested. The final gating strategy was distributed among all centers (detailed information in Online Supplementary Information).
The following parameters were collected: the percentage of NEC within all nucleated cells; the expression pattern of CD71 versus CD235a; the percentage of CD71dimCD235a+ cells within the CD71/CD235a pattern; CD71 and CD36 expression levels; the percentage of CD117+ cells in the erythroid compartment; CD105 expression level and the percentage of CD105+ cells in the erythroid compartment. Recent knowledge, such as the finding that CD71 and CD36 expression represented as CV is statistically more significant than when represented as mean fluorescence intensity (MFI)28, led to adjustments in the initially proposed protocol and, hence, reanalysis of the list mode data files by the individual centers. Gating strategies and analyzed parameters are shown in the Online Supplementary Information with FC plots of MDS in comparison to normal subjects.
Statistical analyses
Due to differences in sample processing, instrument settings, clones, and fluorochromes between centers, the expression levels of CD71, CD36, and CD105 varied. Therefore, the median expression levels of CD36, CD71, and CD105 in the subset of normal bone marrow samples were calculated for each individual center. Expression levels were then normalized against the median value for that particular marker for each center separately. Patient and control groups were compared using the Kruskal Wallis test for continuous data, and the Chi-square or the Fisher’s exact test for dichotomous data. Correlations between certain markers, and between markers and age, were analyzed using Spearman’s rank correlation coefficients. Comparing single parameters between MDS and control groups demonstrated that results overlapped (results section figure 2); hence, receiver-operator-curve (ROC) analyses did not yield applicable cut-offs. Therefore, cut-off values for aberrancies were based on the 10th and/or 90th percentile of the data of pathological controls in the learning cohort. Multivariate logistic regression analyses were performed to determine the erythroid markers that discriminate between pathological controls and MDS; data were analyzed dichotomously. All variables that displayed a univariate difference of P<0.1 were included in a backward selection procedure based on the Likelihood Ratio score. Regression coefficients of the variables in the final model were used to define the weight of these markers in a descriptive score for dyserythropoiesis. Cut-off level of the score indicating MDS-associated erythroid aberrancies was determined based on the total weight of these variables and a specificity of at least 90%. The sensitivity and specificity of the marker combination were calculated to illustrate predictive accuracy. The data were analyzed using SPSS 20.0 (IBM Corp, Armonk, NY), and GraphPad 6.0 software (La Jolla, CA). P-values <0.05 were considered significant.
Results
Flow cytometric analysis of the erythroid lineage in normal bone marrow samples: comparison of results from participating centers
Discrepancies in erythroid analysis between centers (and samples) can occur at several levels: a) sample quality (e.g., hemodilution); b) sample preparation (e.g., lysing procedure); c) data acquisition (e.g., acquisition rate and threshold of forward light scatter); and d) degree of adherence to the proposed gating strategy. Therefore, we first compared the FC results for normal bone marrow samples (learning cohort) between centers in terms of each defined marker. The percentage of NEC was highly diverse among centers; yet, it seemed to be independent of the lysing method applied (Online Supplementary Figure S1). Similarly, the percentage of CD71dim cells differed largely between centers. Furthermore, two centers reported higher percentages of CD117+ erythroid progenitors (up to 50% within the NEC) than the other centers (<15%). Results for one center could be explained by their stringent lysing procedures (i.e., 15 minutes at 37°C) which removed more mature (orthochromatic and polychromatic) erythroblasts resulting in a relative increase in early progenitors (data not shown). To circumvent the issues regarding differences in percentages of erythroid (sub)populations between centers, the percentages of NEC, CD117+ and CD105+ erythroid progenitors were also normalized as described for antigen expression levels (see Material and Methods statistics section); these are further referred to as relative percentages, i.e., relative to the median percentage in normal bone marrow samples (Online Supplementary Figure S2). CD71dim cells were rarely seen in normal controls; therefore, results for the percentage CD71dim could not be normalized.
Erythroid aberrancies that may discriminate between MDS and pathological controls
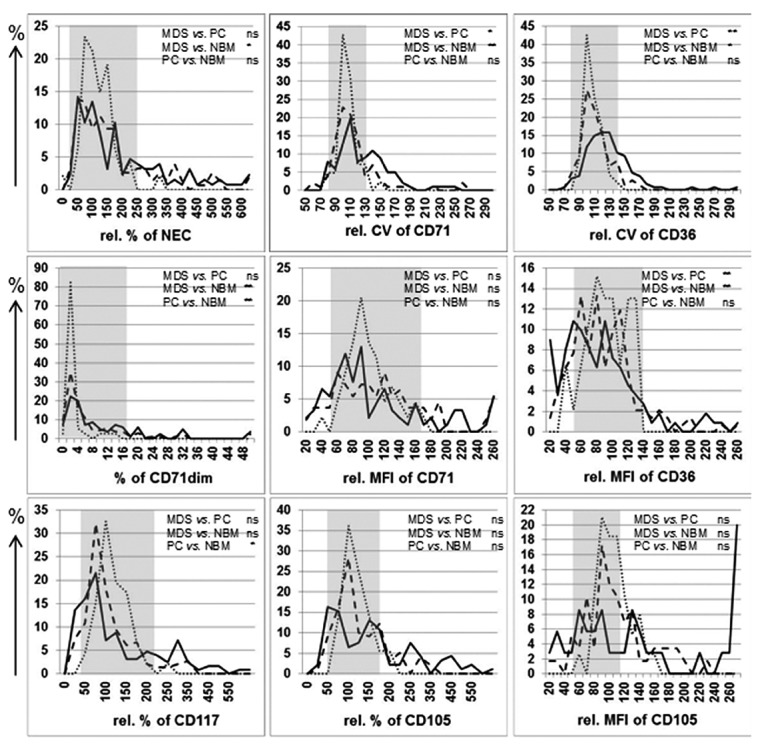
Next, all FC-erythroid parameters in the learning cohort were compared between MDS and controls. The results from the learning cohort are summarized in Figure 2 (P-values in Online Supplementary Table S1). The relative percentage of NEC within the total nucleated cell population was significantly higher in MDS than in the pathological and normal controls (P<0.001). Similarly, the CD71-CD235a differentiation pattern was more frequently considered aberrant in MDS (65%, 109/167 cases) than in pathological and normal controls (18% (44/254) and 3.7% (5/134) of cases, respectively (P<0.001)). To objectify the evaluation of this pattern, we analyzed its components separately. CD71 expression was analyzed in terms of MFI, CV, and the presence of a subpopulation with reduced CD71 expression (CD71dim). The relative CD71 MFI was significantly reduced in MDS, whereas the relative CV for CD71 and the percentage of CD71dim cells were significantly higher than those in both control groups (P<0.001); no significant differences were observed between the pathological controls and normal bone marrow samples. The expression of CD235a largely depends on the success of removing mature erythrocytes from a sample. Moreover, membrane fragments of lysed erythrocytes may stick to other cells in the analysis sample, mimicking positivity. Hence, this parameter was considered too unreliable for evaluation when considered individually.
Figure 2.
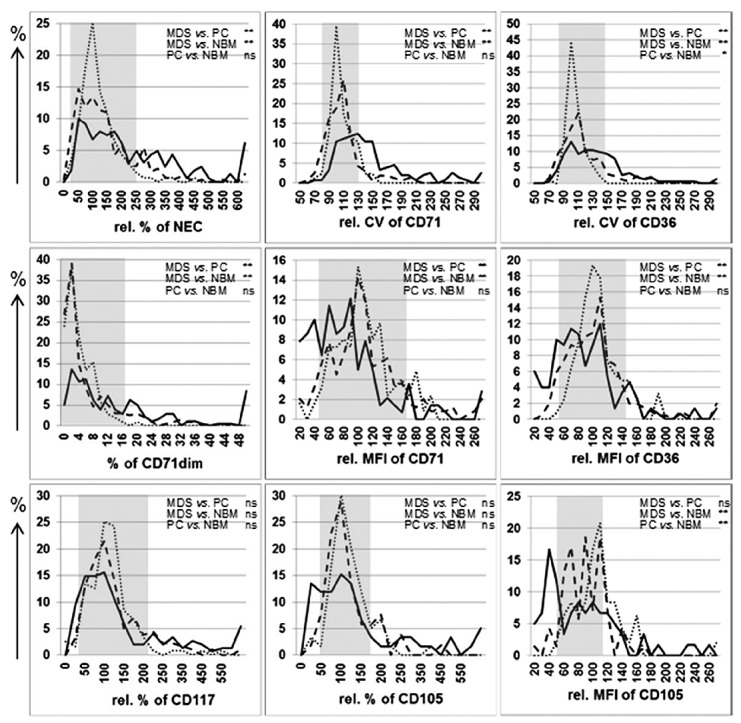
Distribution of erythroid markers analyzed by flow cytometry among MDS patients and controls within the learning cohort. Results of the analysis of indicated markers of the erythroid lineage are plotted along the X-axes: relative (rel.) percentages of nucleated erythroid cells (NEC); rel. mean fluorescence intensity (MFI) for CD36, CD71, and CD105; rel. coefficient of variation (CV) of CD36 and CD71; and rel. percentages of CD117+ and CD105+ erythroid progenitors. Relative frequencies (as percentage of the MDS or control cohort for a particular marker) are depicted along the Y-axes. Dotted lines represent results for normal bone marrow (NBM) samples, dashed lines pathological controls (PC) and solid lines MDS cases. P-values of comparison between groups are depicted: **: <0.001, *: <0.05, ns: not significant (Kruskal Wallis test). Grey boxes indicate reference ranges for the analyzed markers as defined by 10th and 90th percentiles of pathological controls. Scatterplots of results for the markers (depicted here as frequency histograms) that were selected as FC-markers for erythroid dysplasia from the multivariate analysis are depicted in Online Supplementary Figure S3.
The percentage of immature erythroid progenitors can also affect the appearance of the differentiation pattern. Analysis of the relative percentage of CD117+ (and CD105+) erythroid progenitor cells revealed a broader range of these cells in MDS, although not significantly different from the control groups.
Relative expression of CD105 was either increased or decreased in MDS. Nonetheless, CD105 expression did not discriminate between MDS and pathological controls.
Similar to that for CD71, the relative MFI of CD36 was significantly lower and the relative CV for CD36 was significantly higher in MDS than in the control groups.
To summarize, the markers that showed a significantly different distribution in MDS as compared to controls were: the relative percentage of NEC and the percentage of CD71dim cells (increased in MDS); the relative MFI of CD71 and CD36 (decreased in MDS); and the relative CV for CD71 and CD36 (increased in MDS); Figure 2.
Selection of a combination of erythroid FC aberrancies that distinguish MDS from pathological controls
To be applicable in FC analysis of a single patient in daily practice, cut-offs for the identification of MDS-associated changes of all potential aberrancies were defined (10th and 90th percentiles of the pathological controls, Online Supplementary Table S2A) and compared between MDS and controls (Table 3). All parameters differed between groups at a P-value of <0.1, and thus could have been considered for the multivariate logistic regression analysis. However, due to large differences between centers, regarding the percentages of NEC and CD71dim cells (likely due to technical variation as shown for normal controls), these parameters were not entered in the multivariate analysis. Besides, irrespective of the finding that data for CD105 significantly discriminated between subgroups (Table 3), this marker was not included. Entering CD105 data would have reduced the power of the (multicenter) analysis, since data on CD105 were only available in a limited number of centers (5/18) and cases. Multivariate logistic regression analysis was based on 119 MDS cases and 153 pathological controls that had available data for all parameters entered in the test. CD36 CV was identified as the best discriminator between MDS and pathological controls in combination with the CV of CD71, the MFI of CD71 and the percentage of CD117+ erythroid cells (Table 4). These four markers were used to define a FC-erythroid dysplasia score in which aberrancies were considered in a weighted manner: four points for increase in CD36 CV; three points for increase in CD71 CV; two points for decreased CD71 MFI; and two points in the case of decreased or increased percentage of CD117+ erythroid cells (reference ranges are summarized in Table 5). A cutoff of ≥5 points resulted in the identification of MDS-associated erythroid aberrancies by FC at a specificity of 90% (95% CI: 84–94%) and a sensitivity of 33% (95% CI: 24–42). Results for the selected markers and the application of the FC-erythroid dysplasia score in the learning cohort are displayed in Table 6 and Figure 3A. In daily practice, a numerical way of counting aberrancies would be more convenient. This involves the definition of a new cut-off; i.e., ≥2 aberrant markers (Figure 3C). Note that, the exception to this numerical score is that the combination of aberrancies in CD71 MFI and percentage of CD117+ alone is not sufficient to conclude dyserythropoiesis by FC (<5 points in the weighted score). The latter was seen in only one pathological control and three MDS cases.
Table 3.
Aberrancies in FC markers of the erythroid lineage between MDS and controls within the learning cohort.
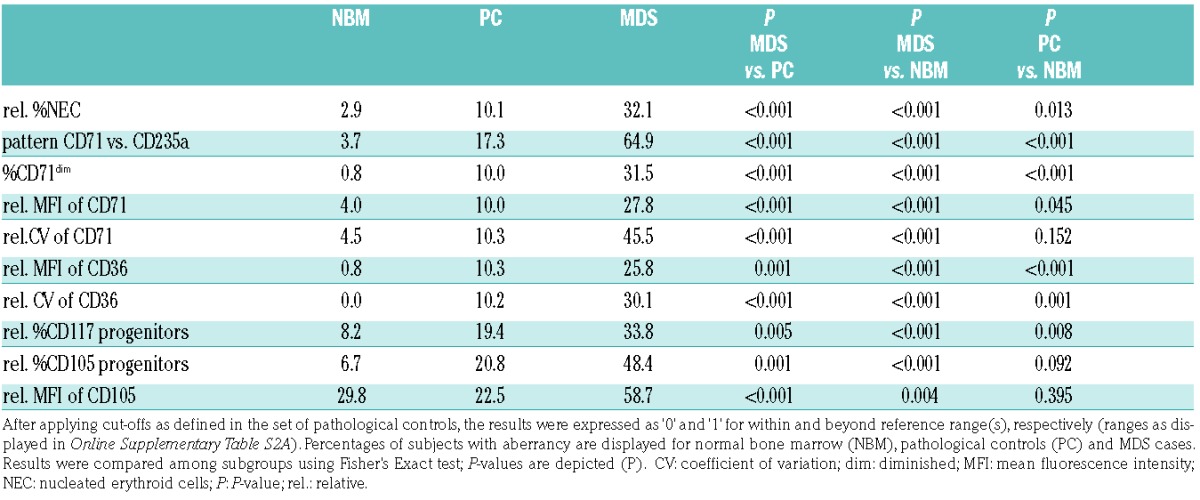
Table 4.
Results of multivariate logistic regression analysis in learning cohort.

Table 5.
Reference ranges of FC parameters incorporated in the FC-erythroid dysplasia score (learning cohort).
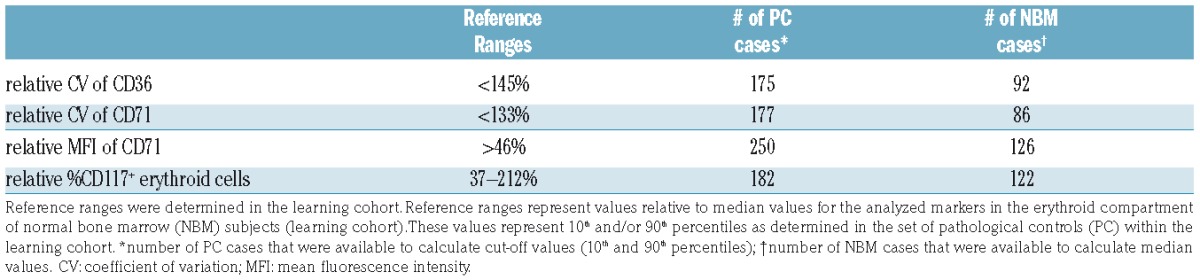
Table 6.
Results of FC aberrancies in the erythroid lineage and the FC-erythroid dysplasia score among MDS cases and controls within the learning cohort.
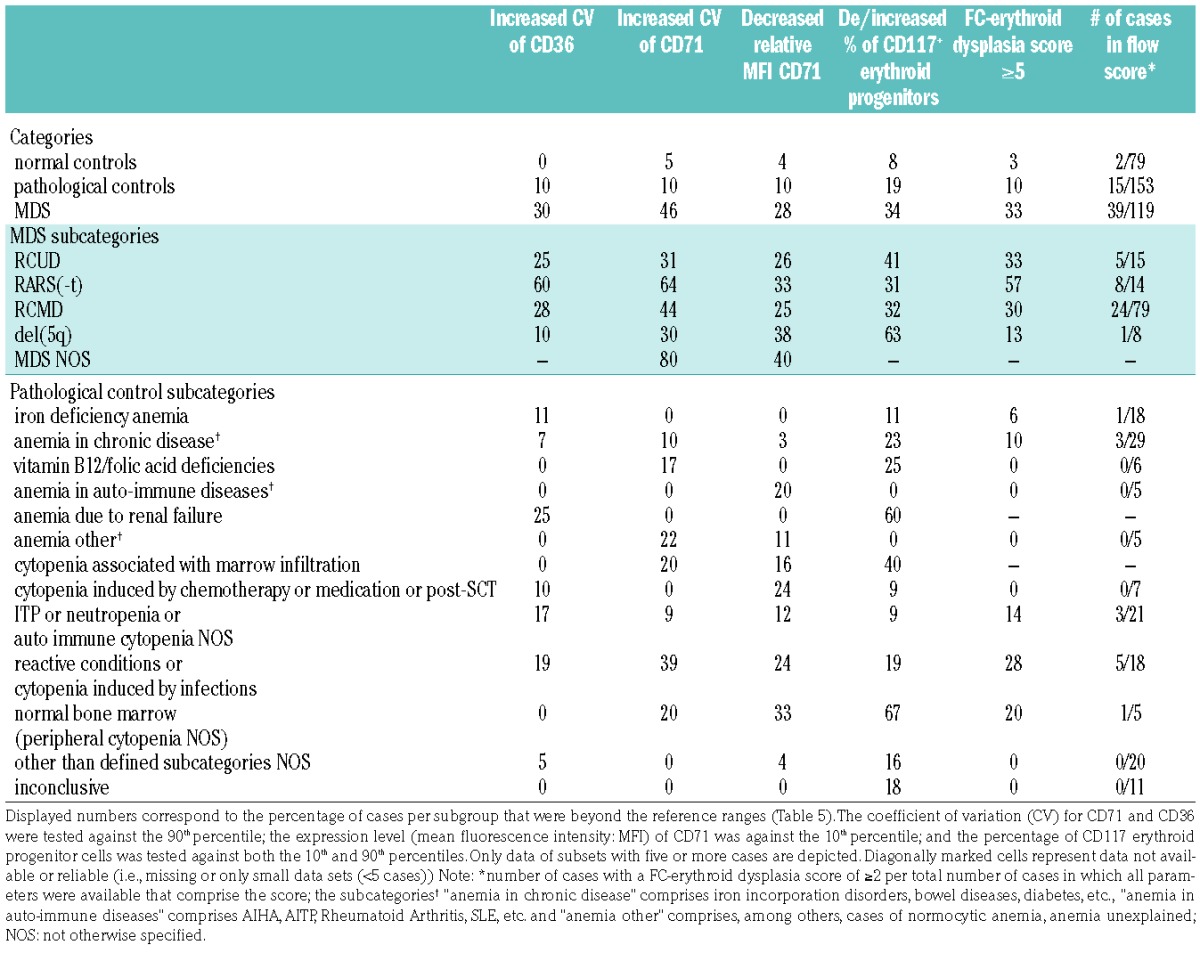
Figure 3.
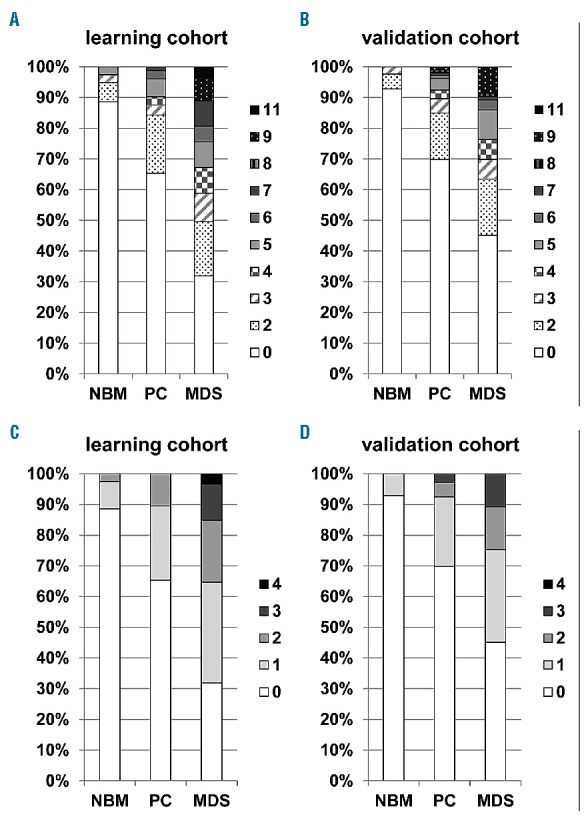
FC-erythroid dysplasia score in learning and validation cohorts. The weighted score consists of four parameters: increase in CD36 CV (4 points) and CD71 CV (3 points); decrease in CD71 MFI (2 points); and decrease or increase of CD117+ erythroid progenitors (2 points). A maximum score of 11 points can be reached. Data are grouped as normal bone marrow (NBM), pathological controls (PC) and MDS, relative distribution of the results for the score is displayed along the Y-axes. Panel A. represents the learning cohort consisting of 79 normal bone marrow samples (NBM), 153 pathological controls (PC) and 119 MDS cases. The FC-erythroid dysplasia score could only be calculated in the cases with data on all four defined parameters (351/670 cases). Panel B. represents the results in the validation cohort consisting of 42 NBM samples, 106 pathological controls and 93 MDS cases (241/320 cases). Clonal disorders as aplastic anemia and those within the category of essential thrombocythemia, polycythemia vera and primary myelofibrosis were excluded from both cohorts (two and nine cases for learning and validation cohorts, respectively). A cut-off of ≥5 points resulted in a specificity of 90% (95% CI: 84–94%) and a sensitivity of 33% (95% CI: 24–42) in the learning cohort; in the validation cohort, specificity was 92% (95% CI: 86–97%) and sensitivity 24% (95% CI: 15–34%). The numerical score, depicted in panels C and D, consists of four parameters: increase in CD36 CV and CD71 CV; decrease in CD71 MFI; and decrease or increase of CD117+ erythroid progenitors. A maximum score of 4 points can be reached. A cut-off of ≥2 points resulted in a specificity of 90% (95% CI: 84–94%) and a sensitivity of 35% (95% CI: 27–45) in the learning cohort; in the validation cohort, specificity and sensitivity were 92% (95% CI: 86–97%) and 25% (95% CI: 16–35%), respectively.
Correlation between erythroid markers and age
The incidence of MDS increases with age; hence, erythroid markers that are significantly correlated with age may be less suitable for discriminating between MDS and controls. Since we observed significant differences between the groups regarding age (Table 1); correlations between FC results for erythroid markers and age were evaluated for normal bone marrow samples. Only CD105 MFI, a variable that was not included in the multivariate analysis, demonstrated a moderate-to-good inverse correlation with age, i.e., CD105 expression decreased with increasing age (Spearman’s Rho −0.55, P<0.001, n=47, Online Supplementary Table S4 and Online Supplementary Figure S4).
Validation of FC aberrancies in the erythroid lineage in MDS and pathological controls
The value of the defined antigenic combinations was tested in an independent cohort. Nine centers provided data for this validation cohort, the results are depicted in Figure 4 and Online Supplementary Table S1. Similar to results in the learning cohort, the relative CVs of CD36 and CD71 were significantly increased in MDS as compared to controls, whereas CD36 MFI was significantly decreased. Since the distribution of subcategories was similar in the MDS learning and validation cohorts, we compared FC results between the two MDS cohorts. This revealed that the increase in CD71 CV and the decrease in CD71 MFI were significantly less evident in the MDS validation cohort than in the learning cohort (t-test, P<0.001). Results for CD36 CV and the percentage of CD117+ erythroid cells did not differ between both MDS cohorts (P=0.134 and 0.116, respectively).
Figure 4.
Distribution of erythroid markers analyzed by FC within subgroups of MDS patients and controls within the validation cohort. Results of the analysis of selected markers of the erythroid lineage in the validation cohort are plotted along the X-axes: relative coefficient of variation (CV) of CD36 and CD71, and relative percentages of CD117+ erythroid progenitors. Normalization was performed against results for the normal bone marrow (NBM) samples of the validation cohort per each individual center. Relative frequencies are depicted along the Y-axes. Dotted lines represent results for NBM samples, dashed lines pathological controls (PC), and solid lines MDS cases. Grey boxes indicate 10th and/or 90th percentiles of pathological controls defined in the learning cohort that were applied for evaluating aberrancies.
Reference ranges, as defined in the learning cohort, were applied to evaluate the data from the validation cohort, and then to calculate the weighted FC-erythroid dysplasia score. This resulted in a specificity of 92% (95% CI: 86–97%) and a sensitivity of 24% (95% CI: 15–34%) for identifying MDS-associated erythroid aberrancies by FC (Figure 3B and Online Supplementary Table S5). In most cases, the numerical score could have been applied (cut-off ≥2 aberrancies; Figure 3D) with the same result regarding presence of erythroid dysplasia; only one MDS had decreased CD71 MFI in combination with an altered CD117+ percentage.
Discussion
Analysis of erythroid dysplasia is rarely included in current FC protocols for MDS, since the significance of FC data from the erythroid lineage is, to a large extent, still under debate.4 Here, we reported the results of a multicenter study within the IMDSFlow group, which focused on defining erythroid parameters that enable discrimination of dyserythropoiesis associated with MDS from non-clonal cytopenia. The majority of erythroid FC markers that are recommended for evaluation of dysplasia according to ELNet guidelines4 were significantly different between MDS and controls. Analysis of the presence of aberrancies in the erythroid markers CD71 and CD36 (expressed as the CV), together with the MFI of CD71 and an abnormal percentage of CD117+ erythroid progenitor cells, provided the best discrimination between MDS and non-clonal cytopenia. A weighted score based on these four parameters yielded a specificity of 90% (95% CI: 84–94%) in the learning cohort and 92% (95% CI: 86–97%) in the validation cohort. Sensitivity of the weighted score was 33% (95% CI: 24–42%) and 24% (95% CI: 15–34%) in the learning and validation cohorts, respectively. The latter lower sensitivity could be explained by a less evidently increased CD71 CV and decreased CD71 MFI in the MDS validation cohort compared to the learning cohort. Hence, fewer MDS cases scored CD71 CV and/or CD71 MFI as aberrant (Online Supplementary Table S3). Notably, these scores only reflect the presence of FC-erythroid dysplasia, not the likelihood of an MDS diagnosis.
Tenth and 90th percentiles in the validation cohort’s control cases slightly differed from the learning cohort (Online Supplementary Table S2B). Yet, application of these cut-offs in the validation cohort resulted in comparable specificity: 91% (95% CI: 84–96%; sensitivity: 27% (95% CI: 18–37%). In general, cut-off values are most reliable when defined by standardized analyses of control samples in a single center. Notably, no consensus has been reached as to whether percentiles, standard deviations or log differences should be applied as cut-offs for any of the MDS-associated aberrancies.
Specificity of the defined markers for identification of MDS-associated erythroid changes is considered to be more important than their general diagnostic value for MDS. The specificity may be optimized by increasing the cut-off from ≥5 to ≥6 points (specificity 96% in both cohorts), at the cost, however, of a decrease in sensitivity (24% and 14%, in the learning and validation cohorts, respectively).
To simplify interpretation of results from erythroid analysis, a numerical way of counting aberrancies was tested; a cut-off of ≥2 aberrant markers led to comparable specificity and sensitivity as for the weighted score. However, it must be taken into account that the sole combination of CD71 MFI and percentage of CD117+ erythroid progenitors is not sufficient to indicate MDS-associated changes in the erythroid lineage. Cremers et al. compared the analysis of the set of four FC-parameters to erythroid dysplasia as assessed by cytomorphology.29 They demonstrated that FC correlated well with cytomorphology, albeit at a lower sensitivity (low/int-1 risk MDS, 64% vs. 84%, respectively); controls showed 11% and 10% of dysplasia by FC and cytomorphology, respectively. The findings presented herein confirmed results from a recent study28 that reported a significant increase in CD71 CV and CD36 CV to be highly suggestive for MDS. Yet, discrimination between MDS and controls based on CV values was less clear in the current dataset. Mathis et al.28 stated that the difference in CD71 CV between MDS and controls was less pronounced after erythrocyte lysis; however, this was not the case for CD36 CV. Since all data in the present study were obtained after erythrocyte lysis, it might explain the observed differences. It may seem paradoxical to use erythrocyte lysing procedures when the focus is on analysis of the erythroid lineage; but lyse-stain-wash is the recommended protocol for processing samples for FC in MDS.3 Despite IMDSFlow recommendations, methodological variation between centers may have led to differences in results as demonstrated in normal controls. Harmonization, or even standardization, of methods may narrow differences and improve validity of conclusions from multicenter studies, as has been demonstrated within the Euroflow consortium.30 Hence, grouping of data per technical procedure could have been informative from a practical perspective; yet, the power of the analyses within and between numerous subgroups of centers would have been strongly limited by sample sizes. Notably, in daily practice, FC results in subjects suspected of MDS should preferably be compared with a center’s own cohort of control samples. Despite these technical considerations, our data confirm the robustness of the evaluation of an increase in CD71 and CD36 CV on erythroid cells.28
Another discriminatory marker was the percentage of erythroid progenitors defined as CD117+. A potential marker for future inclusion in erythroid data analysis by FC is CD105. It has been demonstrated (in normal and pathological controls) that CD105 is lost before carbonic anhydrase is expressed, which suggests that the majority of CD105+ erythroid progenitor cells are not subject to ammonium chloride-based lysing protocols.16 This confirms the robustness of the percentage of erythroid progenitors (CD117+ and/or CD105+) as a marker for erythroid dysplasia. Notably, hemodilution impacts the analysis of the erythroid compartment as it may result in a lack or paucity of erythroid progenitors, similar to what is seen in the myelomonocytic compartments. In heavily hemodiluted samples, the erythroid lineage should be considered non-evaluable.
Application of CD105 may overcome the potential error of assigning CD117+ myeloid progenitors as erythroid progenitors, especially when combined with CD117 and an additional myeloid marker such as CD33. Furthermore, CD105 overexpression was confirmed in some cases of MDS in our dataset.18,20 However, we also observed a decreased expression in MDS. Notably, CD105 expression was negatively correlated with age in normal controls. Future studies in larger data sets may elucidate whether CD105 is truly valuable in analysis of erythroid dysplasia in MDS.
New insights may improve the impact of FC in the diagnosis of MDS. A recent report showed that increased expression of CD44 on all maturational stages of erythroid cells was associated with MDS, irrespective of presence or absence of morphologic dyserythropoiesis.31 In addition, decreased expression of the major coxsackie-adenovirus receptor (CAR) was demonstrated in dysplastic CD105+ erythroid progenitors.32,33 The diagnostic value of the herein presented parameter combination is limited. Yet, ultimately, the analysis of the erythroid and myelomonocytic lineages and hematogones should be combined. Further validation should reveal the power of the herein defined erythroid markers. Results from a prospective clinical trial in low/int-1 risk MDS demonstrated that the addition of proposed erythroid FC-markers to the more widely acknowledged analysis of the myelomonocytic lineage increased the sensitivity of MDS-FC from 68 to 80% (specificity only slightly decreased from 98% to 95%).29 In addition, it would be relevant to elucidate the value of the combination of myeloid and erythroid FC markers in indeterminate cases according to cytomorphology. MDS-FC of the myelomonocytic lineage has shown to be of negative predictive value in these cases.34,35
In view of emerging knowledge from next generation sequencing analysis, future research may also concern the analysis of the relation between gene modifications/mutations and FC findings. Data comparing cytogenetic aberrations and FC have already demonstrated distinct profiles.36,37 Parallel mutational data in the current cohort are not available, but it would be of interest to compare, for instance, the immunophenotypic profile of nucleated erythroid cells in relation to the presence of a SF3B1 mutation since there is a relation between this mutation and the occurrence of ring sideroblasts.38
Cytomorphology reports dysplastic features in erythropoiesis in non-MDS cases, such as reactive conditions.23–25 Moreover, patients with cytopenia due to marrow infiltration may demonstrate FC aberrancies associated with MDS. MDS may even coincide with the other malignancy in these patients.39,40 A subset of patients with reactive marrows or marrow infiltration in our dataset indeed showed multiple erythroid aberrancies (5/23 and 2/9, respectively; Online Supplementary Table S5). Follow-up analysis after several months may exclude or confirm MDS in these cases.34,35 This stresses that FC analysis in suspected MDS, though proven very specific, should always be part of an integrated diagnostic approach rather than a solitary diagnostic tool.41 In line with this, FC may attribute to the diagnostic work-up in cases that show clonal hematopoiesis of indeterminate potential (CHIP), particularly when patients present with cytopenia and have indeterminate cytomorphology and/or non-informative cytogenetics.
To summarize, we identified significant aberrancies with respect to the FC markers recommended by IMDSFlow for analysis of the erythroid lineage in MDS. The best indicators of dysplastic changes associated with MDS were an increased CV of CD36 and CD71, a decreased MFI of CD71 in combination with decreased or increased percentages of erythroid progenitors (CD117+). Application of the defined marker set demonstrated high specificity. Future studies should assess the contribution of the selected erythroid markers to the evaluation of the myeloid progenitors, the maturing myelomonocytic lineage, and hematogones in current FC protocols in MDS. This will be implemented in an upcoming multicenter data collection exercise within IMDSFlow.
Supplementary Material
Acknowledgments
The authors would like to thank Claudia Cali and Kelly Schouten (VU University Medical Center Amsterdam, The Netherlands), Jeroen Lauf (Elisabethinen Hospital, Linz, Austria), Frauke Bellos (MLL Munich Leukemia Laboratory, Munich, Germany), Hans Veenstra (Radboud University Medical Center, Nijmegen, The Netherlands), Rik Brooimans and Andre Bijkerk (Erasmus Medical Center, Rotterdam, The Netherlands) for their contribution to data collection, although they did not take part in the IMDSFlow working group conferences. Contributors from The Netherlands are all members of the “Flow Cytometry in MDS” working group within the Dutch Society of Cytometry.
Footnotes
Check the online version for the most updated information on this article, online supplements, and information on authorship & disclosures: www.haematologica.org/content/102/2/308
References
- 1.Brunning R, Orazi A, Germing U, et al. Myelodysplastic syndromes/neoplasms. In: Swerdlow, et al., ed. WHO classification of Tumours and Haematopoietic and Lymphoid Tissues. Lyon: IARC; 2008 [Google Scholar]
- 2.Malcovati L, Hellstrom-Lindberg E, Bowen D, et al. Diagnosis and treatment of primary myelodysplastic syndromes in adults: recommendations from the European LeukemiaNet. Blood. 2013;122(17):2943–2964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.van de Loosdrecht AA, Alhan C, Bene MC, et al. Standardization of flow cytometry in myelodysplastic syndromes: report from the first European LeukemiaNet working conference on flow cytometry in myelodysplastic syndromes. Haematologica. 2009;94(8):1124–1134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Westers TM, Ireland R, Kern W, et al. Standardization of flow cytometry in myelodysplastic syndromes: a report from an international consortium and the European LeukemiaNet Working Group. Leukemia. 2012;26(7):1730–1741. [DOI] [PubMed] [Google Scholar]
- 5.Wells DA, Benesch M, Loken MR, et al. Myeloid and monocytic dyspoiesis as determined by flow cytometric scoring in myelodysplastic syndrome correlates with the IPSS and with outcome after hematopoietic stem cell transplantation. Blood. 2003;102(1):394–403. [DOI] [PubMed] [Google Scholar]
- 6.van de Loosdrecht AA, Westers TM, Westra AH, et al. Identification of distinct prognostic subgroups in low- and intermediate-1-risk myelodysplastic syndromes by flow cytometry. Blood. 2008; 111(3):1067–1077. [DOI] [PubMed] [Google Scholar]
- 7.Chu SC, Wang TF, Li CC, et al. Flow cytometric scoring system as a diagnostic and prognostic tool in myelodysplastic syndromes. Leuk Res. 2011;35(7):868–873. [DOI] [PubMed] [Google Scholar]
- 8.Kern W, Haferlach C, Schnittger S, Haferlach T. Clinical utility of multiparameter flow cytometry in the diagnosis of 1013 patients with suspected myelodysplastic syndrome: correlation to cytomorphology, cytogenetics, and clinical data. Cancer. 2010;116(19):4549–4563. [DOI] [PubMed] [Google Scholar]
- 9.Maassen A, Strupp C, Giagounidis A, et al. Validation and proposals for a refinement of the WHO 2008 classification of myelodysplastic syndromes without excess of blasts. Leuk Res. 2013;37(1):64–70. [DOI] [PubMed] [Google Scholar]
- 10.Germing U, Strupp C, Giagounidis A, et al. Evaluation of dysplasia through detailed cytomorphology in 3156 patients from the Dusseldorf Registry on myelodysplastic syndromes. Leuk Res. 2012;36(6):727–734. [DOI] [PubMed] [Google Scholar]
- 11.Stetler-Stevenson M, Arthur DC, Jabbour N, et al. Diagnostic utility of flow cytometric immunophenotyping in myelodysplastic syndrome. Blood. 2001;98(4):979–987. [DOI] [PubMed] [Google Scholar]
- 12.Malcovati L, Della Porta MG, Lunghi M, et al. Flow cytometry evaluation of erythroid and myeloid dysplasia in patients with myelodysplastic syndrome. Leukemia. 2005;19(5):776–783. [DOI] [PubMed] [Google Scholar]
- 13.Matarraz S, Lopez A, Barrena S, et al. Bone marrow cells from myelodysplastic syndromes show altered immunophenotypic profiles that may contribute to the diagnosis and prognostic stratification of the disease: a pilot study on A series of 56 patients. Cytometry B Clin Cytom. 2010; 78(3):154–168. [DOI] [PubMed] [Google Scholar]
- 14.Machherndl-Spandl S, Suessner S, Danzer M, et al. Molecular pathways of early CD105-positive erythroid cells as compared with CD34-positive common precursor cells by flow cytometric cell-sorting and gene expression profiling. Blood Cancer J. 2013;3:e100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fajtova M, Kovarikova A, Svec P, Kankuri E, Sedlak J. Immunophenotypic profile of nucleated erythroid progenitors during maturation in regenerating bone marrow. Leuk Lymphoma. 2013;54(11):2523–2530. [DOI] [PubMed] [Google Scholar]
- 16.Wangen JR, Eidenschink Brodersen L, Stolk TT, Wells DA, Loken MR. Assessment of normal erythropoiesis by flow cytometry: important considerations for specimen preparation. Int J Lab Hematol. 2014; 36(2):184–196. [DOI] [PubMed] [Google Scholar]
- 17.McGrath KE, Bushnell TP, Palis J. Multispectral imaging of hematopoietic cells: where flow meets morphology. J Immunol Methods. 2008;336(2):91–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Della Porta MG, Malcovati L, Invernizzi R, et al. Flow cytometry evaluation of erythroid dysplasia in patients with myelodysplastic syndrome. Leukemia. 2006; 20(4):549–555. [DOI] [PubMed] [Google Scholar]
- 19.Lorand-Metze I, Ribeiro E, Lima CS, Batista LS, Metze K. Detection of hematopoietic maturation abnormalities by flow cytometry in myelodysplastic syndromes and its utility for the differential diagnosis with non-clonal disorders. Leuk Res. 2007; 31(2):147–155. [DOI] [PubMed] [Google Scholar]
- 20.Xu F, Wu L, He Q, et al. Immunophenotypic analysis of erythroid dysplasia and its diagnostic application in myelodysplastic syndromes. Intern Med J. 2012;42(4):401–411. [DOI] [PubMed] [Google Scholar]
- 21.Hu J, Liu J, Xue F, et al. Isolation and functional characterization of human erythroblasts at distinct stages: implications for understanding of normal and disordered erythropoiesis in vivo. Blood. 2013; 121(16):3246–3253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Eidenschink Brodersen L, Menssen AJ, Wangen JR, et al. Assessment of Erythroid Dysplasia by “Difference from Normal” in Routine Clinical Flow Cytometry Work-up. Cytometry B Clin Cytom. 2015;88(2):125–135. [DOI] [PubMed] [Google Scholar]
- 23.Bain BJ. The bone marrow aspirate of healthy subjects. Br J Haematol. 1996; 94(1):206–209. [DOI] [PubMed] [Google Scholar]
- 24.Parmentier S, Schetelig J, Lorenz K, et al. Assessment of dysplastic hematopoiesis: lessons from healthy bone marrow donors. Haematologica. 2012;97(5):723–730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Della Porta MG, Travaglino E, Boveri E, et al. Minimal morphological criteria for defining bone marrow dysplasia: a basis for clinical implementation of WHO classification of myelodysplastic syndromes. Leukemia. 2015;29(1):66–75. [DOI] [PubMed] [Google Scholar]
- 26.Westers TM, van der Velden VHJ, Alhan C, et al. Implementation of flow cytometry in the diagnostic work-up of myelodysplastic syndromes in a multicenter approach: report from the Dutch Working Party on Flow Cytometry in MDS. Leuk Res. 2012; 36(4):422–430. [DOI] [PubMed] [Google Scholar]
- 27.van Dongen JJ, Lhermitte L, Bottcher S, et al. EuroFlow antibody panels for standardized n-dimensional flow cytometric immunophenotyping of normal, reactive and malignant leukocytes. Leukemia. 2012;26(9):1908–1975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mathis S, Chapuis N, Debord C, et al. Flow cytometric detection of dyserythropoiesis: a sensitive and powerful diagnostic tool for myelodysplastic syndromes. Leukemia. 2013;27(10):1981–1987. [DOI] [PubMed] [Google Scholar]
- 29.Cremers EMP, Westers TM, Alhan C, et al. Implementation of erythroid analysis by flow cytometry in diagnostic models for myelodysplastic syndromes. Haematologica. 2016;102(2):320–326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kalina T, Flores-Montero J, Lecrevisse Q, et al. Quality assessment program for EuroFlow protocols: Summary results of four-year (2010–2013) quality assurance rounds. Cytometry A. 2015;87(2):145–156. [DOI] [PubMed] [Google Scholar]
- 31.Laranjeira P, Rodrigues R, Carvalheiro T, et al. Expression of CD44 and CD35 during normal and myelodysplastic erythropoiesis. Leuk Res. 2014;39(3):361–370. [DOI] [PubMed] [Google Scholar]
- 32.Macchherndl-Spandl S, Suessner S, Danzer M, et al. Abnormal Expression of the Major Coxsackie-Adenovirus Receptor CAR on Immature Dysplastic CD105+ Erythroid Progenitor Cells in Patients with MDS and Related Bone Marrow Neoplasms. Blood. 2013;122(21):2818. [Google Scholar]
- 33.Bauer K, Machherndl-Spandl S, Suessner S, et al. Identification of CAR as Novel Mediator of Erythroid Differentiation and Migration That is Specifically Downregulated in Erythroid Progenitor Cells in Patients with MDS. Blood. 2014; 124(21):1570.25006130 [Google Scholar]
- 34.Kern W, Haferlach C, Schnittger S, Alpermann T, Haferlach T. Serial assessment of suspected myelodysplastic syndromes: significance of flow cytometric findings validated by cytomorphology, cytogenetics, and molecular genetics. Haematologica. 2013(2);98:201–207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Cremers EMP, Westers TM, Alhan C, et al. Multiparameter flow cytometry is instrumental to distinguish myelodysplastic syndromes from non-neoplastic cytopenias. Eur J Cancer. 2016;54(2):49–56. [DOI] [PubMed] [Google Scholar]
- 36.Cutler JA, Wells DA, van de Loosdrecht AA, et al. Phenotypic abnormalities strongly reflect genotype in patients with unexplained cytopenias. Cytometry B Clin Cytom. 2011;80(3):150–157. [DOI] [PubMed] [Google Scholar]
- 37.Oelschlaegel U, Westers TM, Mohr B, et al. Myelodysplastic syndromes with a deletion 5q display a characteristic immunophenotypic profile suitable for diagnostics and response monitoring. Haematologica. 2015;100(3):e93–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Papaemmanuil E, Cazzola M, Boultwood J, et al. Somatic SF3B1 mutation in myelodysplasia with ring sideroblasts. N Engl J Med. 2011;365(15):1384–1395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Matarraz S, Paiva B, Díez-Campelo M, et al. Immunophenotypic alterations of bone marrow myeloid cell compartments in multiple myeloma patients predict for myelodysplasia-associated cytogenetic alterations. Leukemia. 2014;28(8):1747–1750. [DOI] [PubMed] [Google Scholar]
- 40.Rodriguez-Caballero A, Henriques A, Criado I, et al. Subjects with chronic lymphocytic leukaemia-like B-cell clones with stereotyped B-cell receptors frequently show MDS-associated phenotypes on myeloid cells. Br J Haematol. 2015; 168(2):258–267. [DOI] [PubMed] [Google Scholar]
- 41.Porwit A, van de Loosdrecht AA, Bettelheim P, et al. Revisiting guidelines for integration of flow cytometry results in the WHO classification of myelodysplastic syndromes-proposal from the International/European LeukemiaNet Working Group for Flow Cytometry in MDS. Leukemia. 2014;28(9):1793–1798. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.