

Abstract
Background
Tobacco smoking is the main cause of lung cancer, but it is not the sole causal factor. Significant proportions of workers are smokers and exposed to occupational lung carcinogens. This study aims to systematically review the statistical interaction between occupational lung carcinogens and tobacco smoking, in particular asbestos, crystalline silica and diesel engine exhaust emissions.
Methods
Articles were identified using Scopus, PubMed, and Web of Science, and were limited to those published in English or French, without limitation of time. The reference list of selected studies was reviewed to identify other relevant papers. One reviewer selected the articles based on the inclusion and exclusion criteria. Two reviewers checked the eligibility of articles to be included in the systematic review. Data were extracted by one reviewer and revised by two other reviewers. Cohorts and case–control studies were analyzed separately. The risk of bias was evaluated for each study based on the outcome. The results of the interaction between the tobacco smoking and each carcinogen was evaluated and reported separately.
Results
Fifteen original studies were included for asbestos-smoking interaction, seven for silica-smoking interaction and two for diesel-smoking interaction. The results suggested the absence of multiplicative interaction between the three occupational lung carcinogens and smoking. There is no enough evidence from the literature to conclude for the additive interaction. We believe there is a limited risk of publication bias as several studies reporting negative results were published.
Conclusion
There are no multiplicative interactions between tobacco smoking and occupational lung carcinogens, in particular asbestos, crystalline silica and diesel engine exhaust emissions. Even though, specific programs should be developed and promoted to reduce concomitantly the exposure to occupational lung carcinogens and tobacco smoking.
Electronic supplementary material
The online version of this article (doi:10.1186/s12889-017-4025-1) contains supplementary material, which is available to authorized users.
Keywords: Lung cancer, Interaction, Smoking, Occupational exposures
Background
Lung cancer remains the leading cause of cancer deaths among males and females [1, 2]. In 1986, the International Agency for Research on Cancer (IARC) classified tobacco smoking as a lung carcinogen [3], it was identified as the main cause of lung cancer, and it was found to account for 80–90% of the cases [4, 5]. However tobacco smoking is not the sole causal factor of lung cancer. Indeed, lung cancer cases have been identified in non-smokers groups but exposed to different types of occupational exposures [6]. In the last update of IARC, almost 29 agents were classified as lung carcinogens with sufficient evidence in humans [7]. Many of them are found in occupational settings such as all forms of asbestos, crystalline silica and diesel engine exhaust emissions, which are among the top most frequent occupational exposures [8–11].
The rate of smoking is higher among blue-collar workers than white-collar workers [12]. Thus a significant proportion of workers are concomitantly exposed to occupational lung carcinogens and to tobacco smoking. This brings into light the importance of studying the statistical interactions between the occupational exposures and tobacco smoking.
In fact, the statistical interaction between the occupational exposure to asbestos and tobacco smoking was well studied through systematic reviews and meta-analyses, indicating the presence of a positive additive statistical interaction [13–15]. In the other hand, no systematic reviews were conducted to evaluate the statistical interactions between occupational exposure to crystalline silica and tobacco smoking or between diesel engine exhaust emissions and tobacco smoking.
Determine the nature of the statistical interaction between the occupational exposures and tobacco smoking is of high interest from a public health perspective, in particular to develop prevention programs. Therefore, we conducted a review on the interaction between the three most important occupational lung carcinogens, namely asbestos, crystalline silica and diesel engine exhaust emissions and tobacco smoking to define if the interaction nature is similar irrespective to the lung carcinogen, or if the interaction nature is specific for each carcinogen.
The objective of this study is to evaluate the statistical interactions between the occupational exposures and tobacco smoking, with limitation to the three principal lung carcinogens; asbestos, crystalline silica and diesel engine exhaust emissions, through a systematic review including cohort and case–control studies.
Methods
This systematic review was reported based on the PRISMA checklist (2009) Additional file 1 and the PRISMA-P for developing review protocols (2015) [16, 17].
Search strategy
Articles reviewed in this paper were identified using three bibliographic databases: PubMed, Scopus and Web of Science. The selected studies were limited to those published in English or French, without limitation of time. The most recent research was conducted in June 30, 2016.
For asbestos-tobacco, silica-tobacco and diesel-tobacco statistical interactions, all records of the three bibliographic databases were searched using the following key words respectively: ["asbestos" and "lung cancer" and "smoking"], ["silica" and "lung cancer" and "smoking"], and ["diesel" and "lung cancer" and "smoking"].
Inclusion criteria
Studies were included in this review if they met the following criteria: human studies, studies published in peer-reviewed journals, cohort or case–control studies, studies evaluating the statistical interaction between tobacco smoking and one of the three studied occupational exposures on lung cancer, studies reporting the occupational exposure assessment, studies reporting the smoking behavior assessment, studies reporting the statistical analysis performed to assess the statistical interaction, and studies reporting the results of the statistical interaction and their statistical significance (P-value or CI 95%). For studies analyzing the same population, the most recently published article evaluating the statistical interaction that met all of the previous criteria was included.
Exclusion criteria
In general, studies not meeting the inclusion criteria were excluded: clinical trials, in vitro studies, animal studies, cross-sectional studies, systematic reviews, meta-analyses, case reports and case series. Articles studying the statistical interactions between environmental exposures to asbestos, crystalline silica and diesel engine exhaust emissions and tobacco smoking on lung cancer were also excluded. Finally, articles that investigated the statistical interactions between asbestosis, silicosis, and smoking without taking into consideration asbestos and crystalline silica exposures were also excluded.
Articles selection process
Records identified through the three bibliographic databases were checked for duplications. Duplicated records were removed, and the remaining records were screened to distinguish those that met the inclusion criterias. The screening phase was done in three steps: 1) selection of articles that studied the association between one of the three occupational exposures and lung cancer, 2) selection of the articles that studied the interaction based on the title or the abstract, and 3) for the remaining articles, the full-text was screened to select studies that evaluated the interaction between one of the three occupational exposures and smoking. The reference list of the selected articles was reviewed to identify other relevant articles. The full-text articles remained was assessed for eligibility to determine the final list of articles included in the qualitative synthesis.
Data extraction
Data extraction was performed by one author (MZ), and reviewed by two other authors (FD and AL). The following data were extracted from each study included in the present review: first author, publication year, geographic area, study type (prospective cohort study, retrospective cohort study, nested case–control study, population-based case–control study, hospital-based case–control study), exposure type, industry type, total number of subjects (population and cases/cases and controls), the method to collect the occupational exposure and smoking status details, the definition of occupational exposure, the definition of smoking status, the outcome (lung cancer) classification, the methodology of the statistical interaction evaluation, and the results of the statistical interaction evaluation.
Statistical interaction concepts
Rothman et al. stated that “the concept of interaction is that the effect of an exposure, compared with a reference unexposed group, may depend on the presence of one or more other factors”. In addition, they specified that the statistical interaction is potentially scale-dependent [18]. In epidemiologic studies, researchers examine the additive interaction or multiplicative interaction only for empirical reasons; and usually use the one that shows a better fit to the observations. In fact, statistical interactions are mostly evaluated on multiplicative scale, due to the statistical models used in the analyses (e.g. logistic regression), and that the models generate the multiplicative interaction result directly. If authors are interested in the evaluation of the statistical interaction, they should report results on additive and multiplicative scales [19]. The methods of the statistical interaction evaluation used in the original papers are described in more detail [see Additional file 2].
Quality assessment and risk of bias
The Newcastle-Ottawa quality assessment scale (NOS) was used to assess the quality of the design and the conduction of the included studies at the outcome level [20, 21].
Results
Study selection
Using the methodology previously delineated, 2,302 articles were identified for the asbestos-smoking interaction: 1,061 from Scopus, 628 from PubMed, and 613 from Web of Science. In addition, two articles were added from the reference list of the selected articles. 1,028 articles were duplicated and excluded. From the remaining 1,276 articles, 1,250 papers were irrelevant; studies not meeting the inclusion criteria, or meeting the exclusion criteria. After screening phase, 26 full-text articles were assessed for eligibility; 11 articles were excluded because of duplicates population and 15 articles were retained including 6 cohorts, 1 case-cohort study, and 8 case–control studies (Fig. 1).
Fig. 1.
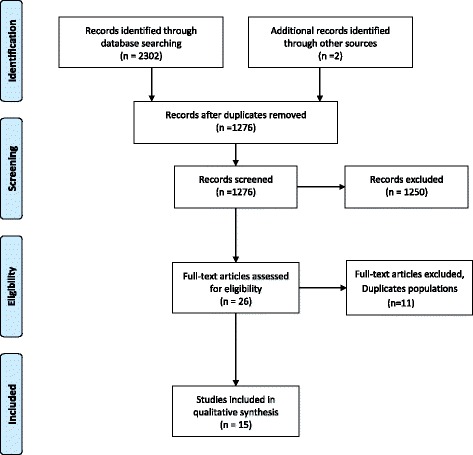
Study selection process for asbestos-smoking interaction
The same methodology was used for silica-smoking and diesel-smoking interactions. In the end, seven articles were included for silica-smoking interaction involving one cohort, one nested case–control study, and five case–control studies (Fig. 2). For diesel-smoking interaction, only two articles were included involving one nested case–control study and one pooled case–control study (Fig. 3).
Fig. 2.
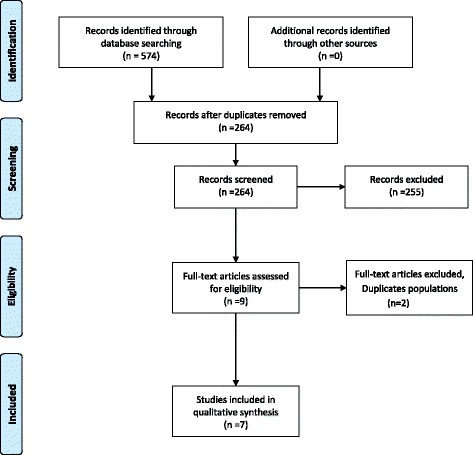
Study selection process for silica-smoking interaction
Fig. 3.
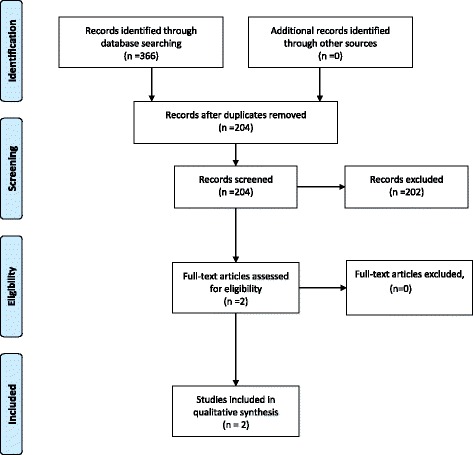
Study selection process for diesel-smoking interaction
The different phases of the study selection for the interactions between the three different occupational exposures and smoking are presented using the PRISMA 2009 Additional file 1 flow diagrams [16].
Occupational exposures and tobacco smoking interactions
Asbestos-smoking statistical interaction
The characteristics and the results of the six cohort studies and the case-cohort study evaluating asbestos-smoking statistical interaction are presented in Tables 1 and 2. Out of the seven studies, six studies assessed the multiplicative interaction; Multiplicative interaction was evaluated for the chrysotile workers of Qinghai mine in China [22], the crocidolite workers of Wittenoom mine in Australia [23], and the asbestos factory workers of East London [24]. The relative asbestos effect (RAE) with 95% confidence interval was calculated in the three studies, indicating the absence of a multiplicative interaction [22–24]. Additive and multiplicative interactions were evaluated for asbestos workers cohort in Great Britain [25]. Results showed that there is a positive additive interaction, but an absence of multiplicative interaction [25]. Additive and multiplicative interactions were also examined for the birth cohort of Quebec chrysotile miners and millers by calculating Rothman’s synergy index (S) and RAE, showing the absence of additive and multiplicative interactions [26]. The case-cohort study evaluated the interactions and showed the absence of additive and multiplicative interactions [27]. The additive interaction was assessed for a cohort of Chinese male asbestos plant workers by calculating S. The value of S was not significantly greater than one indicating the absence of additive interaction [28].
Table 1.
Description of cohort studies included in the systematic review for the asbestos-smoking interaction
| Author (Year) | Study design | Geographic area | Industry type | Fiber type | Outcome identification | Asbestos | Smoking | NOS | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Data collection | Exposure Identification | Non exposed | Exposed | Data collection | Non Smoker | Smoker | |||||||
| Berry (1985) [24] | Prospective | East London (UK) | Asbestos factory | Undetermined | Register | Employment record | Expert | Light and moderate | Severe | Questionnaire | Never | Ever | 6 |
| Liddell (2002) [26] | Prospective | Quebec (Canada) | Mining and Milling | Chrysotile | Death certificate | Employment record | Measures | <30 mpcf.y | ≥30 mpcf.y | Questionnaire | Never | Ever | 7 |
| Reid (2006) [23] | Prospective | Wittenoom (Australia) | Mining and Milling | Crocidolite | Register | -Questionnaire -Employment record |
Measures | Low | High | Questionnaire | Never and former >20 Y | Current and former <20 Y | 8 |
| Frost (2011) [25] | Prospective | Great Britain | Different types | Undetermined | Register | Questionnaire | Expert | <10 Y | ≥30 Y | Questionnaire | Never | Current | 8 |
| Wang (2012) [22] | Prospective | Qinghai (China) | Mining and Milling | Chrysotile | Death certificate | Employment record | Measures | Non miners and millers | Miners and millers | Interview | Never | Ever | 6 |
| Wang (2012) [28] | Prospective | China | Asbestos factory | Chrysotile | Death certificate | -Employment record -Questionnaire |
Measures | Electronics factory | Asbestos cohort | Questionnaire | Never | Ever | 7 |
| Offermans (2014) [27] | Case-cohort | Netherlands | Undetermined | Undetermined | Register | Questionnaire | Matrix | Never | Ever | Questionnaire | Never | Current | 7 |
NOS the Newcastle-Ottawa quality assessment Scale, S current smokers, mpcf.y million particles per cubic foot x years, Y years
Table 2.
Results of cohort studies included in the systematic review for the asbestos-smoking interaction
| Author (Year) | Subjects | Cases (sub-cohort) | Follow-up | NS/Exposed | S/Exposed | Interaction Estimation | Interpretation | ||
|---|---|---|---|---|---|---|---|---|---|
| Additive | Multiplicative | Additive | Multiplicative | ||||||
| Berry (1985) [24] | M: 1250 F: 420 |
M: 64 F: 15 |
1971–1980 | RR = 7.3 | RR = 2.4 | NA | RAE = 3.0 (0.8-7.5) | NA | No |
| Liddell (2002) [26] | M: 7279 | M: 533 | 1904–1992 | SMR = 0.62 | SMR = 1.71 | S = 1.1 (0.73-1.41) | RAE = 1.69 (0.87-3.28) | No | No |
| Reid (2006) [23] | M: 2550 F: 183 |
M: 132 F: 6 |
1979–2002 | OR = 2.02 (0.61–6.72) | OR = 1.64 (1.124–2.37) | NA | RAEm = 1.59 (0.12-20.50) | NA | No |
| Frost (2011) [25] | M: 93966 | M: 1768 | 1971–2005 | RR = 1.6 (0.6–4.2) | RR = 26.2 (13.0–53.1) | S = 1.4 (1.2-1.6) | V = 0.9 (0.3-2.4) | Positive | No |
| Wang (2012) [22] | M: 1539 | M: 50 | 1981–2006 | SMR = 1.79 (0.49-6.51) | SMR = 5.45 (4.11-7.22) | NA | RAE = 0.52 (0.07-1.11) | NA | No |
| Wang (2012) [28] | M: 577 | M: 53 | 1972–2008 | HR = 7.52 (0.90-62.79) | HR = 17.35 (2.38-126.57) | S = 1.41 (0.73-3.99) | NA | No | NA |
| Offermans (2014) [27] | M: 2324 | M: 2107 | 1986–2003 | HR = 1.79 (1.04–3.08) | HR = 10.21 (7.26–14.35) | RERI = 1.94 (0.13-4.89) | IT P = 0.50 | No | No |
M Males, F Females, S smokers, NS non-smokers, S Synergy Index, RERI Relative Excess Risk due to Interaction, V Multiplicativity Index, RAE Relative Asbestos Effect, RAE m the Modified Relative Asbestos Effect
The characteristics and the results of the eight case–control studies evaluating asbestos-smoking statistical interaction are presented in Tables 3 and 4. Seven of those studies did not reveal any multiplicative interaction when they were assessed [6, 29–34]. One case–control study, conducted in Sweden, evaluated the additive and multiplicative interactions and showed the absence of an additive interaction and the presence of a negative multiplicative interaction [35].
Table 3.
Description of case–control studies included in the systematic review for the asbestos-smoking interaction
| Author (Year) | Study design | Geographic area | Subjects identification | Asbestos | Smoking | NOS | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case | Control | Data collection | Exposure Identification | Non exposed | Exposed | Data collection | Non Smoker | Smoker | ||||
| Martischnig (1977) [29] | Hospital-based | United Kingdom | Hospital | Hospital | Questionnaire | Expert | No occupational history | Occupational history | Questionnaire | 0-14 C/D | >14 C/D | 7 |
| Blot (1978) [30] | Hospital-based | Coastal Georgia (USA) | -Hospital -Death certificate |
Hospital | Interview | Auto-declaration | Not shipbuilder | Shipbuilder | Interview | <10 C/D | ≥10 C/D | 6 |
| Jöckel (1998) [31] | Hospital-based | Germany | Hospital | Register | -Questionnaire -Interview |
Matrix | Never | Exposed >5280 h | -Questionnaire -Interview |
Never and < 27.1 P.Y | ≥27.1 P.Y | 7 |
| Gustavsson (2002) [35] | Population-based | Sweden | Register | Register | Self-reported questionnaire | Industrial hygienist | Never | ≥1.0 f-years | Self-reported questionnaire | Never | Current | 7 |
| Carel (2007) [32] | Hospital-based | Europe | Hospital | -Hospital -Register |
Questionnaire | Expert | Never | Exposed > 1 Y | Questionnaire | Never | Ever | 8 |
| De Matteis (2012) [6] | Population-based | Italy | Hospital | Population databases | Questionnaire | Matrix | Never | Ever | Questionnaire | Never | -Former -Current |
6 |
| Villeneuve (2012) [33] | Population-based | Canada | Register | General population | Self-reported questionnaire | Industrial hygienist | Never | Medium or high | Self-reported questionnaire | <10 P.Y | ≥10 P.Y | 7 |
| Lacourt (2015) [34] | Pooled | Montreal (Canada) | Hospital | Population (electoral lists) | Questionnaire | -Chemist -Industrial hygienist |
Never | Ever | Questionnaire | Never-low | Medium-heavy | 7 |
NOS the Newcastle-Ottawa quality assessment Scale, S current smokers, Y years, C/D cigarettes per day, P.Y Pack.Year
Table 4.
Results of case–control studies included in the systematic review for the asbestos-smoking interaction
| Author (Year) | Cases | Controls | Recruitment period | NS /Exposed | S/Exposed | Interaction Estimation | Interpretation | ||
|---|---|---|---|---|---|---|---|---|---|
| Additive | Multiplicative | Additive | Multiplicative | ||||||
| Martischnig (1977) [29] | M: 201 | M: 201 | 1972–1973 | RR = 1.08 | ≥25 C/D: RR = 3.26 |
NA | No heterogeneity of RRs X2 = 2.89; DF =2 | NA | No |
| Blot (1978) [30] | M: 458 | M: 553 | 1970–1976 | RR = 1.3 | RR = 1.7 RR = 2.4 |
NA | No heterogeneity of RRs P > 0.10 | NA | No |
| Jöckel (1998) [31] | M: 839 F: 165 |
M: 839 F: 165 |
1988-1993 | OR = 1.1 | OR = 6.5 OR = 18 |
NA | IT P = 0.73 |
NA | No |
| Gustavsson (2002) [35] | M: 1038 | M: 2359 | 1985–1990 | RR = 4.2 (1.6-11.1) | RR = 28.6 (19.9-48.3) | S = 1.15 (0.77-1.72) | IT OR = 0.31 (0.11-0.86) |
No | Negative |
| Carel (2007) [32] | M: 2205 | M: 2305 | 1998–2002 | Not shown | Not shown | NA | No modification effect CEE: P = 0.37 UK P = 0.62. | NA | No |
| De Matteis (2012) [6] | M: 1537 | M: 1617 | 2002–2005 | OR = 2.47 (1.15-5.31) | OR = 49.54 (28.18-87.08) | NA | LRT P = 0.19 |
NA | No |
| Villeneuve (2012) [33] | M: 1681 | M: 2053 | 1994–1997 | OR = 2.20 (0.42-11.41) | OR = 38.59 (10.78-138.08) | NA | IT P = 0.77 |
NA | No |
| Lacourt (2015) [34] | M: 414 | M: 321 | St.1: 1979–1986 St.2: 1996–1998 | OR = 1.2 (0.7–2.2) | OR = 1.1 (0.8–1.6) | NA | IT P = 0.68 |
NA | No |
M Males, F Females, S Smokers, NS Non-Smokers, CEE Central and Eastern Europe, St Study, S Synergy Index, LRT likelihood ratio test, IT interaction term
Silica-smoking statistical interaction
The characteristics and the results of the studies evaluating silica-smoking statistical interaction are presented in Tables 5 and 6. One cohort and one nested case–control study were reviewed and included. The cohort study, published in 2013, evaluated the additive and the multiplicative silica-smoking statistical interaction. The results of this study indicated the absence of additive and multiplicative interactions [36]. The nested case–control study examined the multiplicative interaction by adding an interaction term of crystalline silica exposure and smoking to the logistic regression, and showing the absence of a multiplicative interaction [37].
Table 5.
Description of silica-smoking and diesel-smoking interaction studies included in the systematic review
| Author (Year) | Study design | Geographic area | Industry type | Outcome identification | Silica | Smoking | NOS | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Data collection | Exposure Identification | Non exposed | Exposed | Data collection | Non Smoker | Smoker | ||||||
| Silica-smoking interaction studies | ||||||||||||
| Liu (2013) [36] | Prospective cohort | China | Metal mines and pottery factories | -Hospital record -Death certificate |
Employment record | Matrix | Never | Ever | Interview | Never | Ever | 8 |
| Fu (1994) [37] | Nested case–control | Guangxi province (China) | Tin miners | Death Certificate | -Employment record -Questionnaire |
Expert | Never | YUED | Questionnaire | Never | P.Y | 7 |
| Cassidy (2007) [38] | Multicenter hospital-based case–control | Europe | Undetermined | Hospital | Questionnaire | Industrial hygienist | Never | Ever | Questionnaire | Never | -Former -Current |
7 |
| De Matteis (2012) [6] | Population-based case–control | Italy | Undetermined | Hospital | -Questionnaire -Interview |
Matrix | Never | Ever | -Questionnaire -Interview |
Never | -Former -Current |
6 |
| Kachuri (2014) [39] | Population-based case–control | Canada | Undetermined | Register | Self-reported questionnaire | Industrial hygienist | Never | ≥30 Y | Self-reported questionnaire | <10 P.Y | ≥40 P.Y | 8 |
| Consonni (2015) [40] | Pooled case–control | Europe, Canada, Hong Kong and New Zealand | Bricklayers | -Register -Hospital |
Questionnaire | Matrix | Never bricklayers | Ever bricklayers | Questionnaire | Never | Ever | 8 |
| Lacourt (2015) [34] | Pooled case–control | Montreal (Canada) | Construction | Hospital | Questionnaire | Expert | Never | Substantial | Questionnaire | Never-low | Medium-heavy | 7 |
| Diesel-smoking interaction studies | ||||||||||||
| Silverman (2012) [41] | Nested case–control | USA | Non-metal mining facilities | -Register -Death certificate |
Computer-assisted telephone interview | Measures | Never | Tertiles | Computer-assisted telephone interview | Never | ≥2 P.D | 8 |
| Pintos (2012) [42] | Pooled case–control | Canada | Wide range of occupations and industries | Incident case | Questionnaire | -Chemist -Industrial hygienist |
Never | Substantial | Questionnaire | Never-low (0–15 P.Y) | Medium-heavy (>15 P.Y) | 7 |
NOS the Newcastle-Ottawa quality assessment Scale, S current smokers, Y years, YUED Years of Underground Exposure to Dust, P.Y Pack.Year
Table 6.
Results of silica-smoking and diesel-smoking interaction studies included in the systematic review
| Author (Year) | Subjects (cases) | Cases (controls) | Perioda | NS/Exposed | S/Exposed | Interaction Estimation | Interpretation | ||
|---|---|---|---|---|---|---|---|---|---|
| Additive | Multiplicative | Additive | Multiplicative | ||||||
| Silica-smoking interaction studies | |||||||||
| Liu (2013) [36] | 34018 | 546 | 1960–2003 | HR = 1.10 (0.68-1.78) | HR = 3.83 (2.48-5.90) | RERI = 0.98 (0.23-1.74) |
IT P = 0.25 |
No | No |
| Fu (1994) [37] | M: 79 | M: 188 | 1973–1989 | NA | NA | NA | IT P = 0.57 |
NA | No |
| Cassidy (2007) [38] | M: 2197 F: 655 |
M: 2295 F: 809 |
1998–2002 | OR = 1.41 (0.79 -2.49) | OR = 1.41 (1.07-1.87) | NA | Test for Heterogeneity P = 0.37 | NA | No |
| De Matteis (2012) [6] | M: 1537 | M: 1617 | 2002–2005 | OR = 1.41 (0.51-3.91) | OR = 44.98 (27.15-74.52) | NA | LRT P = 0.94 |
NA | No |
| Kachuri (2014) [39] | M: 1681 | M: 2053 | 1994–1997 | OR = 0.63 (0.26-1.52) | OR = 42.53 (23.54-76.83) | S = 2.38 (1.35-4.21) |
V = 3.59 (1.51-8.49) |
Positive | Positive |
| Consonni (2015) [40] | M: 15608 | M: 18531 | 1985–2010 | OR = 1.18 | OR = 18.5 | RERI = 6.80 (4.36-9.62) |
IT P = 0.28 |
Positive | No |
| Lacourt (2015) [34] | M: 241 | M: 196 | St.1: 1979–1986 St.2: 1996–1998 | OR = 3.1 (1.0–9.6) | OR = 1.4 (0.7–2.7) | NA | IT P = 0.02 |
NA | Negative |
| Diesel-smoking interaction studies | |||||||||
| Silverman (2012) [41] | M: 198 | M: 562 Ma | 1947–1977 | OR = 7.30 (1.46- 36.57) | OR = 17.38 (3.48-86.73) | NA | IT P = 0.086 |
NA | No |
| Pintos (2012) [42] | St. I: M: 857 St. II: M: 736 | St. I: M: 533 St. II: M: 894 | St. I: 1979–1986 St. II: 1996–2001 |
OR = 2.29 (1.1-4.6) | OR = 9.84 (6.4-15.1) | NA | IT OR = 1.15 (0.5-2.7) |
NA | No |
M Males, F Females, S Smokers, NS Non-Smokers, NA Not Applicable, S Synergy Index, V Multiplicativity Index, RERI Relative Excess Risk due to Interaction, LRT likelihood ratio test, IT interaction term
a: Follow-up or recruitment period
Five case–control studies were reviewed in this study to assess the silica-smoking statistical interaction. Two studies, one conducted in several centers in Europe and the other in Italy, showed that there is no multiplicative interaction [6, 38]. A study published in 2015, evaluated the multiplicative interaction between the exposure of construction workers to crystalline silica and smoking. The study showed a negative multiplicative interaction; the effect of occupational exposure to crystalline silica was higher for non/light smokers than for medium/heavy smokers [34]. A population-based case–control study in eight Canadian provinces showed positive additive and positive multiplicative interactions [39]. Another pooled case–control study (SYNERGY study) showed positive additive interaction, but no multiplicative interaction [40].
Diesel-smoking statistical interaction
Only two articles assessed the diesel-smoking statistical interaction were included in our review (Table 5). These two studies presented a nested case–control study of the workers of eight non-metal mining facilities in United States [41] and a pooled case control study conducted in Montreal (Canada) [42]. The results of these two studies (Table 6) showed the absence of a multiplicative interaction [41, 42].
Discussion
Overall, this review suggests the absence of a multiplicative statistical interaction between the three most frequent occupational lung carcinogens, asbestos, crystalline silica and diesel engine exhaust emissions and tobacco smoking. On the other side, there is no enough evidence from the literature to conclude on the additive statistical interaction.
Asbestos-smoking statistical interaction
Four meta-analyses were conducted to evaluate the asbestos-smoking statistical interaction; one demonstrated a negative multiplicative interaction [43], and three suggested the presence of a positive additive interaction [13–15]. The most recent systematic review published in 2015 indicated the presence of a positive additive interaction and the absence of multiplicative interaction [15]. While we agreed about the absence of a multiplicative interaction, from this systematic review, the presence of a positive additive interaction is less clear. Indeed, out of the five original studies included in this review, only one showed a significant positive additive interaction. This discordance is mainly attributable to selection criteria of original studies. While in the most recent meta-analysis, authors included all studies from which they could assess statistical interaction from odds ratios or relative risks reported in the original studies without any notion of statistical significance [15], in the present systematic review, we add more stringent inclusion criteria. Indeed, we only included and evaluated studies that reported both the interaction results on a specified scale (multiplicative or additive) and the significance of the results, either in terms of confidence intervals or p-value,. However, conclusions from our study are based on a systematic review of the literature and we did not perform a meta-analysis since it was not the primary aim of this study to focus exclusively on the asbestos-smoking statistical interaction. Instead, the present study aimed at assessing the statistical interactions between the most frequent occupational lung carcinogen and tobacco-smoking. Despite the recent publication of a meta-analysis assessing the asbestos-smoking statistical interaction, performing a new one using more stringent inclusion criteria for studies should be considered.
Silica-smoking and diesel smoking statistical interaction
Similarly to asbestos-smoking statistical interaction, for both silica-smoking as well as diesel-smoking statistical interaction, the absence of a multiplicative statistical interaction seems to be consensual. Regarding additive interaction, for both silica-smoking and diesel-smoking statistical interaction, it is impossible to conclude on the presence of a statistical interaction on the additive scale. Indeed, for silica-smoking interactions, it is impossible to conclude due to discrepancies between original studies whereas for diesel-smoking interaction, no studies included in the present systematic review have addressed this issue.
Methodological points in original studies
The inconsistency of the statistical interaction results between original studies may come from methodological differences in each study. Every study has limitations that could be the source of opposite results on the interaction evaluation. In the studies that were included, occupational histories and smoking details were collected using employment records or questionnaires. The reliability of the data may have been affected by the quality of the documentation in the records and by the recall bias from the questionnaires used to collect retrospective data. Although the data collection could be complete and accurate, the methods used to identify and assess occupational exposures may also have been a source of bias. For example; the utilization of a job-exposure matrix (JEM) could introduce non-differential misclassifications leading to a large number of false-positives and false-negatives. In consequence, there is a risk of underestimated risks that could affect the evaluation of the interaction [44, 45].
When evaluating interactions, the method and the scale used to examine the interaction should be reported to avoid confusion and ambiguity and facilitate the comparison between studies [46]. In fact, the best approach is to evaluate the statistical interaction on both additive and multiplicative scales [19]. The additive interaction is generally evaluated by using the difference of risk differences known as interaction contrast, while risk ratios are used to evaluate the multiplicative interactions. In cohort studies, risks and risk ratios can be easily generated, but in the case–control studies only the odds ratios can be estimated. Using odds ratios instead of risk ratios to evaluate the additive or the multiplicative interaction could mistakenly show the presence of a positive interaction, even if the outcome is rare [47, 48]. The majority of the reviewed case–control studies evaluated exclusively the multiplicative interaction by testing the significance of the interaction term introduced into the regression model. However, while rarely used, some authors have proposed various measures to assess the additive interaction from case–control data using logistic regression models [49–52]. Additionally, discrepancy between studies may be explained by the measures used to assess the statistical additive interaction as each measure has its own interpretation. Indeed, Rothman et al. and Kalilani et al. suggested to use simultaneously three measures of interaction to evaluate the additive interaction: the attributable proportion due to interaction (AP), the relative excess risk due to interaction (RERI), and the Rothman’s synergy index (S) [53, 54]. Although, the attributable proportion due to interaction (AP) is the most robust measure to evaluate the additive interaction when the odds ratios are used instead of the risk ratios in the equation [54]. Because of its more intuitive interpretation, the Rothman’s synergy index (S) [55] was used in the majority of the included studies to evaluate the additive statistical interaction even when odds ratios were used instead of risk ratios. Indeed, both S and AP measure interaction as departure from additivity but only S is suitable under a negative additive interaction assumption. Specific measures of interaction have been proposed to assess the statistical multiplicative interaction between asbestos exposure and tobacco smoking. The RAE was proposed to evaluate the asbestos-smoking multiplicative interaction in cohort studies [24]. However it was shown that the RAE tended to be underestimated in studies with low level of asbestos exposure. Thus, a modified version of the RAE (RAEm) have been proposed to assess the asbestos-smoking multiplicative interaction in studies with low asbestos exposure level [43].
In many of the reviewed articles, the conclusion regarding the statistical interaction was not always consistent with the results of our evaluation; authors suggested the presence of a positive interaction without evaluating the statistically significance of the measure, or conclude on both scales although the interaction was evaluated on one scale only. The same findings was discussed by Liddell (2001); authors continue to suggest the presence of a positive multiplicative asbestos-smoking interaction without enough or strong evidence from their results or from the literature [56].
In the current review, our conclusions are based on strong evidence, as the majority of the reviewed studies conclude the absence of the multiplicative interaction. In addition, all precautions were taken to avoid missing papers; three different bibliographic databases were used and each reference list of all included studies was reviewed. Finally, we believe that the publication bias is limited as several papers with negative results were published.
Public health implications
Statistical interaction (whatever the model, multiplicative or additive) between two risk factors increases cancer risk compared to risk related to each factors acting independently.
Two main impacts can be considered from a public health point of view. First, regarding primary prevention, reducing exposure to those two risk factors will induce a greater benefice (number of avoided incident cases) if there is a significant interaction between those two factors. Secondly, regarding targeted screening program (screening proposed to a selected population according to a specific risk threshold), the existence of an interaction will decrease the level of exposure of those two factors corresponding to the defined risk threshold. The same argument could be applied to individual imputability used in compensation system. Therefore, the knowledge of a statistical interaction between two risk factors is crucial and the knowledge of the interaction scale (i.e. multiplicative or additive) is important to conduct risk assessment and risk management.
Besides, in the light of the current knowledge, the statistical interaction between two factors do not allow to infer strong hypothesis about biological mechanisms
Conclusions
To our knowledge, this is the first systematic review conducted to evaluate the statistical interactions between occupational exposures to crystalline silica and diesel engine exhaust emissions and tobacco smoking. In general, there is no multiplicative interaction between the three most frequent occupational lung carcinogens and the tobacco smoking. Evidence found in the literature cannot be considered sufficient to conclude on the additive scale. To minimize the risk of lung cancer among workers, specific programs should be developed and promoted to reduce concomitantly the exposure to occupational lung carcinogens and tobacco smoking.
Acknowledgments
Not applicable.
Funding
This research was funded by the Agence nationale de sécurité sanitaire de l’alimentation, de l’environnement et du travail (ANSES) (Grant: ANSES EST-2011/1/189). ANSES was not involved in the design of the study, the interpretation of the results, or the writing of the manuscript.
Availability of data and materials
Relevant data are available within the manuscript and the additional file.
Authors’ contributions
MZ conducted the literature review, the study selection process, the data extraction and prepared the first draft for all sections of this manuscript with the help and supervision of PS, PB and AL. FD reviewed the eligibility of the included studies and the accuracy of the extracted data and contributed to the interpretation and discussion of findings. IS contributed to the interpretation of the statistical interaction results of the original studies included in the systematic review. PB and PS contributed to interpretation and discussion of findings. AL supervised all aspects of this manuscript, from the study selection process to the interpretation and discussion of findings. All co-authors participated in the editing and correction of the final text, and they read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Abbreviations
- AP
the attributable proportion due to interaction
- IARC
International agency for research on cancer
- NOS
The Newcastle-Ottawa quality assessment scale
- RAE
the relative asbestos effect
- RAEm
the modified version of the relative asbestos effect
- RERI
Relative excess risk due to interaction
- S
Rothman’s synergy index
Additional files
PRISMA 2009 Checklist. (DOC 62 kb)
Statistical Interaction Evaluation. (DOCX 72 kb)
Contributor Information
Mohamad El Zoghbi, Email: zoghbi2001@hotmail.com.
Pascale Salameh, Email: pascalesalameh1@hotmail.com.
Isabelle Stücker, Email: isabelle.stucker@inserm.fr.
Patrick Brochard, Email: patrick.brochard@chu-bordeaux.fr.
Fleur Delva, Email: fleur.delva@isped.u-bordeaux2.fr.
Aude Lacourt, Phone: +33 5 57 57 16 23, Email: aude.lacourt@isped.u-bordeaux2.fr.
References
- 1.Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. doi: 10.3322/caac.20138. [DOI] [PubMed] [Google Scholar]
- 2.Torre AL, Bray F, Siegel LR, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. doi: 10.3322/caac.21262. [DOI] [PubMed] [Google Scholar]
- 3.IARC. Evaluation of the Carcinogenic Risk of Chemicals to Humans. Tobacco Smoking, vol. 38. Lyon: IARC; 1986. [PubMed]
- 4.Pesch B, Kendzia B, Gustavsson P, Jöckel K-H, Johnen G, Pohlabeln H, Olsson A, Ahrens W, Gross MI, Brüske I, et al. Cigarette smoking and lung cancer--relative risk estimates for the major histological types from a pooled analysis of case–control studies. Int J Cancer. 2012;131:1210–1219. doi: 10.1002/ijc.27339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.CDC Annual smoking-attributable mortality, years of potential life lost, and productivity losses--United States, 1997–2001. MMWR Morb Mortal Wkly Rep. 2005;54:625–628. [PubMed] [Google Scholar]
- 6.De Matteis S, Consonni D, Lubin JH, Tucker M, Peters S, Vermeulen R, Kromhout H, Bertazzi PA, Caporaso NE, Pesatori AC, et al. Impact of occupational carcinogens on lung cancer risk in a general population. Int J Epidemiol. 2012;41(3):711–721. doi: 10.1093/ije/dys042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. List of classifications by cancer site. Lyon: IARC; 2016.
- 8.Van Tongeren M, Jimenez SA, Hutchings JS, MacCalman L, Rushton L, Cherrie WJ. Occupational cancer in Britain. Exposure assessment methodology. Br J Cancer. 2012;107(Suppl 1):S18–S26. doi: 10.1038/bjc.2012.114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Peters EC, Ge BC, Hall LA, Davies WH, Demers AP. CAREX Canada: an enhanced model for assessing occupational carcinogen exposure. Occup Environ Med. 2015;72:64–71. doi: 10.1136/oemed-2014-102286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.IARC. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Arsenic, Metals, Fibres, and Dusts, vol. 100C. Lyon: IARC; 2012. [PMC free article] [PubMed]
- 11.IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Diesel and Gasoline Engine Exhausts and Some Nitroarenes, vol. 105. Lyon: IARC; 2013. [PMC free article] [PubMed]
- 12.Nelson ED, Emont LS, Brackbill MR, Cameron LL, Peddicord J, Fiore CM. Cigarette smoking prevalence by occupation in the United States. A comparison between 1978 to 1980 and 1987 to 1990. J Occup Med. 1994;36:516–525. [PubMed] [Google Scholar]
- 13.Erren TC, Jacobsen M, Piekarski C. Synergy between asbestos and smoking on lung cancer risks. Epidemiology (Cambridge, Mass) 1999;10(4):405–411. doi: 10.1097/00001648-199907000-00011. [DOI] [PubMed] [Google Scholar]
- 14.Wraith D, Mengersen K. A Bayesian approach to assess interaction between known risk factors: the risk of lung cancer from exposure to asbestos and smoking. Stat Methods Med Res. 2007;17. [DOI] [PubMed]
- 15.Ngamwong Y, Tangamornsuksan W, Lohitnavy O, Chaiyakunapruk N, Scholfield CN, Reisfeld B, Lohitnavy M. Additive Synergism between Asbestos and Smoking in Lung Cancer Risk: A Systematic Review and Meta-Analysis. PloS One. 2015;10(8):e0135798. doi: 10.1371/journal.pone.0135798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Moher D, Liberati A, Tetzlaff J, Altman GD. Group PRISMA. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1. doi: 10.1186/2046-4053-4-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rothman JK, Greenland S, Lash LT. Modern epidemiology. Lyon: Lippincott Williams & Wilkins; 2008.
- 19.Rothman JK. Epidemiology: An Introduction. USA: Oxford University Press; 2002. [Google Scholar]
- 20.Sanderson S, Tatt DI, Higgins TJP. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: a systematic review and annotated bibliography. Int J Epidemiol. 2007;36:666–676. doi: 10.1093/ije/dym018. [DOI] [PubMed] [Google Scholar]
- 21.The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed 8 July 2016.
- 22.Wang X, Lin S, Yano E, Qiu H, Yu IT, Tse L, Lan Y, Wang M. Mortality in a Chinese chrysotile miner cohort. Int Arch Occup Environ Health. 2012;85(4):405–412. doi: 10.1007/s00420-011-0685-9. [DOI] [PubMed] [Google Scholar]
- 23.Reid A, de Klerk NH, Ambrosini GL, Berry G, Musk AW. The risk of lung cancer with increasing time since ceasing exposure to asbestos and quitting smoking. Occup Environ Med. 2006;63(8):509–512. doi: 10.1136/oem.2005.025379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Berry G, Newhouse ML, Antonis P. Combined effect of asbestos and smoking on mortality from lung cancer and mesothelioma in factory workers. Br J Ind Med. 1985;42(1):12–18. doi: 10.1136/oem.42.1.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Frost G, Darnton A, Harding AH. The effect of smoking on the risk of lung cancer mortality for asbestos workers in Great Britain (1971–2005) Ann Occup Hyg. 2011;55(3):239–247. doi: 10.1093/annhyg/meq089. [DOI] [PubMed] [Google Scholar]
- 26.Liddell FD, Armstrong BG. The combination of effects on lung cancer of cigarette smoking and exposure in quebec chrysotile miners and millers. Ann Occup Hyg. 2002;46(1):5–13. doi: 10.1093/annhyg/mef008. [DOI] [PubMed] [Google Scholar]
- 27.Offermans NS, Vermeulen R, Burdorf A, Goldbohm RA, Kauppinen T, Kromhout H, van den Brandt PA. Occupational asbestos exposure and risk of pleural mesothelioma, lung cancer, and laryngeal cancer in the prospective Netherlands cohort study. J Occup Environ Med. 2014;56(1):6–19. doi: 10.1097/JOM.0000000000000060. [DOI] [PubMed] [Google Scholar]
- 28.Wang X, Yano E, Qiu H, Yu I, Courtice MN, Tse LA, Lin S, Wang M. A 37-year observation of mortality in Chinese chrysotile asbestos workers. Thorax. 2012;67(2):106–110. doi: 10.1136/thoraxjnl-2011-200169. [DOI] [PubMed] [Google Scholar]
- 29.Martischnig KM, Newell DJ, Barnsley WC, Cowan WK, Feinmann EL, Oliver E. Unsuspected exposure to asbestos and bronchogenic carcinoma. Br Med J. 1977;1(6063):746–749. doi: 10.1136/bmj.1.6063.746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Blot WJ, Harrington JM, Toledo A, Hoover R, Heath CW, Jr, Fraumeni JF., Jr Lung cancer after employment in shipyards during World War II. N Engl J Med. 1978;299(12):620–624. doi: 10.1056/NEJM197809212991202. [DOI] [PubMed] [Google Scholar]
- 31.Jöckel KH, Ahrens W, Jahn I, Pohlabeln H, Bolm-Audorff U. Occupational risk factors for lung cancer: a case–control study in West Germany. Int J Epidemiol. 1998;27(4):549–560. doi: 10.1093/ije/27.4.549. [DOI] [PubMed] [Google Scholar]
- 32.Carel R, Olsson AC, Zaridze D, Szeszenia-Dabrowska N, Rudnai P, Lissowska J, Fabianova E, Cassidy A, Mates D, Bencko V, et al. Occupational exposure to asbestos and man-made vitreous fibres and risk of lung cancer: a multicentre case–control study in Europe. Occup Environ Med. 2007;64(8):502–508. doi: 10.1136/oem.2006.027748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Villeneuve PJ, Parent ME, Harris SA, Johnson KC. Occupational exposure to asbestos and lung cancer in men: evidence from a population-based case–control study in eight Canadian provinces. BMC Cancer. 2012;12:595. doi: 10.1186/1471-2407-12-595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Lacourt A, Pintos J, Lavoue J, Richardson L, Siemiatycki J. Lung cancer risk among workers in the construction industry: results from two case–control studies in Montreal. BMC Public Health. 2015;15(1):941. doi: 10.1186/s12889-015-2237-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Gustavsson P, Nyberg F, Pershagen G, Scheele P, Jakobsson R, Plato N. Low-dose exposure to asbestos and lung cancer: dose–response relations and interaction with smoking in a population-based case-referent study in Stockholm, Sweden. Am J Epidemiol. 2002;155(11):1016–1022. doi: 10.1093/aje/155.11.1016. [DOI] [PubMed] [Google Scholar]
- 36.Liu Y, Steenland K, Rong Y, Hnizdo E, Huang X, Zhang H, Shi T, Sun Y, Wu T, Chen W. Exposure-response analysis and risk assessment for lung cancer in relationship to silica exposure: a 44-year cohort study of 34,018 workers. Am J Epidemiol. 2013;178(9):1424–1433. doi: 10.1093/aje/kwt139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Fu H, Gu X, Jin X, Yu S, Wu K, Guidotti TL. Lung cancer among tin miners in southeast China: silica exposure, silicosis, and cigarette smoking. Am J Ind Med. 1994;26(3):373–381. doi: 10.1002/ajim.4700260311. [DOI] [PubMed] [Google Scholar]
- 38.Cassidy A, t Mannetje A, van Tongeren M, Field JK, Zaridze D, Szeszenia-Dabrowska N, Rudnai P, Lissowska J, Fabianova E, Mates D, et al. Occupational exposure to crystalline silica and risk of lung cancer: a multicenter case–control study in Europe. Epidemiology (Cambridge, Mass) 2007;18(1):36–43. doi: 10.1097/01.ede.0000248515.28903.3c. [DOI] [PubMed] [Google Scholar]
- 39.Kachuri L, Villeneuve PJ, Parent ME, Johnson KC, Harris SA, Canadian Canc R. Occupational exposure to crystalline silica and the risk of lung cancer in Canadian men. Int J Cancer. 2014;135(1):138–148. doi: 10.1002/ijc.28629. [DOI] [PubMed] [Google Scholar]
- 40.Consonni D, De Matteis S, Pesatori CA, Bertazzi AP, Olsson CA, Kromhout H, Peters S, Vermeulen HRC, Pesch B, Brüning T, et al. Lung cancer risk among bricklayers in a pooled analysis of case–control studies. Int J Cancer. 2015;136:360–371. doi: 10.1002/ijc.28986. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Silverman DT, Samanic CM, Lubin JH, Blair AE, Stewart PA, Vermeulen R, Coble JB, Rothman N, Schleiff PL, Travis WD, et al. The diesel exhaust in miners study: A nested case–control study of lung cancer and diesel exhaust. J Natl Cancer Inst. 2012;104(11):855–868. doi: 10.1093/jnci/djs034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Pintos J, Parent ME, Richardson L, Siemiatycki J. Occupational exposure to diesel engine emissions and risk of lung cancer: Evidence from two case - Control studies in Montreal, Canada. Occup Environ Med. 2012;69(11):787–792. doi: 10.1136/oemed-2012-100964. [DOI] [PubMed] [Google Scholar]
- 43.Berry G, Liddell FD. The interaction of asbestos and smoking in lung cancer: a modified measure of effect. Ann Occup Hyg. 2004;48(5):459–462. doi: 10.1093/annhyg/meh023. [DOI] [PubMed] [Google Scholar]
- 44.Bouyer J, Dardenne J, Hémon D. Performance of odds ratios obtained with a job-exposure matrix and individual exposure assessment with special reference to misclassification errors. Scand J Work Environ Health. 1995;21:265–271. doi: 10.5271/sjweh.36. [DOI] [PubMed] [Google Scholar]
- 45.Kauppinen PT, Mutanen OP, Seitsamo TJ. Magnitude of misclassification bias when using a job-exposure matrix. Scand J Work Environ Health. 1992;18:105–112. doi: 10.5271/sjweh.1604. [DOI] [PubMed] [Google Scholar]
- 46.Ahlbom A, Alfredsson L. Interaction: A word with two meanings creates confusion. Eur J Epidemiol. 2005;20:563–564. doi: 10.1007/s10654-005-4410-4. [DOI] [PubMed] [Google Scholar]
- 47.Morabia A, Ten Have T, Landis JR. Interaction fallacy. J Clin Epidemiol. 1997;50(7):809–812. doi: 10.1016/S0895-4356(97)00053-X. [DOI] [PubMed] [Google Scholar]
- 48.Campbell BU, Gatto MN, Schwartz S. Distributional interaction: Interpretational problems when using incidence odds ratios to assess interaction. Epidemiol Perspect Innov. 2005;2:1. doi: 10.1186/1742-5573-2-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Knol JM, van der Tweel I, Grobbee ED, Numans EM, Geerlings IM. Estimating interaction on an additive scale between continuous determinants in a logistic regression model. Int J Epidemiol. 2007;36:1111–1118. doi: 10.1093/ije/dym157. [DOI] [PubMed] [Google Scholar]
- 50.Assmann FS, Hosmer WD, Lemeshow S, Mundt AK. Confidence intervals for measures of interaction. Epidemiology (Cambridge, Mass) 1996;7:286–290. doi: 10.1097/00001648-199605000-00012. [DOI] [PubMed] [Google Scholar]
- 51.Hosmer WD, Lemeshow S. Confidence interval estimation of interaction. Epidemiology (Cambridge, Mass) 1992;3:452–456. doi: 10.1097/00001648-199209000-00012. [DOI] [PubMed] [Google Scholar]
- 52.Katsoulis M, Bamia C. Additive interaction between continuous risk factors using logistic regression. Epidemiology (Cambridge, Mass) 2014;25(3):462–464. doi: 10.1097/EDE.0000000000000083. [DOI] [PubMed] [Google Scholar]
- 53.Rothman JK. Modern Epidemiology. 1986. [Google Scholar]
- 54.Kalilani L, Atashili J. Measuring additive interaction using odds ratios. Epidemiol Perspect Innov. 2006;3:5. doi: 10.1186/1742-5573-3-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Skrondal A. Interaction as departure from additivity in case–control studies: a cautionary note. Am J Epidemiol. 2003;158:251–258. doi: 10.1093/aje/kwg113. [DOI] [PubMed] [Google Scholar]
- 56.Liddell FD. The interaction of asbestos and smoking in lung cancer. Ann Occup Hyg. 2001;45(5):341–356. doi: 10.1093/annhyg/45.5.341. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Relevant data are available within the manuscript and the additional file.