

Abstract
Although endoscopic submucosal dissection (ESD) is widely accepted as a curative treatment method for early gastric cancer (EGC) worldwide, metachronous recurrence often occurs after ESD for EGC. However, there are insufficient data about the role of Helicobacter pylori (H. pylori) infection and other risk factors for recurrence. We aimed to compare the metachronous lesion in the H. pylori persistent group and the eradicated group, and to identify risk factors for metachronous lesion. We retrospectively analyzed 782 patients who underwent ESD between January 2008 and December 2013. We excluded patients with dysplasia or patients who were not tested for H. pylori infection. One hundred eighty-five patients were enrolled. We studied risk factors for recurrence, and used survival analysis to test. There were 24 patients with metachronous recurrence after ESD for EGC among the group. The incidence of metachronous gastric lesions after ESD for EGC developed more in the over 70-year-old group (P = 0.025) and more in the H. pylori persistent group (P = 0.008). In conclusion, H. pylori infection and old age are independent risk factors for metachronous gastric lesions after ESD in EGC.
Keywords: Gastric Cancer, Endoscopic Submucosal Dissection, Metachronous Recurrence
Graphical Abstract
INTRODUCTION
Gastric cancer, which is the fourth most common cancer worldwide (1), occurs especially in Korea, Japan, China, and Far East Asia (2). Helicobacter pylori (H. pylori) infection triggers chronic gastritis (3), and causes atrophy and metaplasia (4). International Agency for Research on Cancer, the agency within World Health Organization (WHO), designates H. pylori as a Group 1 carcinogen (5). Results of a meta-analysis showed that H. pylori infection confers a two- or three-fold increase in the risk of gastric cancer development (6).
Early gastric cancer (EGC), by definition, is limited to the mucosa and submucosa layer regardless of lymph node metastasis (7). It was recommended that endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) served as a standard treatment of EGC. ESD and EMR are likely to cause complete resection and en bloc resection, even though those were technically hard to perform (7,8). It was suggested that H. pylori eradication could reduce the likelihood of gastric cancer occurrence (9). However, it was still controversial that H. pylori eradication showed preventive effects for the metachronous lesion following endoscopic resection. Japanese Gastric Cancer Association prescribed ESD for the standard treatment when absolute indication and extended indication were applied to the EGC treatment (10), and its numbers have increased. Some studies about the possibility of predicting relapse of H. pylorus microorganism after treating the ESD have revealed that H. pylori eradication contributed to the prevention of metachronous gastric cancer (11,12,13). However, other scholars failed to prove its effect on prevention (14,15).
The purpose of this study was to investigate the preventive effect of H. pylori eradication in generating metachronous gastric neoplasm among patients who received the ESD for the EGC treatment, and find other risk factors causing metachronous gastric lesion.
MATERIALS AND METHODS
Patients and study design
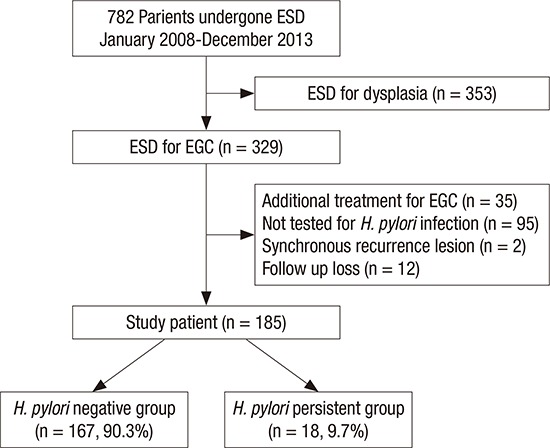
Seven hundred eighty-two patients, excluding patients with a short follow-up duration under 24 months after treating with ESD, were treated with the ESD from January 2008 to December 2013 (60 months) in Gil Medical Center, Incheon, Korea. Three hundred twenty-nine patients in this group were diagnosed with the EGC. We excluded 2 patients having synchronous lesions, 12 patients missing follow-up, 35 patients implementing immediate additional gastrectomy after ESD, and 95 patients who were not tested for H. pylori infection using a breath test, histology, and rapid urease tests from the 329 patients stated above (Fig. 1).
Fig. 1.

Patients and study design.
ESD = endoscopic submucosal dissection, EGC = early gastric cancer.
Therefore, a total of 185 patients were enrolled in this retrospective study. Patients were separated into 2 groups; the negative group (n = 167) included patients who tested negative and experienced eradication after positive testing, while the persistent group (n = 18) encompassed patients who did not experience microorganism removal and patients who did not receive the treatment for H. pylori despite positive testing (Fig. 1).
Their median age was 67.4 years (45–87 years) and there were 57 smokers (30.8%) in the population. The median period of following patients was 61.5 months with a range of 24 to 96 months. Clinicopathological variables, such as age, sex, follow-up duration, number of lesions, tumor location, tumor size, endoscopic gross appearance, pathological result, depths of lesion, smoking, and drinking were captured from medical charts via clinical data retrieving and electronic medical record searching systems.
Because we reviewed patients' medical records from January 2008 to December 2013, it was not possible to receive patients' informed consents. As our study method had very low risk to patients, the IRB approved our study without requiring informed consents.
ESD technique and follow-up schedule
All ESDs were performed by using an insulated-tip knife (KD-610L; Olympus Medical, Tokyo, Japan). The typical procedure was en bloc resection that involved the procedure of marking, mucosal incision, and submucosal dissection. After treating ESD, specimens were sent to the pathology department and were labeled by the Vienna classification (16). The surveillance esophagoduodenoscopy was carried out after treating ESD respectively using GIF-Q240, GIF-Q260J, GIF-Q260, GIF-H260 (Olympus medical) each 3, 6, 12, 18, and 24 months. The esophagogastroduodenoscopy (EGD) was performed every year after 24 months and included a biopsy from the ESD site.
We defined recurrence as a methachronous lesion occurring over 6 months following the initial ESD. The abdominal computed tomography (CT) was carried out for discerning between distant metastasis and lymph node metastasis. The CT was obtained every 6 months within the first year and every year after that.
Determination of H. pylori status and eradication
All the patients (n = 169) in the H. pylori negative group were H. pylori negative on the histopathology test with Hematoxylin and Eosin (HE) stain, Wright-Giemsa stain of the resected specimen, urea breath tests (UBTs), and rapid urease tests (HP kit; CKD Bio Corp., Seoul, Korea). However, the H. pylori positive group was defined when H. pylori showed a positive on at least 1 test among all of the tests. The treatment of H. pylori eradication therapy was carried out based on Korean guidelines for H. pylori infection (17). The first line treatment included amoxicillin, clarithromycin and the standard dose of proton-pump inhibitor (PPI), taken twice a day for a week. If it failed, the second line regimen was administered for a week. This regimen consisted of 4 drugs: metronidazole 250 mg 3 times a day, tetracycline 500 mg 4 times a day, bismuth 240 mg 4 times a day and PPI standard dose twice a day. The UBT and rapid urease tests were used to confirm the successful H. pylori eradication. The negative group was defined when 2 tests were negative.
Histopathological examination of gastric lesion
Our 2 expert pathologists examined both resected specimens through the ESD and specimens through the biopsy. Historical classification of the gastric cancer complied with the new Japanese classification (16). The occurrence of metachronous neoplasm was defined when the dysplasia and carcinoma occurred more than 6 months after ESD.
Statistical analysis
Baseline data were obtained from our prospectively collected electronic medical records. All numerical variables, such as age, follow-up duration, and maximum diameters of lesions, were expressed as the mean standard deviation. Chi-square test and Fisher's exact test were applied to compare 2 groups and metachronous recurrence. Student's t-test was used for non-categorical variables in the intergroup comparison of clinical pathological characteristics. The threshold for statistical significance was set at P < 0.05. Recurrence-free survival and the incidence of metachronous gastric cancer were calculated using the Kaplan-Meier method, and compared between 2 groups by log-rank test. A Cox proportional hazards model and multivariate analyses were used for risk assessment. Statistical analyses were performed using the Statistical Package for Social Science Version 18.0 (SPSS Inc., Chicago, IL, USA).
Ethics statement
The study protocol was approved by the Institutional Review Board of Gachon University Gil Medical Center (GAIRB No. 2016-173). The IRB approved our study without informed consents.
RESULTS
A total of 185 patients were enrolled in our study. Of the 185 patients enrolled, 141 were male and 44 were female with a median age of 67.4. During the follow-up period, metachronous lesions were found in 24 (13.0%) of the 185 patients. The clinicopathological characteristics of patients according to the development of metachronous neoplasms are shown in Table 1. There were no statistically significant differences between the 2 groups in terms of the sex ratio, smoking and alcohol consumption history, location and gross appearance, the diameter, multiplicity or the depth of the tumor. However, there were statistically significant differences in age (P = 0.048) and H. pylori status (P = 0.003) between the patients with metachronous lesions and without metachronous lesions.
Table 1. Clinicopathologic characteristics of patients with and without metachronous lesion.
| Parameters | Patients with ML (n = 24) | Patients without ML (n = 161) | P value |
|---|---|---|---|
| Mean age, yr | 71.25 ± 8.06 | 66.82 ± 10.09 | |
| < 70 | 9 (37.5) | 95 (59.0) | 0.048 |
| ≥ 70 | 15 (62.5) | 66 (41.0) | |
| Sex (male) | 19 (79.2) | 122 (75.8) | 0.716 |
| Location | 0.374 | ||
| Upper 1/3 | 0 (0.0) | 10 (6.2) | |
| Middle 1/3 | 9 (37.5) | 43 (26.7) | |
| Lower 1/3 | 15 (62.5) | 108 (67.1) | |
| Gross appearance | 0.731 | ||
| Elevated | 2 (8.3) | 18 (11.2) | |
| Flat | 7 (29.2) | 59 (36.6) | |
| Depressed | 15 (62.5) | 84 (52.2) | |
| Maximum diameter of lesion, mm | 14.08 ± 7.96 | 14.74 ± 8.61 | 0.248 |
| Multiplicity | 1 (4.2) | 5 (3.1) | 0.571 |
| Depth of invasion | 0.476 | ||
| M | 23 (95.8) | 143 (88.8) | |
| SM | 1 (4.2) | 18 (11.2) | |
| H.P. status | 0.003 | ||
| Eradicated | 17 (70.8) | 150 (93.2) | |
| Persistent | 7 (29.2) | 11 (6.8) | |
| Smoking | 4 (16.7) | 53 (32.9) | 0.108 |
| Alcohol | 11 (45.8) | 73 (45.3) | 0.964 |
Values are presented as mean ± SD or number (%).
ML = metachronous lesion, M = mucosa, SM = submucosa, H.P. = Helicobacter pylori.
Metachronous lesions consisted of adenocarcinoma (12 patients, 50.0%), high grade dysplasia (7 patients, 29.1%), and low grade dysplasia (5 patients, 20.9%). H. pylori persistent group included 16 patients who did not receive eradication treatment though the test result showed positive, and 2 patients consistently appearing positive results of H. pylori examinations after second line therapy. The median time to recurrence was 24 months, with a range of 6 to 75 months. We calculated cumulative incidence of the metachronous recurrence between the H. pylori persistent group and negative group using Kaplan-Meier method. The risk of cumulative incidence of the metachronous recurrence in the H. pylori persistent group was higher than the negative group (P = 0.008) (Fig. 2). We also analyzed a risk of cumulative incidence of the metachronous recurrence in age by using Kaplan-Meier method. There was higher risk in the over 70-years-old group (P = 0.025) (Fig. 3).
Fig. 2.

Cumulative incidence of the metachronous recurrence (H. pylori).
ESD = endoscopic submucosal dissection.
Fig. 3.

Cumulative incidence of the metachronous recurrence (age).
ESD = endoscopic submucosal dissection.
DISCUSSION
Our study shows that H. pylori could play an important role in developing metachronous cancer after ESD for EGC. Metachronous lesions occurred in 7 cases in the persistent group (38.8%) and 17 cases in the negative group (10.2%) during 61.1 months (median) (Table 1). There was little clinicopathological difference in the metachronous lesion group. However, there was substantial difference in both the H. pylori persistent group and the over 70-years-old group. These results suggest that the existence of H. pylori and old age increase the likelihood of metachronous lesion. Our study was based on previous studies that reported H. pylori infection plays an important role in the development of gastric cancer.
In Korea, endoscopic resection, including ESD, is the mainstream modality for EGC without metastasis (18). Recently, several studies reported that ESD for EGC treatment achieved good long-term outcomes and acceptable complication rates (7,19,20,21,22). In metachronous recurrence, 1 large population retrospective study reported the 5-year, 7-year, and 10-year cumulative incidence of metachronous gastric cancer were 9.5%, 13.1%, and 22.7%, retrospectively (23). This was distinguished from the cumulative incidence (6.1%) who underwent surgery (24). This discrepancy can be explained by the existence of tiny invisible lesions at the moment of ESD, the ability of ESD to offer an organ-sparing approach, a contribution to the better quality of life, and atrophic mucosa that can be a risk factor for cancer. It was reported that there was no difference in overall survival of patients who received the EMR on EGC, unlike the generation of metachronous lesion (25,26).
Gastric carcinogenesis is a complex and multifactorial process with many risk factors including non-ulcer dysplasia, active gastric ulcers, degree of mucosal atrophy, and H. pylori infection (27,28). The effect of H. pylori eradication on gastric mucosa is that neutrophillic infiltration disappears and infiltration with lymphocytes and plasma cells will be significantly reduced in the gastric mucosa. Then this retards the process of the precancerous lesion (29). The randomized trial reported that H. pylori eradication has a preventative effect to put the blocks on intestinal metaplasia and gastric atrophy (30). This can reduce the metachronous lesion occurrence from ESD patients after H. pylori eradication. However, moderate to severe atrophy or intestinal metaplasia may represent a ‘point of no return’ (31,32). Therefore, the prompt eradication of H. pylori reduces the process of atrophy, and this is helpful to prevent gastric cancer (33). The removal of H. pylori microorganism after ESD is necessary for the prevention of gastric metachronous. According to our study, H. pylori eradication decreased metachronous lesions, which is one of the topics in recent meta-analysis studies (34). The increase of metachronous lesions in patients over 70 years old was a meaningful result from our data. A study found that old age was an independent risk factor of metachrounous lesion, and H. pylori eradication on EGC after endoscopic resection did not increase metachronous lesions (14). In the other 10-year follow-up Japanese study, preventing gastric cancer by H. pylori eradication showed 100% effectiveness in patients under 40 years of age, and only 45% effectiveness in patients over 70 years of age (35). The occurrence of metachronous lesion in old age can be explained by the ‘point of no return’ idea (31). The H. pylori eradication from elderly patients, who proceeded to intestinal metaplasia and severe atrophy with a long-term H. pylori infection, could not prevent EGC. Other environmental factors, such as food, tobacco, and socioeconomic status based on age, are possible to generate metachronous lesions in elderly patients (36). Therefore, regular inspection is necessary for elderly patients, even if H. pylori is eradicated.
We think a prospective cohort study is needed for the exact multivariate analysis of both old age and H. pylori infection. Several limitations of this study require discussion. First, this was only a single center, retrospective study. This could induce selection bias for the generalization of the results. Second, the persistent H. pylori infection group was a small population. We had tried to determine H. pylori status through medical records, but had to enroll a small number of patients compared to the number of patients in the H. pylori negative group. This was due to the absence of examining a large number of patients with a H. pylori test. Finally, we did not analyze the background atrophy status and intestinal metaplasia, which might affect the metachronous recurrence and could be a confusing factor. Despite its limitations, this study is different from previous studies. First, we were covering only ESD from EGC. Second, we included metachronous lesions in all dysplasia as well as in malignancy.
In conclusion, the risk of metachronous recurrence after ESD for EGC was higher in the H. pylori persistent group than the negative group. Old age is an independent risk factor for patients after ESD for EGC. Therefore, a lot of clinicians should consider H. pylori eradication and regular surveillance, especially in patients with old age, after ESD for EGC.
Footnotes
DISCLOSURE: The authors have no potential conflicts of interest to disclose.
AUTHOR CONTRIBUTION: Conceptualization: Chung JW. Data curation: Jeong SH, Kwon KA, Kim YJ, Kim KO, Park DK. Formal analysis: Chung CS. Investigation: Chung CS. Writing - original draft: Chung CS, Woo HS. Writing - review & editing: Chung CS, Woo HS.
References
- 1.Tan VP, Wong BC. Gastric cancer chemoprevention: the current evidence. Gastroenterol Clin North Am. 2013;42:299–316. doi: 10.1016/j.gtc.2013.02.001. [DOI] [PubMed] [Google Scholar]
- 2.Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin. 2011;61:212–236. doi: 10.3322/caac.20121. [DOI] [PubMed] [Google Scholar]
- 3.Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet. 1984;1:1311–1315. doi: 10.1016/s0140-6736(84)91816-6. [DOI] [PubMed] [Google Scholar]
- 4.Marshall BJ, Armstrong JA, McGechie DB, Glancy RJ. Attempt to fulfil Koch’s postulates for pyloric Campylobacter. Med J Aust. 1985;142:436–439. doi: 10.5694/j.1326-5377.1985.tb113443.x. [DOI] [PubMed] [Google Scholar]
- 5.Schistosomes, liver flukes and Helicobacter pylori. IARC Working Group on the evaluation of carcinogenic risks to humans. Lyon, 7-14 June 1994. IARC Monogr Eval Carcinog Risks Hum. 1994;61:1–241. [PMC free article] [PubMed] [Google Scholar]
- 6.Huang JQ, Sridhar S, Chen Y, Hunt RH. Meta-analysis of the relationship between Helicobacter pylori seropositivity and gastric cancer. Gastroenterology. 1998;114:1169–1179. doi: 10.1016/s0016-5085(98)70422-6. [DOI] [PubMed] [Google Scholar]
- 7.Choi MK, Kim GH, Park DY, Song GA, Kim DU, Ryu DY, Lee BE, Cheong JH, Cho M. Long-term outcomes of endoscopic submucosal dissection for early gastric cancer: a single-center experience. Surg Endosc. 2013;27:4250–4258. doi: 10.1007/s00464-013-3030-4. [DOI] [PubMed] [Google Scholar]
- 8.Kim SG. Endoscopic treatment for early gastric cancer. J Gastric Cancer. 2011;11:146–154. doi: 10.5230/jgc.2011.11.3.146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nakagawa S, Asaka M, Kato M, Nakamura T, Kato C, Fujioka T, Tatsuta M, Keida K, Terao S, Takahashi S, et al. Helicobacter pylori eradication and metachronous gastric cancer after endoscopic mucosal resection of early gastric cancer. Aliment Pharmacol Ther. 2006;24:214–218. [Google Scholar]
- 10.Japanese Gastric Cancer Association Japanese gastric cancer treatment guidelines 2010 (ver. 3) Gastric Cancer. 2011;14:113–123. doi: 10.1007/s10120-011-0042-4. [DOI] [PubMed] [Google Scholar]
- 11.Shin SH. Jung da H, Kim JH, Chung HS, Park JC, Shin SK, Lee SK, Lee YC. Helicobacter pylori eradication prevents metachronous gastric neoplasms after endoscopic resection of gastric dysplasia. PLoS One. 2015;10:e0143257. doi: 10.1371/journal.pone.0143257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bae SE, Jung HY, Kang J, Park YS, Baek S, Jung JH, Choi JY, Kim MY, Ahn JY, Choi KS, et al. Effect of Helicobacter pylori eradication on metachronous recurrence after endoscopic resection of gastric neoplasm. Am J Gastroenterol. 2014;109:60–67. doi: 10.1038/ajg.2013.404. [DOI] [PubMed] [Google Scholar]
- 13.Kim YI, Choi IJ, Kook MC, Cho SJ, Lee JY, Kim CG, Ryu KW, Kim YW. The association between Helicobacter pylori status and incidence of metachronous gastric cancer after endoscopic resection of early gastric cancer. Helicobacter. 2014;19:194–201. doi: 10.1111/hel.12116. [DOI] [PubMed] [Google Scholar]
- 14.Maehata Y, Nakamura S, Fujisawa K, Esaki M, Moriyama T, Asano K, Fuyuno Y, Yamaguchi K, Egashira I, Kim H, et al. Long-term effect of Helicobacter pylori eradication on the development of metachronous gastric cancer after endoscopic resection of early gastric cancer. Gastrointest Endosc. 2012;75:39–46. doi: 10.1016/j.gie.2011.08.030. [DOI] [PubMed] [Google Scholar]
- 15.Choi J, Kim SG, Yoon H, Im JP, Kim JS, Kim WH, Jung HC. Eradication of Helicobacter pylori after endoscopic resection of gastric tumors does not reduce incidence of metachronous gastric carcinoma. Clin Gastroenterol Hepatol. 2014;12:793–800.e1. doi: 10.1016/j.cgh.2013.09.057. [DOI] [PubMed] [Google Scholar]
- 16.Japanese Gastric Cancer Association Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011;14:101–112. doi: 10.1007/s10120-011-0041-5. [DOI] [PubMed] [Google Scholar]
- 17.Kim SG, Jung HK, Lee HL, Jang JY, Lee H, Kim CG, Shin WG, Shin ES, Lee YC; Guidelines for the diagnosis and treatment of Helicobacter pylori infection in Korea, 2013 revised edition. Korean J Gastroenterol. 2013;62:3–26. doi: 10.4166/kjg.2013.62.1.3. [DOI] [PubMed] [Google Scholar]
- 18.Chung JW, Jung HY, Choi KD, Song HJ, Lee GH, Jang SJ, Park YS, Yook JH, Oh ST, Kim BS, et al. Extended indication of endoscopic resection for mucosal early gastric cancer: analysis of a single center experience. J Gastroenterol Hepatol. 2011;26:884–887. doi: 10.1111/j.1440-1746.2010.06611.x. [DOI] [PubMed] [Google Scholar]
- 19.Kosaka T, Endo M, Toya Y, Abiko Y, Kudara N, Inomata M, Chiba T, Takikawa Y, Suzuki K, Sugai T. Long-term outcomes of endoscopic submucosal dissection for early gastric cancer: a single-center retrospective study. Dig Endosc. 2014;26:183–191. doi: 10.1111/den.12099. [DOI] [PubMed] [Google Scholar]
- 20.Tanabe S, Ishido K, Higuchi K, Sasaki T, Katada C, Azuma M, Naruke A, Kim M, Koizumi W. Long-term outcomes of endoscopic submucosal dissection for early gastric cancer: a retrospective comparison with conventional endoscopic resection in a single center. Gastric Cancer. 2014;17:130–136. doi: 10.1007/s10120-013-0241-2. [DOI] [PubMed] [Google Scholar]
- 21.Oda I, Oyama T, Abe S, Ohnita K, Kosaka T, Hirasawa K, Ishido K, Nakagawa M, Takahashi S. Preliminary results of multicenter questionnaire study on long-term outcomes of curative endoscopic submucosal dissection for early gastric cancer. Dig Endosc. 2014;26:214–219. doi: 10.1111/den.12141. [DOI] [PubMed] [Google Scholar]
- 22.Kim JH, Lee JH, Chung JW, An J, Won IS, Lee JW, Ha M, Kim JS, Ahn HD, Park JC, et al. Risk factors for local recurrence of early gastric cancer after endoscopic submucosal dissection. Korean J Med. 2013;85:285–293. [Google Scholar]
- 23.Abe S, Oda I, Suzuki H, Nonaka S, Yoshinaga S, Nakajima T, Sekiguchi M, Mori G, Taniguchi H, Sekine S, et al. Long-term surveillance and treatment outcomes of metachronous gastric cancer occurring after curative endoscopic submucosal dissection. Endoscopy. 2015;47:1113–1118. doi: 10.1055/s-0034-1392484. [DOI] [PubMed] [Google Scholar]
- 24.Hosokawa O, Kaizaki Y, Watanabe K, Hattori M, Douden K, Hayashi H, Maeda S. Endoscopic surveillance for gastric remnant cancer after early cancer surgery. Endoscopy. 2002;34:469–473. doi: 10.1055/s-2002-32007. [DOI] [PubMed] [Google Scholar]
- 25.Choi KS, Jung HY, Choi KD, Lee GH, Song HJ, Kim DH, Lee JH, Kim MY, Kim BS, Oh ST, et al. EMR versus gastrectomy for intramucosal gastric cancer: comparison of long-term outcomes. Gastrointest Endosc. 2011;73:942–948. doi: 10.1016/j.gie.2010.12.032. [DOI] [PubMed] [Google Scholar]
- 26.Etoh T, Katai H, Fukagawa T, Sano T, Oda I, Gotoda T, Yoshimura K, Sasako M. Treatment of early gastric cancer in the elderly patient: results of EMR and gastrectomy at a national referral center in Japan. Gastrointest Endosc. 2005;62:868–871. doi: 10.1016/j.gie.2005.09.012. [DOI] [PubMed] [Google Scholar]
- 27.Hansson LE, Nyrén O, Hsing AW, Bergström R, Josefsson S, Chow WH, Fraumeni JF, Jr, Adami HO. The risk of stomach cancer in patients with gastric or duodenal ulcer disease. N Engl J Med. 1996;335:242–249. doi: 10.1056/NEJM199607253350404. [DOI] [PubMed] [Google Scholar]
- 28.Uemura N, Okamoto S, Yamamoto S, Matsumura N, Yamaguchi S, Yamakido M, Taniyama K, Sasaki N, Schlemper RJ. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med. 2001;345:784–789. doi: 10.1056/NEJMoa001999. [DOI] [PubMed] [Google Scholar]
- 29.Hojo M, Miwa H, Ohkusa T, Ohkura R, Kurosawa A, Sato N. Alteration of histological gastritis after cure of Helicobacter pylori infection. Aliment Pharmacol Ther. 2002;16:1923–1932. doi: 10.1046/j.1365-2036.2002.01346.x. [DOI] [PubMed] [Google Scholar]
- 30.Ley C, Mohar A, Guarner J, Herrera-Goepfert R, Figueroa LS, Halperin D, Johnstone I, Parsonnet J. Helicobacter pylori eradication and gastric preneoplastic conditions: a randomized, double-blind, placebo-controlled trial. Cancer Epidemiol Biomarkers Prev. 2004;13:4–10. doi: 10.1158/1055-9965.epi-03-0124. [DOI] [PubMed] [Google Scholar]
- 31.Wong BC, Lam SK, Wong WM, Chen JS, Zheng TT, Feng RE, Lai KC, Hu WH, Yuen ST, Leung SY, et al. Helicobacter pylori eradication to prevent gastric cancer in a high-risk region of China: a randomized controlled trial. JAMA. 2004;291:187–194. doi: 10.1001/jama.291.2.187. [DOI] [PubMed] [Google Scholar]
- 32.Chung JW, Hahm KB. Rejuvenation of atrophic gastritis in the elderly. J Gastroenterol Hepatol. 2010;25:434–435. doi: 10.1111/j.1440-1746.2010.06251.x. [DOI] [PubMed] [Google Scholar]
- 33.Wu CY, Kuo KN, Wu MS, Chen YJ, Wang CB, Lin JT. Early Helicobacter pylori eradication decreases risk of gastric cancer in patients with peptic ulcer disease. Gastroenterology. 2009;137:1641–1648.e1-2. doi: 10.1053/j.gastro.2009.07.060. [DOI] [PubMed] [Google Scholar]
- 34.Lee YC, Chiang TH, Chou CK, Tu YK, Liao WC, Wu MS, Graham DY. Association between Helicobacter pylori eradication and gastric cancer incidence: a systematic review and meta-analysis. Gastroenterology. 2016;150:1113–1124.e5. doi: 10.1053/j.gastro.2016.01.028. [DOI] [PubMed] [Google Scholar]
- 35.Asaka M, Kato M, Graham DY. Prevention of gastric cancer by Helicobacter pylori eradication. Intern Med. 2010;49:633–636. doi: 10.2169/internalmedicine.49.3470. [DOI] [PubMed] [Google Scholar]
- 36.Kushi LH, Byers T, Doyle C, Bandera EV, McCullough M, McTiernan A, Gansler T, Andrews KS, Thun MJ, American Cancer Society 2006 Nutrition and Physical Activity Guidelines Advisory Committee American Cancer Society guidelines on nutrition and physical activity for cancer prevention: reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J Clin. 2006;56:254–281. doi: 10.3322/canjclin.56.5.254. [DOI] [PubMed] [Google Scholar]