

Abstract
Background:
Violence against women is an emerging problem worldwide and more so in India. Considering its adverse effects on women's health, assessing the burden of violence in the community will help in planning services for the victims.
Objectives:
To determine the prevalence of domestic violence and to identify factors associated with domestic violence among married women in reproductive age group in rural Puducherry.
Materials and Methods:
A community-based cross-sectional study was carried out in a rural area of Puducherry, South India. Married women in reproductive age group were interviewed using structured pretested questionnaire. Domestic violence was assessed using 12 questions that were used in National Family Health Survey-3. Adjusted odds ratios (AORs) were calculated using multivariate logistic regression to identify factors associated with violence.
Results:
Of 310 study participants, 56.7% of them reported some form of domestic violence, 51.3% reported psychological violence, 40% reported physical violence, and 13.5% reported sexual violence. A statistically significant association was found between illiteracy of women and domestic violence (AOR: 4.3, 95% confidence interval: 1.1–15.7 P: 0.03). The other factors such as love marriage and nonregistration of marriage were significantly associated with violence.
Conclusion:
The prevalence of domestic violence was found to be high in this rural setting. Multisectoral response such as improving literacy, creating awareness regarding legal aid and screening the victims of violence at primary health centers, should be initiated to mitigate this public health issue.
Keywords: Domestic violence, physical violence, psychological violence, sexual violence
Introduction
In the recent times, violence against women is an emerging problem both in the developed and developing countries, with the World Health Organization (WHO) declaring domestic violence as a “public health epidemic.” According to the WHO, globally more than one-third of women are suffering physical and sexual violence, with a lifetime prevalence of violence ranging from 10% to 69% from different population surveys.[1,2] India falls in the higher end of this range with the third round of the National Family Health Survey (NFHS-3) reporting a burden of domestic violence as 37% among ever-married women in the reproductive age group.[3]
Domestic violence has substantial public health consequences, including both general health and reproductive health consequences such as chronic pain, injuries, fractures, disability, unwanted pregnancy and contraceptive use, rates of HIV, and other sexually-transmitted infections. Victims of domestic violence also suffer from psychological disturbances.[1] In addition, it has adverse effect on the economic progress of a country in the form of increased economic costs including loss of women's labor hours and increased health-care costs.[4]
Domestic violence against women has for a long time been considered only as a legal issue to be handled by the judicial system of the country. However, given its adverse effects on the women's health, there has been growing consensus that the health sector should also take initiatives to help these women. Women may not voluntarily report instances of violence due to the sensitive nature of the problem. Since domestic violence varies with the local social norms and literacy level of women, it is important to assess the problem of domestic violence in the given geographical region for initiating supportive measures.[5] The studies including the NFHS-3 have reported varied levels of domestic violence in different states and communities.[3] Hence, this study was carried out to determine the prevalence of domestic violence and identify factors associated with domestic violence in a selected rural area of South India.
Materials and Methods
A community-based cross-sectional study was carried out among the married women in the Ramanathapuram village, of Puducherry from January 2015 to February 2015. The majority of the villagers are engaged in agriculture as daily wage laborers. This village is one of the four villages catered by a Rural Training and Health Centre of a tertiary care teaching hospital in Puducherry. The health center provides primary health-care services to a population of approximately 9500 people.
The study included all married women in the age group of 18–49 years residing in the village, who got married at least 1 year ago and were living with their husbands. Based on the prevalence of domestic violence of 45.1% in Tamil Nadu,[6] assuming the absolute precision 8%, alpha error 5%, and design effect of 2, the required sample size was estimated to be 298. From the enumeration records maintained at the health center, it was estimated that there were 350 eligible women in the village. Considering nonresponse rate, it was decided to cover all houses in the village. All eligible women in a household were included in the study after obtaining written informed consent. The houses that were either locked or those in which the eligible woman was not present at the time of the visit, were noted down and were revisited at least three times. If the woman could not be contacted at the end of the three visits, then she was excluded from the study.
The women were interviewed with a pretested structured questionnaire adapted from the women's questionnaire used in NFHS-3, after ensuring adequate privacy. The questionnaire consisted of sociodemographic characteristics of the women and questions to ascertain whether the respondent had experienced domestic violence. There were seven, three and two questions to ascertain where the woman had experienced physical, psychological, or sexual violence, respectively. An affirmative response to any of these questions was considered as an indication of domestic violence irrespective of the type of violence.
The study protocol was reviewed and approved by the Institute Ethics Committee of the Tertiary Care Teaching Hospital. Data entry was done using EpiData software (version 3.1, EpiData Association, Odense, Denmark). Data analysis was done using EpiData software version 2.2.2.182 and SPSS (version 20.0, IBM, USA). To identify factors associated with domestic violence, bivariate analysis was done for each factor and the presence of domestic violence. Those factors which were found to have a statistically significant association at P < 0.10 were included in the multivariate logistic regression. Adjusted odds ratios (AORs) and 95% confidence interval (CI) were computed for the multivariate model, and statistical significance was considered if P < 0.05.
Results
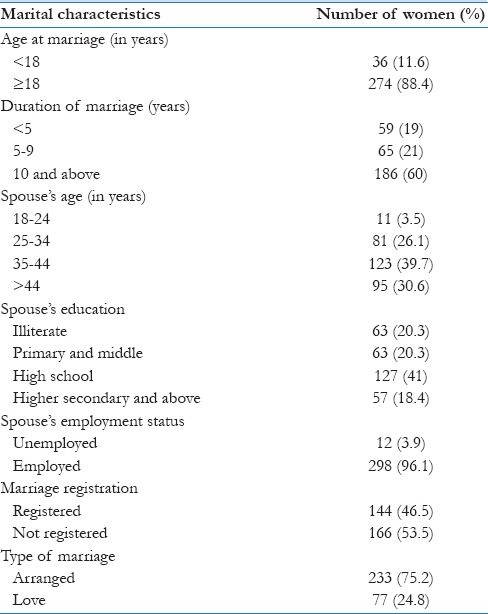
A total of 310 eligible women were included, and the mean (standard deviation [SD]) age was 33.9 (7.5) years. The sociodemographic and marital characteristics of the respondents are shown in Tables 1 and 2. About two-fifths of the respondents were in age group of 25–34 years, and nearly one-fourth had not received any formal education. More than half (58%) were homemakers. The mean (SD) age at marriage was 20.8 (3.6) years. One-fifth of the respondents’ husbands was illiterate and a vast majority of the husbands (96%) were employed. More than half (56%) of the women belonged to joint families.
Table 1.
Distribution of sociodemographic characteristics of the married women in reproductive age group in Ramanathapuram, Puducherry (n=310)
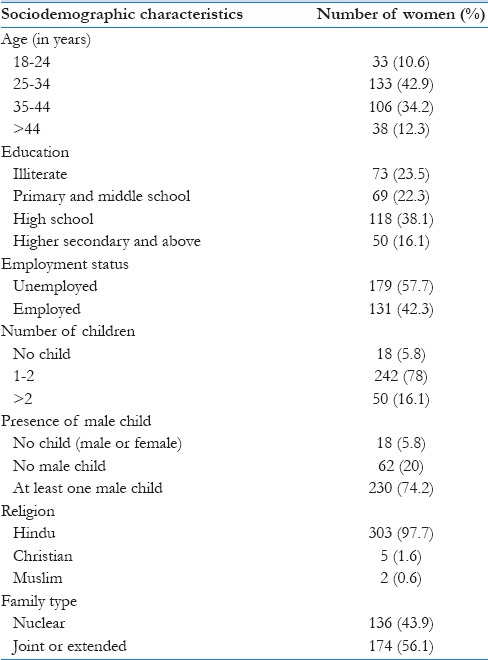
Table 2.
Distribution of marital characteristics of the married women in reproductive age group in Ramanathapuram, Puducherry (n=310)
Out of the total respondents, 176 (56.7%) women had experienced some form of domestic violence. Psychological violence was the predominant form reported by 159 (51.3%) women followed by physical violence (40%) and sexual violence (13.5%). Among those 176 women who had suffered violence, 90.3%, 72.5%, and 23.7% had suffered from psychological, physical and sexual violence, respectively. Out of the 176 women who reported domestic violence, 113 (64.2%) women reported that husband was the common perpetrator, followed by mother in law (35.2%).
Among the victims of physical violence (n = 124), 56 (45.1%) respondents reported or had cuts, bruises, or ache as a result of the violence. Grievous injuries such as eye injuries, sprain, and dislocations were reported by 31 (25%) women. Deep wounds, broken teeth, or bone, serious injuries were reported by 18 (14.5%) women.
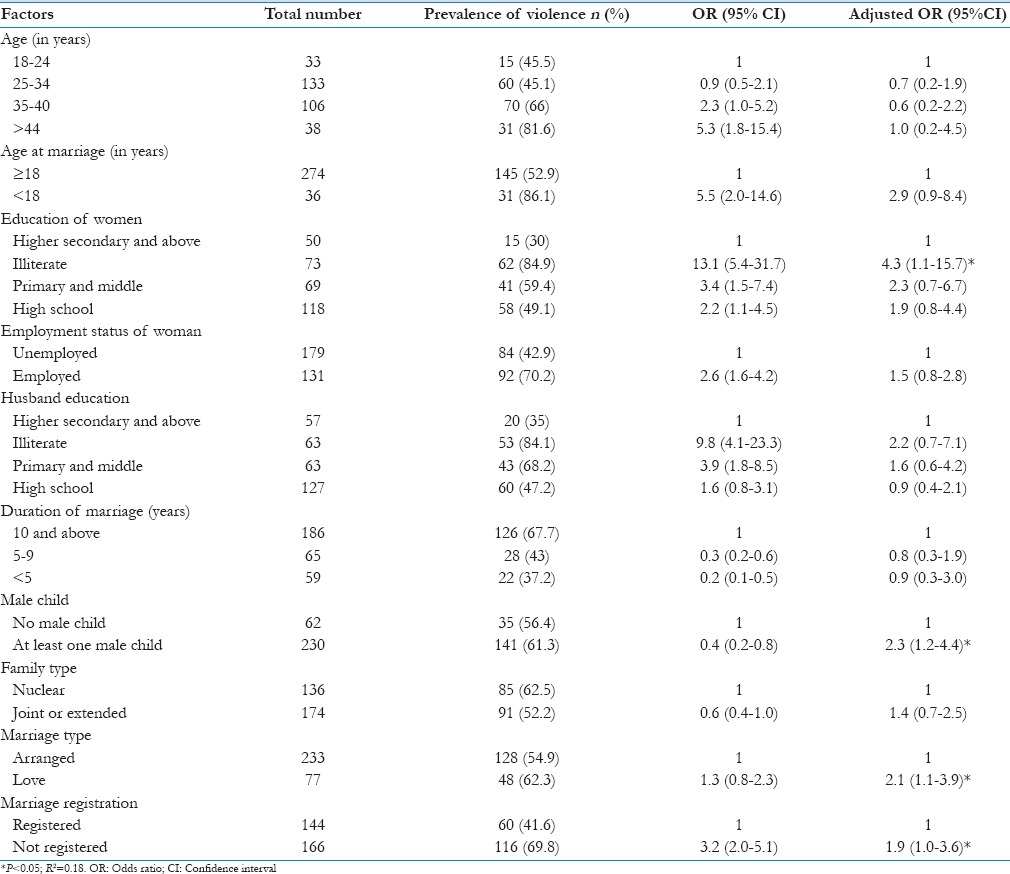
Factors associated with domestic violence in bivariate analysis are shown in Table 3. Age of the respondent, age at marriage <18 years, women's educational status, employment status, husband's education, duration of the marriage, having male child, marriage registration, and type of marriage (love or arranged) were associated with domestic violence. In multivariate analysis, a significant association was found between illiteracy of women and domestic violence (AOR: 4.3, 95% CI: 1.2–15.7, P: 0.03). Love marriage (AOR 2.1, 95% CI: 1.1–3.9, P = 0.02) and no registration of marriage (AOR 1.9, 95% CI: 1.0–3.6, P = 0.04) were independently associated with domestic violence.
Table 3.
Factors associated with domestic violence among married women aged 18-49 years in Ramanathapuram, Puducherry, 2015 (n=310)
Discussion
In this study, in a rural area of South India, it was found that more than half of the married women were victims of domestic violence, and the husband was the perpetrator in most of the cases. Illiterate women were at higher risk of violence than literate women.
The overall prevalence of domestic violence (56.7%) found in our study was similar to the prevalence reported previously in rural Puducherry and Eastern India.[7,8,9] However, NFHS-3[3] and a multicentric study[10] have reported a prevalence of 37%, and 39%, respectively, much lesser than the present study. Exact reasons for this difference are not known.
Psychological abuse was the most common form of abuse with a prevalence of 51.3%, which is similar to other studies from North Bengal (54.5%)[11] and Eastern India (52).[9] The present study has found the prevalence of physical violence as 40% which was similar to the prevalence reported in NFHS-3 for the state of Tamil Nadu[6] (41.9%). However, this prevalence was higher than the national average of 29.7%. The different sociocultural norms such as acceptability of physical violence at the hands of husbands could be the reason for these differences. This study reported that the prevalence of sexual violence was 13.5%. Similar prevalence estimates were reported in NFHS-3[3] and the studies from the state of Maharashtra[12] as well.
According to this study, the husbands were the usual perpetrator of violence (64.2%) which is similar to NFHS-3 and other studies from different states of India.[3,8,13,14,15] Most of the previous studies have reported that illiteracy among the women was associated with domestic violence, and our study found a similar association.[3,16,17] However, husband's education was not found significantly associated with violence.
One interesting finding of the study is that those women who had love marriage were significantly at higher risk of getting abused than who had arranged marriage. Another study from South India has reported similar association.[18] Among women who had love marriage, this may be due to lack of family support at the times of conflict. In rural areas, love marriages mostly imply that the couple had eloped which may have led to a feeling of guilt on the part of women and in turn, become a factor to put up with prolonged domestic violence.
Another finding was the significantly higher prevalence of violence among women with nonregistered marriages.
The study has few implications. First, identification of the domestic victims and offering them help is important. These measures should be implemented at the level of primary health-care centers. The primary care physicians are usually the first points of contact of women with the health system. Being a sensitive issue, women may not voluntarily reveal that they have been victimized. Innovative approaches such as opportunistic screening for domestic violence by physicians at health facilities with a screening tool will be useful.[19] Community level workers such as ASHA and Anganwadi workers can be involved in targeted screening of illiterate, married women since they routinely interact with the women for the provision of services and have an existing rapport with them. The multidisciplinary team in primary health centers should be upgraded to include mental health professionals as well as professional social workers to address this issue effectively. Although the National Mental Health Programme addresses the issue of capacity building at primary level, its implementation has not been universal.[20] Second, awareness about legal options and other helplines should be generated among public. The community in general and married women, in particular, should be made aware of the Domestic Violence Act, 2005 to protect the victim and prevent the violence. Women self-help groups in the rural areas may be involved in these programs. Helplines should be initiated for women at every primary health-care center. Third, improving overall education of girl child will help in empowering against the domestic violence. In addition, the male partners should be educated to instill values such as respect for women at an early age. Introducing gender sensitization at an earlier age through schools is likely to have a positive effect on the men in the long-term. The focus of services should not be restricted to woman alone and should involve family members as well in to help them to gain the right perception of domestic violence. Fourth, given the significant association between the registration of marriages and less prevalence of domestic violence, stricter marriage laws will help mitigate this public health issue.
The study has a few strengths. We were able to interview more than 90% of the eligible women in the study area. We used a validated questionnaire for assessing domestic violence and definitions similar to the one used in the nationwide NFHS-3 survey which allows for comparisons with other studies. There are few limitations. As domestic violence is a sensitive issue, under-reporting due to fear of stigma cannot be ruled out, though interviews were conducted with privacy and ensuring confidentiality. The study was conducted in a small geographical area, and hence, the study findings may not be generalizable to other rural areas.
Conclusion
More than half of the married women in this rural study setting have experienced one or other form of violence. Long-term measures are needed to empower women and educate men to curb this menace. Taking the issue only as a public health problem will be a futile attempt unless a multifaceted approach using legal, social sciences, and mental health systems is employed to check it.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.World Health Organisation. World Report on Violence and Health. WHO. [Last cited on 2016 May 23]. Available from: http://www.who.int/violence_injury_prevention/violence/world_report/en/
- 2.World Health Organisation. Global and Regional Estimates of Violence Against Women. WHO. [Last cited on 2016 May 23]. Available from: http://www.who.int/reproductivehealth/publications/violence/9789241564625/en/
- 3.International Institute for Population Sciences (IIPS), Macro International. National Family Health Survey (NFHS-3), 2005-2006: India. I. Mumbai: International Institute for Population Sciences; 2007. [Google Scholar]
- 4.Pandey MK, Singh P, Yadav RA. Domestic Violence and Women's Health in India: Evidence from Health Survey. University Library of Munich, Germany. 2008. [Last cited on 2016 May 23]. Available from: http://www.core.ac.uk/download/pdf/12020342.pdf .
- 5.United Nations Population Fund. A Practical Approach to Gender-based Violence. UNFPA. [Last cited on 2016 May 23]. Available from: http://www.unfpa.org/resources/practical-approach-gender-based-violence .
- 6.International Institute for Population Sciences (IIPS), Macro International. National Family Health Survey (NFHS-3), India, 2005-2006: Tamil Nadu. Mumbai: International Institute for Population Sciences; 2008. [Google Scholar]
- 7.Rajini S, Kamesh C, Senthil S. Prevalence of domestic violence and health seeking behavior among women in rural community of puducherry – A cross sectional study. Int J Curr Res Rev. 2014;6:20–3. [Google Scholar]
- 8.Vasudevan K, Vasudevan P. Epidemiological study of domestic violence among married women in a rural area of Pondicherry. Int J Curr Res. 2013;5:3480–2. [Google Scholar]
- 9.Babu BV, Kar SK. Domestic violence against women in eastern India: A population-based study on prevalence and related issues. BMC Public Health. 2009;9:129. doi: 10.1186/1471-2458-9-129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mahapatro M, Gupta R, Gupta V. The risk factor of domestic violence in India. Indian J Community Med. 2012;37:153–7. doi: 10.4103/0970-0218.99912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ray K, Chakraborty M, Roy H, Gupta S. Violence against women: Evidence from a cross sectional study in urban area of North Bengal. Al Ameen J Med Sci. 2012;5:157–64. [Google Scholar]
- 12.Parikh D, Anjenaya S. A cross sectional study of domestic violence in married women in Asudgaon village of Raigad District. Int J Recent Trends Sci Technol. 2013;6:81–8. [Google Scholar]
- 13.Sinha A, Mallik S, Sanyal D, Dasgupta S, Pal D, Mukherjee A. Domestic violence among ever married women of reproductive age group in a slum area of Kolkata. Indian J Public Health. 2012;56:31–6. doi: 10.4103/0019-557X.96955. [DOI] [PubMed] [Google Scholar]
- 14.Kaur S, Patidar AB, Sharma S. Domestic violence and its contributory factors among married women in selected slums of Ludhiana, Punjab. Nurs Midwifery Res J. 2014;10:30–5. [Google Scholar]
- 15.Sarkar M. A study on domestic violence against adult and adolescent females in a rural area of west bengal. Indian J Community Med. 2010;35:311–5. doi: 10.4103/0970-0218.66881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kamat U, Ferreira AM, Motghare DD, Kamat N, Pinto NR. A cross-sectional study of physical spousal violence against women in Goa. Health Line. 2010;1:34–40. [Google Scholar]
- 17.Mishra A, Patne S, Tiwari R, Srivastava DK, Gour N, Bansal M. A cross-sectional study to find out the prevalence of different types of domestic violence in Gwalior city and to identify the various risk and protective factors for domestic violence. Indian J Community Med. 2014;39:21–5. doi: 10.4103/0970-0218.126348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rocca CH, Rathod S, Falle T, Pande RP, Krishnan S. Challenging assumptions about women's empowerment: Social and economic resources and domestic violence among young married women in urban South India. Int J Epidemiol. 2009;38:577–85. doi: 10.1093/ije/dyn226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Nair D, Majumdar A, Ramakrishnan J, Mahalakshmy T, Sahu SK. Feasibility of routine screening for domestic violence among women attending an urban health center in Puducherry, India. Int J Med Sci Public Health. 2015;4:1191–6. [Google Scholar]
- 20.Roy S, Rasheed N. The National Mental Health Programme of India. Int J Curr Med Appl Sci. 2015;7:7–15. [Google Scholar]