

Abstract
Myasthenia gravis (MG) is an autoimmune neuromuscular junction disorder which is characterized by fluctuating muscle fatigue. However, the association of MG with nemaline myopathy is rarely reported.
Here we report a case of MG coexisting with adult-onset nemaline myopathy. A 55-year-old man endured fluctuating muscle weakness with positive acetylcholine receptor and titin antibodies. After the patient was administrated cholinergic drugs and immunosuppression, the muscle weakness of the patient had mildly been alleviated. Electromyography showed a progressive decrement in the amplitude of muscle action potential at low frequency. Muscle biopsy showed numerous nemalines in the muscle fibers.
This is the first reported case of nemalines present in the muscle fibers of adult patient with MG. The pathogenesis of nemaline may be related to titin antibody in adult-onset nemaline myopathy with MG.
INTRODUCTION
Myasthenia gravis (MG) is an autoimmune neuromuscular junction disorder which is characterized by fluctuating muscle fatigue and is frequently associated with other autoimmune diseases.1 Recently, MG has been reported to coexist with several other diseases.2,3 However, up to now, there is no description of the association of MG with nemaline myopathy. Here we report a case of MG coexisting with adult-onset nemaline myopathy.
CASE REPORT
The patient is a 55-year-old man. He had breathing difficulty and persistent bilateral ptosis since June 2007. Neostigmine test was positive. Laboratory tests revealed positive acetylcholine receptor (AChR) antibody. Computerized tomography (CT) of the chest revealed a retrosternal ovoid nodule with mild enhancement. These symptoms supported the diagnosis as MG. After treatment with pyridostigmine, prednisome, and azathioprine, dysphasia, dysarthria, and ptosis were mildly alleviated. Recently, the patient presented exacerbating weakness in proximal muscles of the limbs with obvious muscle fasciculation. He complained of chest distress and persistent ache in the left chest. The muscle strength of neck extensor was 4/5 (medical research council scale, grades 0–5) grade. Muscle fatigue was found in orbicularis oculi, bulb muscles, and proximal muscles of limbs. No muscle atrophy and muscle cramps were observed. Muscle fasciculation was observed in both quadriceps femoris. The patient presented mildly symmetrical hyperreflexia with positive Rossolimo signs.
The patient underwent a muscle biopsy in left biceps brachii. Modified gomori trichrome staining revealed numerous red rod-shaped bodies accumulated in 7% muscle fibers (Figure 1A). No inflammatory cells were observed in endomysial and perivascular areas. Immunostaining showed that the rod-shaped bodies had alpha-actinin positive reaction (Figure 1B). In contrast, actin and titin-positive grains were not found in the rod-shaped bodies. Ultrastructural examination revealed that the muscle fibers contained many disorderly arrays of osmiophilic oval or rectangular structures with 2 ends linking to sarcomere, which had the same electron density as Z-band. These structures mainly scattered in the sarcoplasm, occasionally distributed under subsarcolemma (Figure 2). No intranuclear rod bodies were observed.
FIGURE 1.
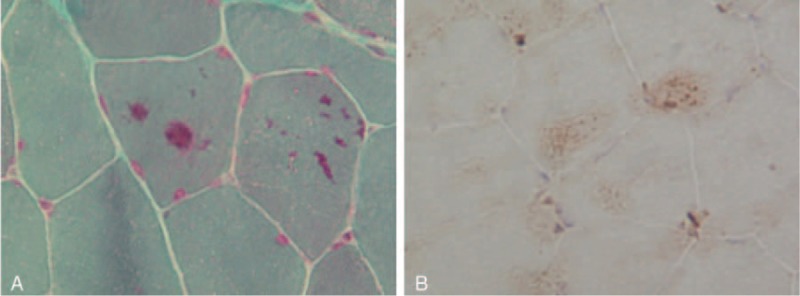
(A) Modified gomori trichrome staining indicated the red nemalines scatter in muscle fibers. (B) Immunostaining indicated that the nemalines in muscle fibers were alpha-actinin positive. Magnification: 200×.
FIGURE 2.
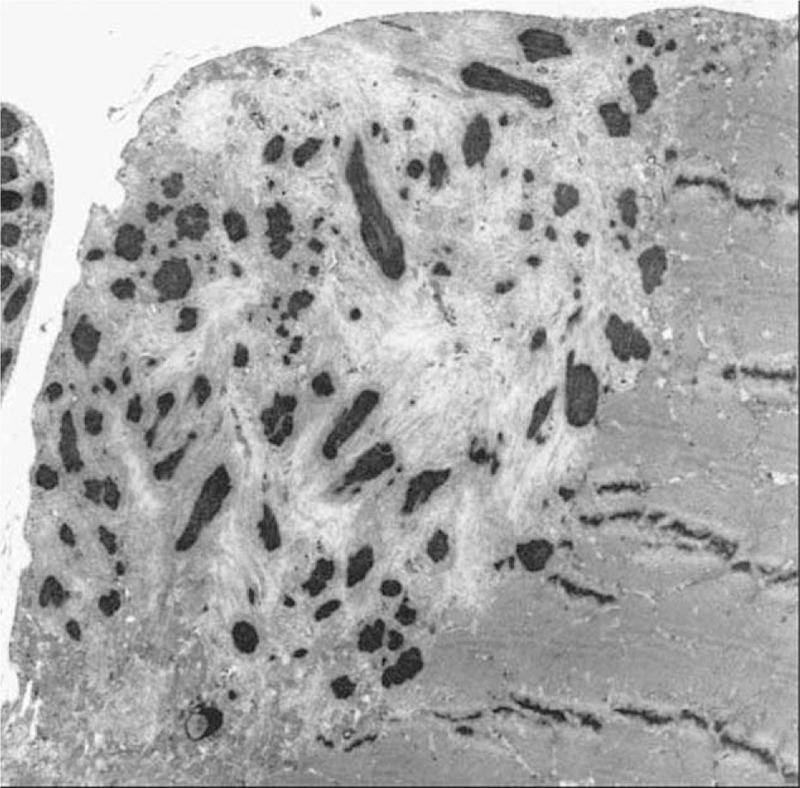
Electron microscopy showed that muscle fibers contained many arrays of osmiophilic oval or rectangular structures. Magnification: 5000×.
The written informed consent for the case report was obtained from this patient, and the consent procedure was approved by the Ethics Committee of Nanchang University.
DISCUSSION
The simultaneous occurrence of both thymomatous MG and adult-onset nemaline myopathy is extremely rare. It is unclear whether MG is the cause or coincidence to adult-onset nemaline myopathy in our patient. Adult-onset nemaline myopathy has been described either as an isolated entity or as concomitance in association with virus infections or autoimmune diseases.4 Therefore, we speculate that adult-onset nemaline myopathy may be caused by abnormally immunological etiology. Inflammatory cells in biopsy specimens and improvement of symptoms after immunosuppressive therapies support our speculation.5 Our patient had obvious autoimmune disturbance, such as positive AchR antibody, acetylcholine esterase antibody, and titin body.
Nemaline is derived from the Z disc of striated muscle and composed of actin and alpha-actinin, but the detailed mechanisms by which actin and alpha-actinin form disorderly arrays are unclear.6 Anti-titin antibody is a sensitive marker of thymoma associated with MG in elder patients.7 Although we were unable to confirm thymoma in our patient due to his refusal to thymus resection, a mildly enhanced ovoid nodule at the posterior of sternum was found through CT scanning of chest. In addition, we found a high level of titin antibody in his serum. Thus we speculate that the pathological process in this case is as follows: abnormal autoimmune is associated with MG at the early stage; at the late stage, high level of anti-titin antibody destructs the sarcomere components, resulting in the formation of nemaline in affected fibers. This process corresponds to the worsening of muscle strength in our patient. However, nemaline myopathy is known to be caused by the mutations in at least 6 genes including ACTA1, CFL2, NEB, TNNT1, TPM2, and TPM3. Further studies are needed to characterize the mutations responsible for nemaline myopathy in this case.
In summary, we present the first case of MG coexisting with adult-onset nemaline myopathy. The clinical process reminds us to differentiate myasthenia crisis from adult-onset nemaline myopathy.
Footnotes
Abbreviations: AchR = acetylcholine receptor, CT = computerized tomography, MG = myasthenia gravis.
LC and YW contributed equally.
Conflicts of interest: All authors report no conflicts of interest.
REFERENCES
- 1.Raica M, Cimpean AM, Ribatti D. Myasthenia gravis and the thymus gland. A historical review. Clin Exp Med 2008; 8:61–64. [DOI] [PubMed] [Google Scholar]
- 2.Tsai Y, Lin Y, Chen C, et al. Thymoma associated with myasthenia gravis and Sjögren syndrome. West Indian Med J 2013; 62:264–265. [DOI] [PubMed] [Google Scholar]
- 3.Miyazaki Y, Hirayama M, Watanabe H, et al. Paraneoplastic encephalitis associated with myasthenia gravis and malignant thymoma. J Clin Neurosci 2012; 19:336–338. [DOI] [PubMed] [Google Scholar]
- 4.Gyure KA, Prayson RA, Estes ML. Adult-onset nemaline myopathy: a case report and review of the literature. Arch Pathol Lab Med 1997; 121:1210–1213. [PubMed] [Google Scholar]
- 5.Chahin N, Selcen D, Engel AG. Sporadic late onset nemaline myopathy. Neurology 2005; 65:1158–1164. [DOI] [PubMed] [Google Scholar]
- 6.Wallgren-Pettersson C, Jasani B, Newman GR, et al. Alpha-actinin in nemaline bodies in congenital nemaline myopathy: immunological confirmation by light and electron microscopy. Neuromuscul Disord 1995; 5:93–104. [DOI] [PubMed] [Google Scholar]
- 7.Yamamoto AM, Gajdos P, Eymard B, et al. Anti-titin antibodies in myasthenia gravis: tight association with thymoma and heterogeneity of nonthymoma patients. Arch Neurol 2001; 58:885–890. [DOI] [PubMed] [Google Scholar]