

Abstract
Background:
Pregnancy induced hypertension (PIH) is a state of extremely increased oxidative stress. Hence, research and test of role and significance of oxidative stress in hypertensive disturbance in pregnancy is very important.
Aim:
Aims of this research were to determine a level of thiobarbituric acid reactive substance (TBARS) as oxidative stress marker in blood of pregnant woman with pregnancy induced hypertension and to analyze correlation of TBARS values with blood pressure values in pregnancy induced hypertensive pregnant women.
Patients and methods:
Research has been performed at the Clinic of Gynecology and Obstetrics, University Clinical Centre in the Republic of Srpska. It covered 100 pregnant women with hypertension and 100 healthy pregnant women of gestation period from 28 to 40 weeks. Level of TBARS is determined as an equivalent of malondialdehyde standard, in accordance with recommendations by producer (Oxi Select TBARS Analisa Kit).
Results:
Pregnancy induced hypertension is a state of extremely increased oxidative stress. All pregnant women experiencing hypertension had increased TBARS values in medium value interval over 20 µmol, 66%, whereas in group of healthy pregnant women, only 1% experienced increased TBARS value. Pregnant women with difficult preeclampsia (32%) had high TBARS values, over 40 µmol, and with mild PIH, only 4.9% pregnant women.
Conclusion:
Pregnant women with pregnancy induced hypertension have extremely increased degree of oxidative stress and lipid peroxidation. TBARS values are in positive correlation with blood pressure values, respectively the highest TBARS value were present in pregnant women with the highest blood pressure values.
Keywords: pregnancy induced hypertension, oxidative stress, TBARS
1. INTRODUCTION
Pregnancy induced hypertension (PIH) is one of the most frequent and most difficult illnesses in pregnancy, which jeopardizes both mother and fetus. Frequency is about 10% with significant variations in certain parts of the world depending on diagnostic criteria (1). Preeclampsia makes up to70% of all hypertensions of the pregnancy course (2-4). About 10% of cases occur at about 34 gestation week, and in about 25% cases there is a severe disorder of pregnant woman’s vital organs function. In the most developed countries of the world, preeclampsia is responsible for over 15% preterm deliveries and about 18% maternal deaths (5, 6, 7, 9). General vasospasm with hypovolemia and hypoperfusion of organs and utero placental hypoperfusions consequence is pathophysiological dominant (9, 10). Nowadays, role of oxidative stress in PIH etiology is being researched, and acquired results show that oxidative stress could have a significant role in generation of preeclampsia since it starts damage of endothelium of placenta vascularization and immune response (12-15). Normal pregnancy is considered to be a state where oxidative stress increases a bit, but there is no increase in, so called, free radicals. Recently, a great attention is being paid to lipid peroxidation, which actually is oxidative damage of lipids and increased creation of lipid peroxides, whose final product is malondialdehyde (MDA). Nowadays, malondialdehyde (MDA) is used in many expert researches as oxidative stress marker, i.e. for assessment of lipid peroxidation (16-17). Oxidative stress marker, which bonds to malondialdehyde fast and strongly is Thiobarbituric Acid Reactive Substance (TBARS). In accordance with the current findings from the literature, it is presumed that pregnancy induced hypertension (PIH) is a state of extremely increased oxidative stress. Hence, research and test of role and significance of oxidative stress in hypertensive disturbance in pregnancy is very important (18). This research is actually directed to the analyses of oxidative stress existence, oxidative stress degree, i.e. lipid peroxidation as well as pregnancy induced hypertension and correlation of those parameters with blood pressure values.
2. AIMS
Aims of this research were to determine a level of oxidative stress marker (TBARS) in blood of pregnant woman with pregnancy induced hypertension and to analyze correlation of TBARS values with blood pressure values in pregnancy induced hypertensive pregnant women.
3. PATIENTS AND METHODS
Research has been performed at the Clinic of Gynecology and Obstetrics of University Clinical Centre in the Republic of Srpska pursuant to current standards and regulations of the Ethics Committee. 200 pregnant women with single pregnancy, gestation from 28 to 40 weeks with regular medical documentation were tested. Based on clinical laboratory and ultrasound criteria, we divided pregnant women in to two groups: test group of 100 pregnant women with hypertension and control group of 100 pregnant women without hypertension.
While hospitalized, all pregnant women were treated in the same way, oral therapies, Aldomet tablets dosage 500 mg to 2–2.5 g, depending on blood pressure values. With difficult hypertension and preeclampsia, apart from mentioned therapy, Cordipin tablets dosage from 10 mg to 60 mg were administered. Half-salty nutrition regime, high-protein food, strictly resting and oxygen therapy were advised. Blood pressure (BP) was measured every 4 hours, auscultatory method with mercury sphygmomanometer. Mild hypertension is considered to be the level of BP equal or higher than 140/90 mmHg, and difficult hypertension is considered to be the level of BP equal or higher than 160/110 mmHg. Selection of pregnant women of control group was similar to pregnant women of test group in age and gestation period. All pregnant women of control and test group were analyzed for blood to oxidative stress biomarker, thiobarbituric acid reactive substance (TBARS), by spectrophotometric method based on concentration of malondialdehyde, product of lipid peroxidation. Thiobarbituric acid reactive substance is as very sensitive method for quantitative determination of lipid peroxidation degree, being key indicator of oxidative stress. Principle of this screening method is that two molecules of thiobarbituric acid reactive substance react with malondialdehyde in order to create a complex, which is determined by spectrophotometry. At the ward, five milliliters of vein blood from cubital vein was taken out and put into a sterile tube. Level of TBARS is determined as an equivalent of malondialdehyde standard, in accordance with recommendations by producer (Oxi Select TBARS Analisa Kit (MDA quantification), and result was acquired by spectrophotometry at 532 nm. Analyses protocol was: we added 100 µl of sample or MDA standard. Each tube was added 100 µl of Sodium dodecyl sulfate (SDS) solution for analyses (in samples and MDA standard), well mixed. Samples were incubated for 5 minutes in ambient temperature. We added 250 µl of TBA reagent in each sample and standard. Each tube was sealed and incubated in 95 ºC, for 45-60 minutes. Tubes were taken out and chilled to ambient temperature in ice bath. All tubes with samples were centrifuged on 3000 revolutions for 10 minutes. Supernatant for further analyses was set aside. Spectrophotometric measuring: 200 µl of MDA standard and samples were transferred to tubes and absorption was read on 532 nm.
We were governed by sensitiveness of test recommended by producers and based on acquired minimum and maximum values. Acquired TBARS values were divided into intervals for the purpose of detailed analysis and comparison low values interval up to 20 µmol, medium values interval from 20 to 40 µmol and high values interval of TBARS over 40 µmol. Results were analyzed and presented through descriptive statistics and adequate statistical tests in analytic-statistic software kit Statistical Package for the Social Sciences (SPSS). In normal division, we used t – test of independent samples, and in cases where basic group significantly deviated from normal division, we applied Mann-Whitney U-test. We used Chi-squared (χ2) test and Fisher test with appropriate importance level of p < 0.05.
4. RESULTS
Research results of test group, pregnant women with pregnancy induced hypertension and control group, which were healthy pregnant women, were analyzed in detail in accordance with age in the first place, parity and delivery gestation (Table 1).
Table 1.
Pregnancy and delivery parameters in all pregnant women

Analyzing age of examinees, we got a high statistic difference in pregnant women’s age, p=0.005, pregnant women with hypertension were older compared to pregnant women in control group. Pregnant women with PIH delivered in significantly lower gestation compared to control group; Fisher test applied, we got high statistic difference p=0.000. In gestation from 28-33+6 weeks, there were15 pregnant women in test group, pregnant women with PIH, whereas only one pregnant women in control group. Referring to parity, there is no statistic significant difference of pregnant women with PIH and healthy pregnant women, number of primiparas and multipara were equal in both groups. The highest measured value of systolic pressure amounted to 220 mmHg in test group, whereas diastolic amounted to 160 mmHg. 59% pregnant women experienced difficult hypertension (PIH), whereas 41% of them experienced mild PIH. Values of systolic and diastolic pressure of control group was maximum of 140/90 mmHg.
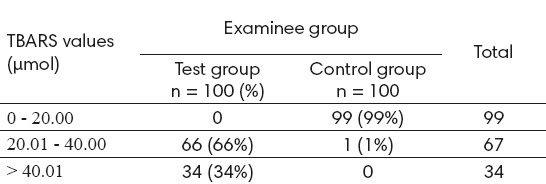
In order to view clinical applications of TBARS, being oxidative stress marker, we analyzed acquired TBARS values divided into intervals: low values interval up to 20 µmol, medium values interval from 20 to 40 µmol and high values interval of TBARS over 40 µmol and compared them with test and control group.
Table 2 shows that pregnant women of test group, pregnant women with PIH, TBARS mean value from 20 to 40 µmol, was experienced by 66% pregnant women, TBARS high value over 40 µmol was experienced by 34% pregnant women with PIH. There was no pregnant woman in test group in the group of low value interval of TBARS up to 20 µmol. Low TBARS values up to 20 µmol in the control group were found in 99% healthy pregnant women.
Table 2.
TBARS values in all pregnant women.
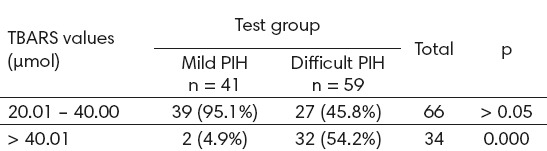
We analyzed TBARS values in high and medium intervals with pregnant women of test group with mild and difficult PIH and acquired the following results. Table 3 shows that we acquired a high statistic significant difference in TBARS values in TBARS high values group over 40 µmol with pregnant women with PIH, applying Fisher test, p = 0.000.
Table 3.
TBARS values with pregnancy induced hypertensive pregnant women
5. DISCUSSION
Former researches dealing with problem of oxidative stress indicate that pregnancy is a state of physiological, slightly increased oxidative stress in comparison to healthy non-pregnant women. Oxidative stress could have a significant role in generation of pregnancy induced hypertension (PIH), since it starts damage of endothelium of placenta vascularization and immune response (19, 20). Bhale DV et al. also concluded in their study that pregnancy induced hypertension (PIH) is a state of extreme increase of oxidative stress and lipid peroxidation (21).
In our study, we proved the increased TBARS level as oxidative stress marker in pregnant women with PIH, too. Acquired results show that low TBARS values up to 20 µmol were found with 99% pregnant women of control group, and interval of TBARS medium values was experienced by only 1% pregnant women in that group. In test group, low TBARS values were not experienced by any pregnant women, interval of medium TBARS values from 20 µmol to 40 µmol were experienced by 66% pregnant women, whereas interval of high TBARS values over 40 µmol were experienced by 34% pregnant women with PIH. Based on our acquired results, that means that pregnant women of test group had extremely increased TBARS values in comparison to control group. Our results in this research show that pregnancy induced hypertension is a state of extremely increased oxidative stress which corresponds to the other studies, too (22, 23, 24).
Kurlak LO et al. put forward a positive correlation between oxidative stress markers in hypertensive states of pregnancy (25). In our study, we analyzed values of TBARS oxidative stress marker according to groups in relation to blood pressure values. Statistical analyses resulted in high statistic difference in TBARS values in pregnant women with difficult PIH and mild PIH. Out of 34 pregnant women with difficult PIH, 32 of them experienced high TBARS values over 40 µmol, whereas in group with mild PIH, high TBARS values were experienced in only 2 pregnant women, which is high statistic importance. Our results showed that there was positive correlation between blood pressure value and TBARS values, respectively higher TBARS value had higher value of blood pressure.
6. CONCLUSION
Based on analyses of material and comparison of acquired results, we can conclude that the pregnant women with pregnancy induced hypertension (PIH) have extremely increased degree of oxidative stress and lipid peroxidation. TBARS values are in positive correlation with blood pressure values, respectively the highest TBARS value were present in pregnant women with the highest blood pressure values. This research shows that TBARS, being oxidative stress marker, could be applied in clinical work for assessment of clinical features difficulty and termination period of pregnancy induced hypertension, but it would request additional research on bigger number of pregnant women experiencing difficult hypertension in the first place.
Footnotes
• Author’s contributions: Conception and design: DD; Acquisition, analysis and interpretation of data: DD, DJ, NL; Drafting the article DD, DJ; Revising it critically for important intellectual content: DD, DJ, NL.
• Conflict of interest: none declared.
REFERENCES
- 1.National Institute of Health (NIH): National Heart, Lung, and Blood Institute. National High Blood Pressure Education Program: working group report on high blood pressure in pregnancy. NIH Publication; 2000. p. 3029. [Google Scholar]
- 2.Sibai BM, Dekker G, Kupferminc M. Preeclampsia: an update on its causation, diagnosis, prevention and management. Lancet. 2005;365:785–99. doi: 10.1016/S0140-6736(05)17987-2. [DOI] [PubMed] [Google Scholar]
- 3.Duley L. The global impact of pre-eclampsia and eclampsia. Semin Perinatol. 2009;33:130–7. doi: 10.1053/j.semperi.2009.02.010. [DOI] [PubMed] [Google Scholar]
- 4.Sibai BM. Best practices for diagnosis and management of preeclampsia. Obstet Gynecol Manage.2005; 17(2):20–32. [Google Scholar]
- 5.Koonin LM, Mackay AP, Berg CJ, et al. Pregnancy-related mortality surveillance, United States 1987–1990. MorbidityMortality Weekly Rep CDC Surveill Summ. 1997;46(4):17–36. [PubMed] [Google Scholar]
- 6.Zhang J, Meikle S, Trumble A. Severe maternal morbidity associated with hypertensive disorders in pregnancy in the United States. Hypertens Pregnancy. 2003;22:203. doi: 10.1081/PRG-120021066. [DOI] [PubMed] [Google Scholar]
- 7.Hamilton BE, Martin JA, Osterman MJK, Curtin SC, Mathews TJ. Final data for 2014. National vital statistics Report. 2015;64(12):49–63. [PubMed] [Google Scholar]
- 8.Berg CJ, Chang J, Callaghan WM, et al. Pregnancy-related mortality in the United States 1991-1997. Obstet Gynecol. 2003;101:289. doi: 10.1016/s0029-7844(02)02587-5. [DOI] [PubMed] [Google Scholar]
- 9.Backes CH, Markham K, Moorehead P, Cordero L, Craig A, Giannone PJ. Maternal Preeclampsia and Neonatal Outcomes. J Pregnancy. 2011 doi: 10.1155/2011/214365. http://www.hindawi.com/journals/jp/2011/214365/abs/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Roberts JM, Gammill HS. Preeclampsia: recent insights. Hypertension. 2005;46:1243–9. doi: 10.1161/01.HYP.0000188408.49896.c5. [DOI] [PubMed] [Google Scholar]
- 11.Milašinović LJ. Monitoring žena sa oboljenjem kardiovaskularnog sistema 6. Kongres perinatalne medicine sa međunarodnim učećem. Beograd: Zbornik radova; 2007. pp. 45–55. [Google Scholar]
- 12.Burton GJ, Jauniaux E. Oxidative stress. Best Pract. Res Clin Obstet Gynaecol. 2011;25:287–99. doi: 10.1016/j.bpobgyn.2010.10.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rudera EH, Hartmanb TJ, Goldman MB. Impact of oxidative stress on female fertility. Curr Opin Obstet Gynecol. 2009;21(3):219–22. doi: 10.1097/gco.0b013e32832924ba. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ðukić M, Ninković M, Jovanović M. Oxidative stress–Clinical diagnostic significance. Journal of Medical Biochemistry. 2008;27(4):409–25. [Google Scholar]
- 15.Novakov Mikić A. Thiobarbituric Acid Reactive Substances in pre-eclampsia. Med pregled. 2011;LXIV(7-8):377–80. doi: 10.2298/mpns1108377n. [DOI] [PubMed] [Google Scholar]
- 16.Gupta S, Aziz N, Sekhon L, et al. Lipid peroxsidation and antioxsidant status in preeclampsia;a systematic review. Obstet Gynecol Surv. 2009;64(11):750–9. doi: 10.1097/OGX.0b013e3181bea0ac. [DOI] [PubMed] [Google Scholar]
- 17.Patil SB, Kodliwadmath MV, Kodliwadmath M. Lipid peroxidation and antioxidant activity in complicated pregnancies. Clin Exp Obstet Gynecol. 2009;36(2):110–2. [PubMed] [Google Scholar]
- 18.Suhail M, Suhail MF. Koncentracije malondialdehida i antioksidativnih vitamina pupkovine kod majki oboljelih od preeklampsije i zdravih majki. Biochemia Medica. 2009;19(2):182–91. [Google Scholar]
- 19.Huber C, Robertson J, Taylor R, et al. Lipid peroxidation in pregnancy. New perspectives on preeclampsia. Am J Obstet Gynecol. 1989;161:1025–34. doi: 10.1016/0002-9378(89)90778-3. [DOI] [PubMed] [Google Scholar]
- 20.Sutherland MR, Bertagnolli M, Lukaszewski MA, et al. Preterm birth and hypertension risk: the oxidative stress paradigm. Hypertension. 2014;6:12–8. doi: 10.1161/HYPERTENSIONAHA.113.01276. [DOI] [PubMed] [Google Scholar]
- 21.Bhale DV, Hivre MD, Mahat RK, Bujurge AA. Comparative study of serum malondialdehyde levels as marker of oxidative stress in patients of pregnancy–induced hypertension and controls. Journal of Medical Sciencis. 2014;1(2):53–5. [Google Scholar]
- 22.Leidiane L, Francisco M, Pancich G, Thissiane LG. Oxidative Stress Markers in Pregnant Women with Preeclampsia. American Journal of Medical and Biological Research. 2015;3(3):68–73. [Google Scholar]
- 23.Watanabe K, Mori T, Iwasaki A, et al. Increased oxygen free radical production during pregnancy may impair vascular reactivity in preeclamptic women. Hypertens. Res. 2013;36:356–60. doi: 10.1038/hr.2012.208. [DOI] [PubMed] [Google Scholar]
- 24.Egić A. Predikcija preeklampsije u prvom trimestru. Imaging biomarkeri -perspektive i očekivanja. Udruženje za perinatalnu medicinu Srbije; 2013. Tara. Zbornik radova. 2013:101–4. [Google Scholar]
- 25.Kurlak LO, Green A, Loughna P, Broughton Pipkin F. Oxidative stress markers in hypertensive states of pregnancy: preterm and term disease. Frontiers in Physiology. 2014;5(310):1–8. doi: 10.3389/fphys.2014.00310. [DOI] [PMC free article] [PubMed] [Google Scholar]