

Abstract
Abdominal computed tomography in a 64 year-old male presenting hematuria showed two malignant tumors in the left kidney, thus radical nephrectomy was realized. In histological preparations a clear cell renal cell carcinoma and a papillary urothelial carcinoma were identified occurring synchronously, which is a rare occurrence having only about 50 cases reported in the literature.
Keywords: Left kidney, Hematuria, Malignant tumor, Nephrectomy
Introduction
The first case of synchronous neoplasms in the same kidney was reported by Graves R.C. and Templeton E.R. in 1921,1 however the finding of synchronous renal neoplasms in the same kidney is very uncommon. The authors did not identify a specific risk factors for the simultaneous presence of neoplasms although 24% of patients reported were smokers.2 We present a case report where clear cell renal cell carcinoma and papillary urothelial carcinoma were identified occurring synchronously in the same kidney.
Clinical case description
A 64 year-old male with medical history of 4–6 months presenting microscopic and macroscopic hematuria with the subsequent addition of pain in the left renal region. Smoker for 40 years, currently ceased. He denied any history of trauma, fever, or past history of stones. The other laboratory tests were normal. Abdominal computed tomography (Fig. 1) and ultrasound showed two tumors in the left kidney suggesting a malignant behavior, thus radical nephrectomy was realized.
Figure 1.
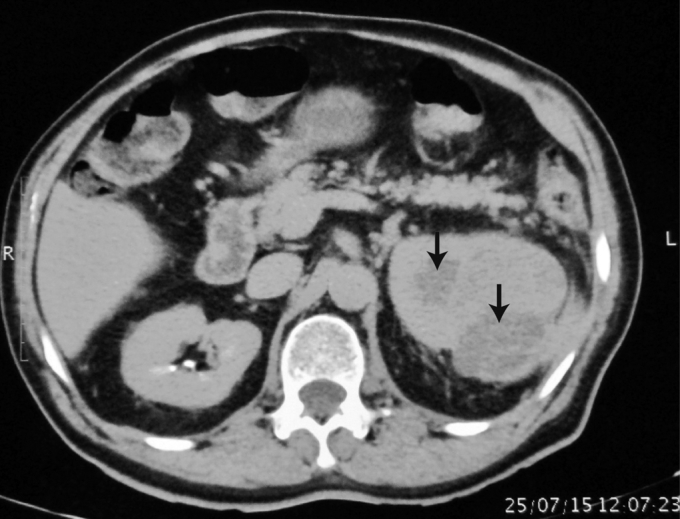
Preoperative abdominal computed tomography. The illustration shows the presence of two masses (arrows) in the left kidney.
The product of radical left nephrectomy was sent for pathological analysis consisting of a 19.5 × 10 × 8 cm specimen, yellow, smooth and shiny. The ureter, renal artery and vein together with 1 cm length without nodules. On opening of the kidney was observed in the upper renal pole a papillary tumor on renal pelvis measuring 3.5 × 1.5 × 2 cm encroaching the renal parenchyma. Moreover, in the parenchyma could be identified another white-yellow tumor measuring 6.5 × 5.8 × 5 cm with cavitated areas breaking the renal cortex and invading the peri-renal adipose tissue without exceeding the surgical edge. The adrenal gland was not extracted with the kidney (Fig. 2).
Figure 2.

Radical left nephrectomy. The illustration shows two neoplasm: a papillary urothelial carcinoma in the renal pelvis (red arrow) and a clear cell renal cell carcinoma in the parenchyma (black arrow).
In histological preparations of tumor on renal pelvis was identified a malignant epithelial neoplasm from urothelial lineage considered of low grade that grows in papillary structures with 30–40 layers of large cells presenting verticalized nucleus and isolated mitoses figures. The lesion invades the renal parenchyma, however it is distant from the limits of surgical section (Fig. 3A).
Figure 3.
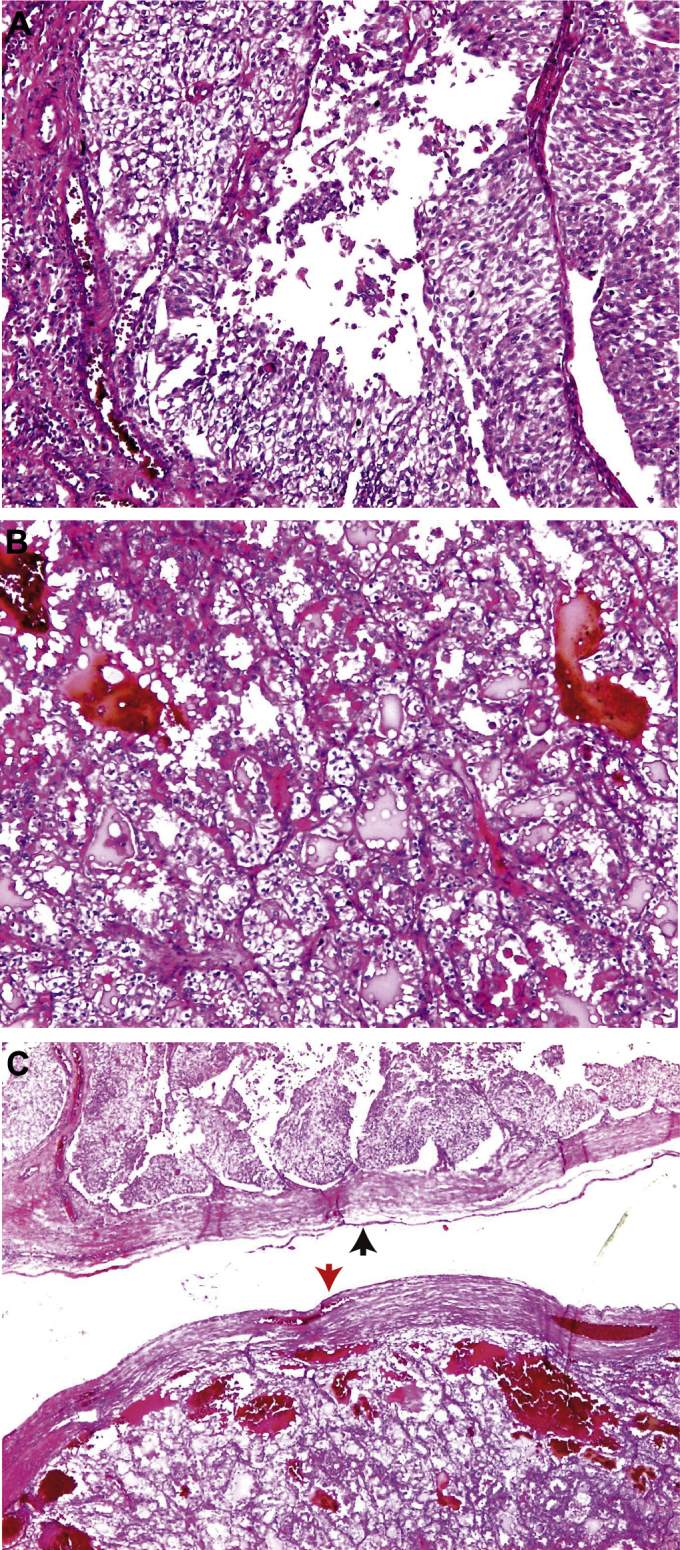
Histological findings. A) Papillary urothelial carcinoma (100×, H&E). B) Clear cell renal cell carcinoma from tubular lineage. The illustration shows abundant vascularization forming lakes of blood (100×, H&E). C) Both neoplasms are attached but not collide. The red arrow points the urothelial carcinoma and black arrow points renal cell carcinoma (25×, H&E).
In the parenchyma was found another malignant glandular epithelial neoplasm from tubular lineage that grows and encroaches on mantles or glands formed by clear cytoplasm cells with eosinophilic granular areas and medium nuclei presenting apparent nucleoli, corresponding to a clear cell renal cell carcinoma evaluated as Fuhrman grade 3. The abundant vascularization formed lakes of blood (Fig. 3B). The lesion invades peri-renal fat without exceeding the surgical margin. Both neoplasms are attached but not collide (Fig. 3C). The renal vein did not present neoplastic thrombi and artery and ureter were histologically normal.
Discussion
Renal cell carcinoma represents 85% of all kidney tumors in adults, affecting mainly older subjects between the sixth and seventh decade of life, with a preponderance 2:1 in favor of men. Meanwhile, clear cell renal cell carcinoma is responsible for 70–80% of renal cell cancer whereas upper tract urothelial carcinoma corresponds only 10–15%.1 According with this data, our patient presents the principal predisposing characteristics and the two most common kinds of renal cell carcinomas reported, however, their joint appearance in the same kidney, without being exceptional, it is a rare occurrence. Thus, only about 50 cases of synchronous renal neoplasm have been reported in the literature.
Previously have been reported cases where distinct combination of subtypes of renal cell carcinoma (clear cell, papillary, chromophobe, collecting duct) occurs synchronously in the same kidney.1, 2, 3, 4, 5 According with Ustuner M. et al (2014),3 the association of a papillary renal cell carcinoma and a clear cell renal cell carcinoma only have been reported in another two cases, thus correlating with our case. Remarkably, due to unknown causes, the left kidney is affected mostly as in this case report.1, 4 Moreover, the upper pole is mainly affected in the same way that solitary renal cell carcinomas.
The most common symptoms reported are hematuria in 90% of cases, flank pain in 19% and mass effect in 14%.1 Our patient presented the first two symptoms but did not feel mass effect although the kidney was enlarged.
Hart et al4 reported a case where both neoplasms collide, a transitional cell carcinoma and a clear cell renal cell carcinoma, however, in our case both neoplasm are close but not collide.
As regards aggressiveness, clear cell renal carcinoma presents the greatest malignant potential and a 5-year survival rate of 50–60%, while papillary and chromophobe renal cell carcinomas are associated with less metastatic potential and an overall 5-year survival of 80–90%.5 In this way, the prognosis in our patient was favorable.
Nowadays, radical nephrectomy is still considered a standard procedure for treating renal malignant neoplasm. However, recent studies show that patients with sporadic single or multiple ipsilateral renal tumors may undergo nephron-sparing surgery, with oncologically comparable results with low morbidity and recurrence rates.5 In this case, because of large tumoral mass affecting the upper pole was not possible to preserve nephron mass.
Conflict of interest
The authors declare that there is no conflict of interests regarding the publication of this paper.
References
- 1.Fernández-Arjona M., Santos-Arrontes D., DeCastro-Barbosa F. Carcinoma renal de células claras y carcinoma urotelial ipsilateral sincrónicos: aportación de un nuevo caso y revisión de la literatura. Arch Esp Urol. 2005;58:460–463. doi: 10.4321/s0004-06142005000500014. [DOI] [PubMed] [Google Scholar]
- 2.Mucciardi G., Galì A., D’Amico C. Transitional cell carcinoma of the renal pelvis with synchronous ipsilateral papillary renal cell carcinoma: case report and review. Urol Case Rep. 2015;3:93–95. doi: 10.1016/j.eucr.2015.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ustuner M., Yaprak B., Teke K. Coexisting papillary and clear renal cell carcinoma in the same kidney. Case Rep Urol. 2014;2014:575181. doi: 10.1155/2014/575181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hart A.P., Brown R., Lechago J., Truong L.D. Collision of transitional cell carcinoma and renal cell carcinoma. An immunohistochemical study and review of the literature. Cancer. 1994;73:154–159. doi: 10.1002/1097-0142(19940101)73:1<154::aid-cncr2820730126>3.0.co;2-k. [DOI] [PubMed] [Google Scholar]
- 5.Capaccio E., Varca V., Simonato A. Synchronous parenchymal renal tumors of different histology in the same kidney. Acta Radiol. 2009;50:1187–1192. doi: 10.3109/02841850903236120. [DOI] [PubMed] [Google Scholar]