

Acute posterior wall myocardial infarction (PMI) occurs in up to 20% of cases of acute myocardial infarction (MI), with the vast majority occurring along with inferior or lateral acute MI.1 A true PMI is considered more rare, with an incidence of approximately 3.3%.2 The term PMI is used for necrosis of the part of the left ventricle located beneath the atrioventricular sulcus.3 The majority of patients with the typical electrocardiogram (ECG) abnormalities of PMI have a stenosis or occlusion of the left circumflex coronary artery.4 The ECG diagnosis of PMI is difficult because no specific leads of the standard ECG directly represent this area.5 In addition, the lack of ST-segment elevation (as seen in typical ST-elevation MI) combined with misinterpreting the anterior ST-segment depressions as indicating ischemia rather than posterior infarction frequently lead to missing the diagnosis of PMI.
In PMI, there is loss of electrical forces in a dorsal direction, so the typical infarction pattern only appears in the electrodes placed dorsally between the spine and left scapula on the ECG. On the standard ECG of a true PMI, the leads V1 and V2 are a mirror image of the V1 and V2 leads of the anterior MI, resulting in ST-segment depression in leads V1 and V2 in PMI (Figure 1) rather than ST-segment elevation seen in acute anterior MI.5
Figure 1.

12-lead electrocardiogram from a 71-year-old woman with multiple cardiac risk factors presenting to the Emergency Department with 90 minutes of chest discomfort. Figure demonstrates a normal sinus rhythm with deep ST-segment depressions in leads V2–V4. Findings are consistent with an acute posterior wall myocardial infarction.
The QRS complex on the vector cardiogram points ventrally during PMI because of losses of normally dorsally aimed electrical forces, resulting in a prolonged R wave. An increase in the R/S ratio > 1.0 can occur in leads V1 and V2 as a case of PMI evolves.3,5 The increase of the R wave during PMI is the opposite to the Q wave associated with traditional ST-segment elevated MI. The ST segment points in the direction of the infarcted area, and ST-segment depression occurs in the precordial leads in the acute phase.3 The T wave points away from the infarcted area. As a result, a forward movement of the T wave can frequently be seen in patients with PMI. The combination of right precordial horizontal ST-segment depression with tall, upright T waves indicates an early ECG sign of acute ischemia of the posterior wall during a progressive PMI.6
The addition of posterior leads V7 to V9 significantly increases the ability to detect posterior injury patterns compared with the standard 12-lead ECG.5,7 Lead V7 should be placed at the level of lead V6 at the posterior axillary line, lead V8 on the left side of the back at the tip of the scapula, and lead V9 halfway between lead V8 and the left paraspinal muscles. When using posterior leads to diagnose PMI, ST-segment elevation in leads V7 through V9 is defined as elevation of at least 0.5 mm in 2 or more of the leads (Figure 2), on the basis of the increased distance between the posterior chest wall and the heart.7 Posterior ECG leads greatly improve sensitivity and specificity when identifying patients with isolated PMI.7
Figure 2.
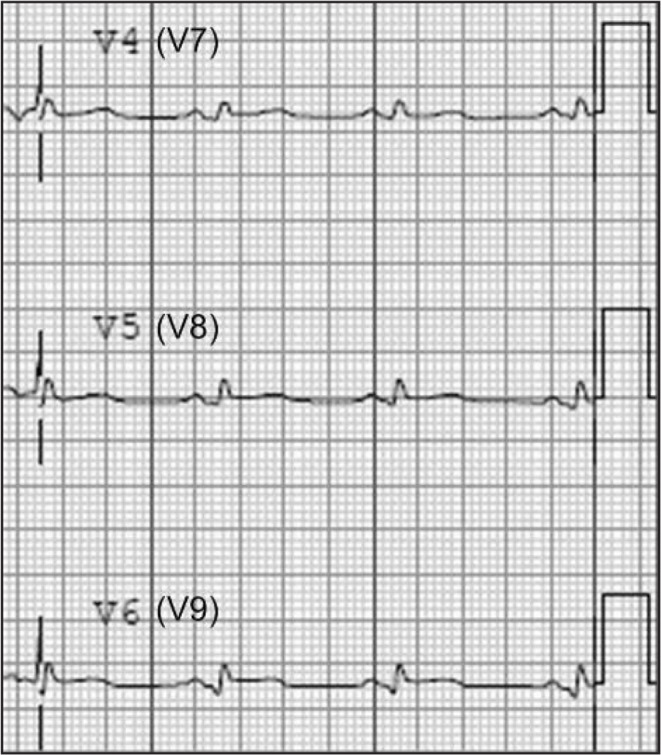
Posterior electrocardiogram leads V7–V9 from same patient, obtained shortly after the initial electrocardiogram (Figure 1). Figure 2 demonstrates 0.5 mm ST-segment elevation in leads V8 and V9, confirming the posterior wall myocardial infarction.
Footnotes
Disclosure Statement
The author(s) have no conflicts of interest to disclose.
References
- 1.Zalenski RJ, Cooke D, Rydman R, Sloan EP, Murphy DG. Assessing the diagnostic value of an ECG containing leads V4R, V8, and V9: the 15-lead ECG. Ann Emerg Med. 1993 May;22(5):786–93. doi: 10.1016/s0196-0644(05)80792-9. DOI: http://dx.doi.org/10.1016/S0196-0644(05)80792-9. [DOI] [PubMed] [Google Scholar]
- 2.Oraii S, Maleki M, Tavakolian AA, Eftekharzadeh M, Kamangar F, Mirhaji P. Prevalence and outcome of ST-segment elevation posterior electrocardiographic leads during acute myocardial infarction. J Electrocardiol. 1999 Jul;32(3):275–8. DOI: http://dx.doi.org/10.1016/S0022-0736(99)90110-3. [PubMed] [Google Scholar]
- 3.van Gorselen EO, Verheugt FW, Meursing BT, Oude Ophius AJ. Posterior myocardial infarction: the dark side of the moon. Neth Heart J. 2007 Jan;15(1):16–21. [PMC free article] [PubMed] [Google Scholar]
- 4.Bough EW, Korr KS. Prevalence and severity of circumflex coronary artery disease in electrocardiographic posterior myocardial infarction. J Am Coll Cardiol. 1986 May;7(5):990–6. doi: 10.1016/s0735-1097(86)80216-9. DOI: http://dx.doi.org/10.1016/S0735-1097(86)80216-9. [DOI] [PubMed] [Google Scholar]
- 5.Rich MW, Imburgia M, King TR, Fischer KC, Kovach KL. Electrocardiographic diagnosis of remote posterior wall myocardial infarction using unipolar posterior lead V9. Chest. 1989 Sep;96(3):489–93. doi: 10.1378/chest.96.3.489. DOI: http://dx.doi.org/10.1378/chest.96.3.489. [DOI] [PubMed] [Google Scholar]
- 6.Agarwal JB, Khaw K, Aurignac F, LoCurto A. Importance of posterior chest leads in patients with suspected myocardial infarction, but nondiagnostic, routine 12-lead electrocardiogram. Am J Cardiol. 1999 Feb 1;83(3):323–6. doi: 10.1016/s0002-9149(98)00861-3. DOI: http://dx.doi.org/10.1016/S0002-9149(98)00861-3. [DOI] [PubMed] [Google Scholar]
- 7.Matetzky S, Freimark D, Feinberg MS, et al. Acute myocardial infarction with isolated ST-segment elevation in posterior chest leads V7-9: “hidden” ST-segment elevations revealing acute posterior infarction. J Am Coll Cardiol. 1999 Sep;34(3):748–53. doi: 10.1016/s0735-1097(99)00249-1. DOI: http://dx.doi.org/10.1016/S0735-1097(99)00249-1. [DOI] [PubMed] [Google Scholar]