

Sir,
The sub-Tenon's block is commonly used for providing anaesthesia and akinesia during ophthalmic surgery due to the reduced risk of complications as compared to needle-based blocks.[1]
Traditional approach involves making a conjunctival incision with blunt forceps and sprung Westcott scissors 5–8 mm away from the limbus, followed by insertion of disposable 19-gauge single-use rigid metal cannula into the sub-Tenon's space.[1,2] Despite being safer than the needle-based blocks[3], conjunctival haemorrhage occurs and the technique is relatively expensive (approximately 10 USD for single-use 19-gauge sub-Tenon's cannula and additional cost of sterilisation of scissors and forceps).
Allman et al.[4,5] described an incisionless sub-Tenon's block without prior conjunctival incision using a 21-gauge, 25 mm, angled and blunt pencil point disposable triport sub-Tenon's cannula [Figure 1] (much more expensive than routinely used disposable sub-Tenon's cannula). We use the incisionless technique using 21-gauge, 25 mm, angled, metal and re-sterilisable sub-Tenon's cannula [Figure 2]. The conjunctiva is anaesthetised with topical anaesthetic drops and a lid speculum is inserted. The patient is asked to look up and out and a small tent of conjunctiva is elevated using blunt forceps (Moorfields) in the inferonasal quadrant 5–8 mm away from the limbus. Without making any prior incision, the reusable cannula is inserted directly through the conjunctiva (lateral to the globe) and then rotated to follow the contour of the globe and a desired volume of local anaesthetic agent is injected.
Figure 1.
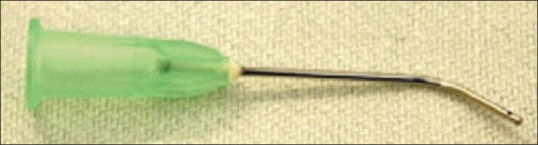
Modified from Lin et at 21-gauge, 25.4 cm long (1 inch), angled triport sub-Tenon's curved metal disposable cannula
Figure 2.
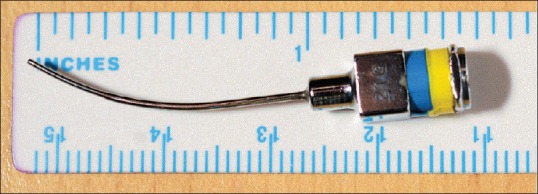
Original reusable 21-gauge, 25.4 cm long (1 inch), curved metal cannula for incisionless sub-Tenon's block
We have used the reusable sub-Tenon's cannula in more than 450 patients over 1 year without any injury and known complications with the added advantage of reduced conjunctival haemorrhage, which is frequently associated with standard sub-Tenon's block.[3] The cost-savings of this incision-less technique would also take account of obviating the need of sterilising the scissors, but one has to consider the initial cost of metal sub-Tenon's cannula.
Incisionless sub-Tenon's block can be made affordable using reusable 21-gauge metal cannula and is an effective alternative to needle-based blocks, which may be adopted in countries where reusable equipment use may not be prohibitive.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Roman SJ, Chong Sit DA, Boureau CM, Auclin FX, Ullern MM. Sub-Tenon's anaesthesia: An efficient and safe technique. Br J Ophthalmol. 1997;81:673–6. doi: 10.1136/bjo.81.8.673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kumar CM, Dodds C. Sub-Tenon's anesthesia. Ophthalmol Clin North Am. 2006;19:209–19. doi: 10.1016/j.ohc.2006.02.008. [DOI] [PubMed] [Google Scholar]
- 3.Kumar CM, Eid H, Dodds C. Sub-Tenon's anaesthesia: Complications and their prevention. Eye (Lond) 2011;25:694–703. doi: 10.1038/eye.2011.69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Allman KG, Theron AD, Byles DB. A new technique of incisionless minimally invasive Sub-Tenon's anaesthesia. Anaesthesia. 2008;63:782–3. doi: 10.1111/j.1365-2044.2008.05592.x. [DOI] [PubMed] [Google Scholar]
- 5.Lin S, Ling RH, Allman KG. Real-time visualisation of anaesthetic fluid localisation following incisionless Sub-Tenon block. Eye (Lond) 2014;28:497–8. doi: 10.1038/eye.2014.14. [DOI] [PMC free article] [PubMed] [Google Scholar]