

Abstract
The objective of this study was to use performance-based measurements to identify, in a population of community-dwelling American Indians aged ≥55 years, the prevalence and correlates of lower body functioning. Data were collected as part of a cross-sectional study of disability with members of a tribe in the southeast. Lower body functioning was measured with the Short Physical Performance Battery (SPPB) where higher scores reflect better functioning. Independent variables included age, sex, marital status, educational attainment, current cigarette smoking, physical activity, body mass index, hearing loss, vision loss, bone or joint trauma, chronic pain syndrome, osteoporosis, medical comorbidity, and depressive symptomatology. The total composite SPPB score was 8.80± 3.4 and declined significantly with increasing age and was negatively associated with unmarried status, physical inactivity, vision loss, bone or joint trauma, and medical comorbidity after adjustment for all other factors in the model. Likewise, all individual SPPB component scores declined significantly with increasing age, and were negatively associated with physical inactivity and comorbidity. In addition, the balance test score was significantly and negatively associated with unmarried status and vision loss; gait speed was negatively related to unmarried status; and the chair stand test scores were negatively related to body mass index, vision loss, bone or joint trauma, and chronic pain syndrome. In the clinical setting, the SPPB can be an important screening tool for adverse health-related events. Further studies are needed to investigate the determinants and sequelae of physical dysfunction in this population.
Keywords: American Indians, disability, balance, gait, chair stands, mobility, physical functioning
Introduction
The aging process and functioning in American Indians is poorly understood although over 4.2 million American Indians live in the U.S.1 and 1,319,000 will be aged ≥ 55 years old by 2020.2 The scant and relatively dated data on older American Indian adults suggests that disability rates in this population rank among the highest of any U.S. racial group, far exceeding those of their White counter parts. Using the 2000 Census data, the prevalence of a functional limitation, mobility disability, and self-care disability among persons aged ≥ 55 years was 36%, 21%, and 12% among American Indians versus 25%, 17%, and 9% among Whites.3 A second study examining the 2000 Census data revealed that differences were even more striking among those aged ≥ 65 years, with 58% among American Indians versus 42% among all other racial groups reporting a disability.4
To date, studies regarding physical functioning in American Indian populations have only used self-reported measures, which may be strongly influenced by social and cultural factors.5-7 To address this concern, the primary objective of this study was to use performance-based measurements to examine the prevalence and correlates of poor lower body physical functioning in a population of community-dwelling American Indian elders.
Methods
Data Source
Data for this research were collected as part of the Native Elder Care Study, a cross-sectional study of community-dwelling members of an American Indian tribe via in-person assessments.8 The participating tribe is a federally-recognized tribe in a rural Southeast region of the U.S. The study gathered in-depth information via interviewer-administered surveys on lower body functioning, disability, personal assistance needs, mental and physical health conditions, psychosocial resources, and use of health care and supportive services. All hired interviewers received 8 hours of training, including human subject protection certification, survey administration, and safety. Lower body functioning, the outcome of interest for the analyses, was measured by the Short Physical Performance Battery (SPPB). For the administration of the SPPB, the study's principal investigator and research coordinator received in-person training by the developer of the SPPB protocol. The principal investigator and research coordinator then trained the interviewers supported by a self-produced video demonstrating the administration of the battery to 6 fictitious participants with varying abilities. Interviewers were retrained every 3 months on the SPPB protocol.
Data were collected between July 2006 and August 2008. To be included in the study, participants had to be an enrolled tribal member, aged ≥ 55 years, non-institutionalized, cognitively intact, and reside in the tribe's service area. A lower age criterion was used because research suggests that health declines with age more rapidly in American Indians than in other racial groups, and that chronic disease burden is continuing to increase in American Indians.9 In addition, many American Indian communities, including the tribe participating in this study, consider elders as those aged ≥ 55 years.
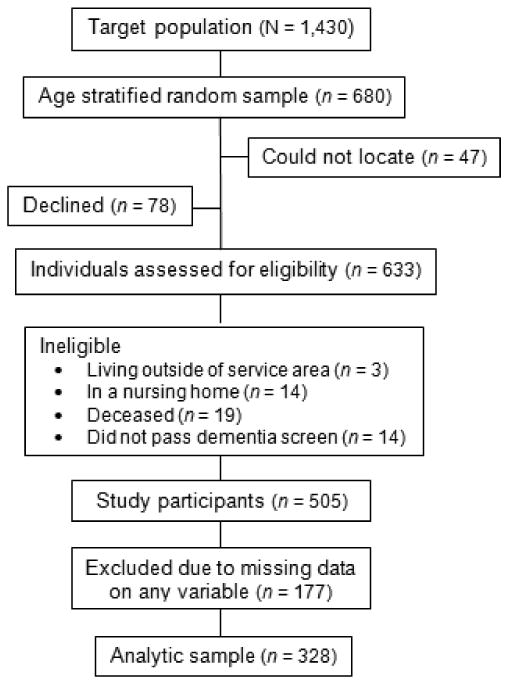
Figure 1 shows participant enrollment for the Native Elder Care Study. The tribal enrollment records indicated that there were 1,430 potentially eligible adults based on age and residential location. From this list, a random sample of 680 adults was drawn, stratified by three age groups: 55-64, 65-74, and ≥75 years. Potentially eligible persons were invited to participate via a telephone call or a home visit by an interviewer. Forty-seven adults could not be located, 78 declined participation, and 50 were determined to be ineligible (3 living outside of service area, 14 in a nursing home, 19 were deceased, 14 who did not pass the dementia screen10). The remaining 505 participants received comprehensive, in-person assessments; all assessments were conducted by trained interviewers and lasted between 60 to 90 minutes. The majority of interviews were conducted in the participant's home (87%) and the remaining performed in a tribal building. Propensity to decline participation increased with age, although this was not significant, and men were more likely to decline than women (p≤ 0.001).
Figure 1. Participant enrollment.
The tribe's Institutional Review Board, Tribal Council, Tribal Elder Council, and West Virginia University Institutional Review Board approved the project. All study participants provided informed consent and received a $20 gift card for completing the interview.
Measures
Dependent Variables
The SPPB is an important measure of functioning as it has been shown to predict falls,11 disability,12, 13 nursing home admission,12 and mortality.12, 14 The SPPB measures lower body functioning with three tasks: hierarchical test of standing balance, four meter walk, and chair stands.12 Scores on all three tests range from 0 to 4, with higher scores indicative of better test performance, which summed generates a SPPB total score ranging from 0 to 12. To assess standing balance, each participant attempted 3 increasingly difficult positions without the assistance of devices. Participants were first tested standing with feet side by side, then in a semi-tandem position with the heel of one foot beside the big toe of the other foot, and last, in a tandem position with the heel of one foot directly in front of the toe of the other foot. Participants were asked to hold each position for 10 seconds. Each balance test was scored and summed to generate a total balance score.
For the 4-meter walk, a walking course was measured and marked with masking tape. If the participants felt they could complete the walk safely, they were asked to walk the course at their usual pace past the end of the course. If needed, participants were permitted to use a cane or other walking aid. If the participant was unable to perform the walk, they were given a score of 0 and progressively higher scores for faster completion of the course.
The chair stand test assessed whether the participant could stand up from a chair without the assistance of arms. If the participant could safely stand from the chair, they were then asked to stand up from the chair 5 times as quickly as possible without the use of arms. Progressively higher scores were assigned based on the speed in which the 5 chair stands were completed; participants who could not complete 5 chair stands or completed the stands in > 60 seconds received a score of 0.
SPPB validity and reliability have been established with large community-based geographically and racially diverse samples of older adults.12, 15 In this study, interviewer training testing for measurement of inter-rater reliability on the SPPB showed an intra-class correlation of 0.84 indicating between moderate to high reliability.
Independent Variables
Independent variables included demographic characteristics, health-related behaviors, body mass index, medical history, and depressive symptomatology. Demographic characteristics included age, sex, marital status, and educational attainment. Age was measured in years. Marital status was coded to indicate whether the respondent was married/had a life partner or other. Educational attainment was coded into three categories, which were ≤ 11 years, high school graduate/General Education Development, and some college or greater.
Health-related behaviors included self-report of current cigarette smoking status (current smoker vs. not a current smoker) and self-report of engagement in non-occupational related physical activity during the previous month (yes or no). Body mass index was calculated as weight in kilograms divided by height in meters squared and analyzed as a continuous variable. Anthropometric indices were measured by interviewers at the time of assessment.
Medical history was measured using self-reported physician diagnosis.16, 17 For the purposes of analyses, specific health conditions were collapsed into 6 categories: (1) Hearing loss; (2) vision loss; (3) bone or joint trauma, defined as history of broken bone, joint replacement, joint fusion, and/or amputation; (4) chronic pain syndrome, defined as back pain, arthritis, and/or a chronic pain syndrome; (5) osteoporosis; and (6) medical comorbidity, defined as total number of chronic medical conditions including heart disease, stroke, angina, congestive heart failure, heart attack, lung disease, Parkinson's disease, cancer, diabetes, high blood pressure, kidney disease, and liver disease, ranging from 0 to 12. Hearing loss, vision loss, bone or joint trauma, chronic pain syndrome, and osteoporosis were all coded as binary variables (diagnosed vs. not diagnosed by a physician). Medical comorbidity was also coded as a binary variable with ≥ 2 conditions versus 0 or 1 condition.
Depressive symptomatology was assessed using the Center for Epidemiologic Studies Depression Scale (CES-D), a multidimensional screening instrument for mood disorders and acute depressive symptoms experienced over a 7-day period.18 The CES-D is a widely used instrument and has been validated with older American Indians.19 Scores were analyzed as a binary variable using the standard cut-off of 16 reflecting a clinically significant level of psychological distress.18
Statistical Analyses
Descriptive statistics were used to examine sample characteristics and scores on the SPPB. Independent t and chi square tests were used to assess potential differences in mean SPPB scores by the independent variables and to evaluate potential differences in those with versus without missing data. Analysis of variance was performed to compare sex-adjusted SPPB scores among the age groups. Multiple ordinary least squares regression was used to identify significant independent correlates of the overall SPPB score. Multiple ordinal logistic regression was used to investigate the correlates of the individual SPPB component (balance, gait, and chair stand tests) scores. A p value of ≤ 0.05 was used to determine statistical significance. The variance inflation factor was estimated to assess multi-collinearity among the independent variables; based on this analysis, no multi-collinearity was detected. One hundred and seventy-seven participants who lacked complete data on the SPPB or on the independent variables of interest were excluded from the analyses, resulting in a final analytic sample of 328 (see Figure 1). Those who had missing data on the SPPB did not differ significantly with respect to age and sex from those with complete SPPB data. Those who had missing data on the SPPB and/or the independent variables were more likely to have lower educational levels (p≤ 0.05), hearing loss (p≤ 0.001), and bone or joint trauma (p≤ 0.01). All analyses used SAS software package version 9.1 (SAS Institute, Inc., Cary, NC).
Results
The Table gives the characteristics of the study population and mean SPPB scores by the independent variables. Mean SPPB composite scores were lower as the age groups increased. The mean SPPB was significantly lower among participants who were female, unmarried, with lower educational levels, nonsmokers, and physically inactive. SPPB scores also averaged significantly lower in those who had hearing loss, vision loss, bone or joint trauma, chronic pain syndrome, osteoporosis, ≥ 2 medical comorbidities, and CES-D scores ≥ 16.
Table. Sample characteristics (n = 328).
| n | (%) | SPPB Score | |||
|---|---|---|---|---|---|
|
| |||||
| Mean | SD | p value | |||
|
|
|
||||
| Age | <0.01 | ||||
| 55-64 | 109 | (33.2) | 9.6 | 3.1 | |
| 65-74 | 131 | (40.0) | 9.0 | 2.8 | |
| ≥75 | 88 | (26.8) | 5.6 | 3.9 | |
| Mean age in years (SD) | 69.5 | (9.6) | |||
| Sex | <0.001 | ||||
| Female | 211 | (64.3) | 7.8 | 3.7 | |
| Male | 117 | (35.7) | 9.2 | 3.2 | |
| Marital Status | <0.01 | ||||
| Married | 159 | (48.5) | 9.3 | 3.1 | |
| Unmarried | 169 | (51.5) | 7.3 | 3.7 | |
| Educational Status | <0.01 | ||||
| 1-11 years | 112 | (34.2) | 7.4 | 3.5 | |
| High school grad/GED | 106 | (32.3) | 8.0 | 3.8 | |
| College graduate or more | 110 | (33.5) | 9.4 | 3.1 | |
| Current Smoker | 0.02 | ||||
| Yes | 71 | (21.7) | 9.1 | 3.0 | |
| No | 257 | (78.3) | 8.1 | 3.7 | |
| Physically Active in Last Month | <0.01 | ||||
| Yes | 208 | (63.4) | 9.0 | 3.2 | |
| No | 120 | (36.6) | 7.1 | 3.9 | |
| Body Mass Index | 0.59 | ||||
| Under weight | 7 | (2.1) | 8.0 | 3.2 | |
| Normal weight | 76 | (23.2) | 7.8 | 3.9 | |
| Overweight | 110 | (33.5) | 8.5 | 3.4 | |
| Obese | 135 | (41.2) | 8.4 | 3.5 | |
| Mean body mass index (SD) | 29.4 | (6.4) | |||
| Hearing Loss | 0.01 | ||||
| Yes | 81 | (24.7) | 7.4 | 3.8 | |
| No | 247 | (75.3) | 8.6 | 3.4 | |
| Vision Loss | <0.01 | ||||
| Yes | 105 | (32.0) | 6.9 | 3.8 | |
| No | 223 | (68.0) | 8.9 | 3.3 | |
| Bone or Joint Trauma | <0.01 | ||||
| Yes | 90 | (27.4) | 6.6 | 3.9 | |
| No | 238 | (72.6) | 8.9 | 3.2 | |
| Chronic Pain Syndrome | <0.01 | ||||
| Yes | 189 | (57.6) | 7.4 | 3.7 | |
| No | 139 | (42.4) | 9.5 | 3.0 | |
| Osteoporosis | <0.01 | ||||
| Yes | 37 | (11.3) | 6.8 | 3.5 | |
| No | 291 | (88.7) | 8.5 | 3.5 | |
| Medical Comorbidity Score* | <0.01 | ||||
| 2 or greater | 167 | (50.9) | 7.3 | 3.6 | |
| 0-1 | 161 | (49.1) | 9.3 | 3.2 | |
| Mean number of conditions (SD) | 1.8 | (1.6) | |||
| CES-D Score | 0.05 | ||||
| ≥16 | 41 | (12.5) | 7.2 | 3.7 | |
| <16 | 287 | (87.5) | 8.4 | 3.5 | |
| Mean CES-D score | 6.5 | (8.3) | |||
Includes heart disease, stroke, angina, congestive heart failure, heart attack, lung disease, Parkinson's disease, cancer, diabetes, high blood pressure, kidney disease, and liver disease. SD = standard deviation; GED = General Educational Development; CES-D = Center for Epidemiologic Studies Depression Scale.
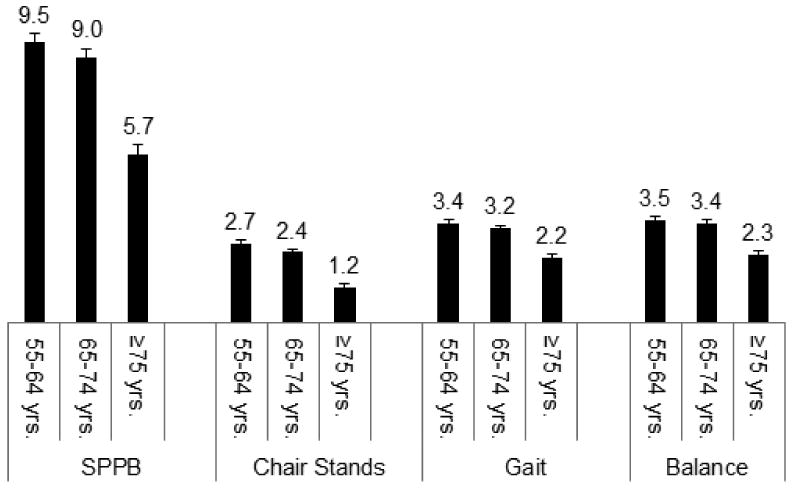
The data indicated that 51.8% of the sample had SPPB scores of 9 or less, with an average SPPB score of 8.8 ± 3.4 (data not shown), suggesting relatively poor physical functioning in this population.20 Figure 2 presents the sex-adjusted mean total SPPB composite score and balance, gait speed, and chair stand test scores stratified according to age group. Mean composite SPPB score declined significantly with increasing age (P = .001). Scores for each the separate components of the SPPB likewise decreased significantly with rising age (all P ≤ .001).
Figure 2. Sex-adjusted mean scores on the composite SPPB and the individual tests (n = 328).
Results from the multiple ordinary least squares regression showed that total composite SPPB score declined significantly with increasing age (P = .001) and was significantly and negatively associated with unmarried status (P = .004), physical inactivity (P = .001), vision loss (P = .049), bone or joint trauma (P = .02), and medical comorbidity (P = .005) after adjustment for all other factors in the model.
Results from the multiple ordinal logistic regressions identified correlates of the individual tests that make up the SPPB. The balance test score declined significantly with increasing age (P = .001), and was negatively associated with unmarried status (P = .01), physical inactivity (P = .05), vision loss (P = .04), and medical comorbidity (P = .01). The gait speed test score declined significantly with increasing age (P < .001) and was negatively associated with unmarried status (P = .006), physical inactivity (P = .01), and medical comorbidity (P = .001). Chair stand test score declined significantly with increasing age (P < .001) and was negatively associated with physical inactivity (P = .01), BMI (P = .01), vision loss (P = .04), bone or joint trauma (P = .02), chronic pain syndrome (P = .02), and medical comorbidity (P = .047).
Discussion
The purpose of this study was to identify, in a population of community-dwelling older American Indians, the prevalence and correlates of poor lower body functioning. The few studies with older American Indians suggest relatively high rates of functional disability in this population. However, findings of previous studies with American Indian elders have been based on self-reported measures, and to date, investigations employing performance-based measures are lacking. This is the first study to investigate functioning in American Indian elders using objective performance measures.
Examining physical functioning using objective measures is particularly important with American Indian populations given that several prevalent cultural constructs may affect the validity of self-report data. For example, previous research has identified “harmony ethic,”7 “passive forbearance,”6 and “tolerated illness”5 as cultural phenomena in American Indians. Generally, these constructs reflect the values of autonomy, the ability to endure pain, hardships, and frustration without external evidence of discomfort. As such, harmony ethic, passive forbearance, and tolerated illness have been proposed as factors leading to the significant under-reporting of functional difficulties.
Given that a SPPB score of ≤ 9 is considered poor performance,20 these findings suggest that the Native Elder Care Study participants had poor lower body functioning overall. Comparing these findings to other published data is challenging for two reasons. First, performance-based measures have not been previously reported on American Indians. Second, the differing sampling approaches and inclusion criteria across studies makes is difficult to compare the mean SPPB score on this sample to published results with other race and ethnic populations.
The studies with older American Indians have identified correlates of self-reported activities of daily living limitations including increased age, not being married, physical inactivity, and comorbidity.3, 21-23 Significant correlates of poor lower body functioning identified here are consistent with previous research with other race and ethnic groups that also used the SPPB, including increased age,24-26 chronic disease,15, 24, 26 physical inactivity,25 bone trauma,24 increased body mass index,24 and pain.27, 28
Strengths of this study include the population-based design, relatively large and representative study sample, and high participation rates. Additional strengths include the objective measures of physical functioning and comprehensive assessment of potential demographic, behavioral, and health-related correlates. There are several limitations to this study that deserve acknowledgement. Perhaps the most important limitation is the cross-sectional nature of the data, precluding determination of causal relationships. To date, there are no studies that have examined functional disability among American Indians over time thus future research is needed to examine functional disability longitudinally to establish causality. Second, the presence of chronic conditions was based on self-report, thus potentially introducing bias. However, research has shown that there is generally good agreement between self-report of diagnosis and physician diagnosis for older adults.29, 30 Other research has suggested that there is generally lower sensitivity of self-report versus medical record data, which would tend to attenuate the observed associations.31, 32
Study participants were also restricted to community-dwelling persons aged ≥ 55 years, limiting generalizability to other age groups, those in an institution, or persons with cognitive impairments. Participants were members of a single American Indian tribe. Tremendous regional and tribal variation in health33 and disability4 has been documented among peoples known collectively as American Indians. Thus caution is warranted in generalizing the results to other American Indian communities or populations.
Despite these limitations, this research contributes to the limited understanding of functioning among aging American Indians. The SPPB has been determined to be an important screening tool for adverse health-related events.34 Studies that help identify modifiable factors amenable to interventions designed to improve function can have implications for clinical and public health practice. The use of the SPPB in the clinical setting can inform referrals to community-based programs designed to strengthen the lower body and improve balance. For instance, lower body functioning is a strong predictor of falls11 and data suggest that American Indians have a disproportionate risk compared to other race and ethnic groups. Analyses of the 2006 Behavioral Risk Factor Surveillance System found that 28% of American Indians reported at least one fall during the preceding three months compared to 13% of Asians and Pacific Islanders and African Americans, 17% of Hispanics, and 16% of Whites.35 It is important that clinicians have information about variations in fall rates and risk factors for the full range of race and ethnicities of their patients. In response to the findings from the Native Elder Care Study, the participating tribe implemented a geriatrics clinic where patients receive a comprehensive assessment that is used to guide treatment plans and to identify needed rehabilitative services as well as community-based health promotion programs.
To develop appropriate responses to the growing demands on the long-term care system among older American Indians, routine functional assessments can aid tribes, states, the Indian Health Service, and the Centers for Medicare and Medicaid Services in identifying and addressing both formal and informal care needs. Older American Indians are among the fastest growing populations in the United States with an estimated 1,319,000 who will be aged ≥ 55 years by 2020.2 With relatively limited research examining the functional status of older American Indians, further studies are needed to investigate the determinants and sequelae of physical dysfunction and to inform clinical and public health intervention efforts.
Acknowledgments
The authors would like to thank Drs. Blythe Winchester and Elizabeth Phelan for their geriatric practice perspectives on the findings, Dr. Gerry Hobbs for his statistical guidance, and Drs. Spero Manson and Stephanie Studenski for mentorship and support.
Footnotes
Conflict of Interest: R. Turner Goins received funding from the National Institute on Aging, National Institutes of Health (K01 AG022336).
Author Contributions:
Goins: Secured funding for the study, planned the study, supervised data collection and data entry, directed the data analysis, and wrote the paper.
Innes: Assisted in data analysis and in the development and revision of the paper.
Dong: Conducted all of the data analysis and assisted in writing the paper.
Sponsor's Role: The sponsor had no role in the design, methods, analysis, or preparation of the manuscript.
References
- 1.United States Census Bureau, editor. United States Census Bureau. United States Census. 2002. [Google Scholar]
- 2.United States Census Bureau, editor. United States Census Bureau. United States Census. 2008. [Google Scholar]
- 3.Goins RT, Moss M, Buchwald D, et al. Disability among older American Indians and Alaska Natives: An analysis of the 2000 Census Public Use Microdata Sample. Gerontologist. 2007;47:690–696. doi: 10.1093/geront/47.5.690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Moss MP, Schell MC, Goins RT. Using GIS in a first national mapping of functional disability among older American Indians and Alaska Natives from the 2000 census. Int J Health Geogr. 2006;5:37. doi: 10.1186/1476-072X-5-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Moss MP. Tolerated Illness concept and theory for chronically ill and elderly patients as exemplified in American Indians. J Cancer Educ. 2005;20:17–22. doi: 10.1207/s15430154jce2001s_05. [DOI] [PubMed] [Google Scholar]
- 6.Strong C. Stress and caring for elderly relatives: Interpretations and coping strategies in an American Indian and white sample. Gerontologist. 1984;24:251–256. doi: 10.1093/geront/24.3.251. [DOI] [PubMed] [Google Scholar]
- 7.Loftin JD. The “Harmony Ethic” of the conservative Eastern Cherokees: A religious interpretation. J Cherokee Stud. 1983;8:40–43. [Google Scholar]
- 8.Goins RT, Garroutte EM, Fox SL, et al. Theory and practice in participatory research: lessons from the Native Elder Care Study. Gerontologist. 2011;51:285–294. doi: 10.1093/geront/gnq130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hayward MD, Heron M. Racial inequality in active life among adult Americans. Demography. 1999;36:77–91. [PubMed] [Google Scholar]
- 10.Inouye SK, Robison JT, Froehlich TE, et al. The time and change test: A simple screening test for dementia. J Gerontol A Biol Sci Med Sci. 1998;53:M281–286. doi: 10.1093/gerona/53a.4.m281. [DOI] [PubMed] [Google Scholar]
- 11.Abellan Van Kan G, Rolland Y, Andrieu S, et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J Nutr Health Aging. 2009;13:881–889. doi: 10.1007/s12603-009-0246-z. [DOI] [PubMed] [Google Scholar]
- 12.Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49:M85–94. doi: 10.1093/geronj/49.2.m85. [DOI] [PubMed] [Google Scholar]
- 13.Ostir GV, Markides KS, Black SA, et al. Lower body functioning as a predictor of subsequent disability among older Mexican Americans. J Gerontol A Biol Sci Med Sci. 1998;53:M491–495. doi: 10.1093/gerona/53a.6.m491. [DOI] [PubMed] [Google Scholar]
- 14.Markides KS, Black SA, Ostir GV, et al. Lower body function and mortality in Mexican American elderly people. J Gerontol A Biol Sci Med Sci. 2001;56:M243–247. doi: 10.1093/gerona/56.4.m243. [DOI] [PubMed] [Google Scholar]
- 15.Ostir GV, Volpato S, Fried LP, et al. Reliability and sensitivity to change assessed for a summary measure of lower body function: Results from the Women's Health and Aging Study. J Clin Epidemiol. 2002;55:916–921. doi: 10.1016/s0895-4356(02)00436-5. [DOI] [PubMed] [Google Scholar]
- 16.Goins RT, Pilkerton CS. Comorbidity among older American Indians: The Native Elder Care Study. J Cross Cult Gerontol. 2010;25:343–354. doi: 10.1007/s10823-010-9119-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rigler SK, Studenski S, Wallace D, et al. Co-morbidity adjustment for functional outcomes in community-dwelling older adults. Clin Rehabil. 2002;16:420–428. doi: 10.1191/0269215502cr515oa. [DOI] [PubMed] [Google Scholar]
- 18.Radloff LS Center for Epidemiologic Studies Depression Scale. The CES-D Scale: A self-report depression scale for research in the general population. Appl Psychol Measure. 1977;1:385–401. [Google Scholar]
- 19.Chapleski EE, Lichtenberg PA, Dwyer JW, et al. Morbidity and comorbidity among Great Lakes American Indians: Predictors of functional ability. Gerontologist. 1997;37:588–597. doi: 10.1093/geront/37.5.588. [DOI] [PubMed] [Google Scholar]
- 20.Bean JF, Leveille SG, Kiely DK, et al. A comparison of leg power and leg strength with the InCHIANTI Study: Which influences mobility more? J Gerontol A Biol Sci Med Sci. 2003;58A:728–732. doi: 10.1093/gerona/58.8.m728. [DOI] [PubMed] [Google Scholar]
- 21.Fitzpatrick TR, Aleman S, Van Tran T. Factors that contribute to levels of independent activity functioning among a group of Navajo elders. Res Aging. 2008;30:318–333. [Google Scholar]
- 22.Fuller-Thomson E, Minkler M. Functional limitations among older American Indians and Alaska natives: Findings from the Census 2000 Supplementary Survey. Am J Public Health. 2005;95:1945–1948. doi: 10.2105/AJPH.2004.053462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Moss MP, Roubideaux YD, Jacobsen C, et al. Functional disability and associated factors among older Zuni Indians. J Cross Cult Gerontol. 2004;19:1–12. doi: 10.1023/B:JCCG.0000015013.36716.45. [DOI] [PubMed] [Google Scholar]
- 24.Ferrucci L, Penninx BW, Leveille SG, et al. Characteristics of nondisabled older persons who perform poorly in objective tests of lower extremity function. J Am Geriatr Soc. 2000;48:1102–1110. doi: 10.1111/j.1532-5415.2000.tb04787.x. [DOI] [PubMed] [Google Scholar]
- 25.Chale-Rush A, Guralnik JM, Walkup MP, et al. Relationship between physical functioning and physical activity in the lifestyle interventions and independence for elders pilot. J Am Geriatr Soc. 2010;58:1918–1924. doi: 10.1111/j.1532-5415.2010.03008.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Volpato S, Cavalieri M, Guerra G, et al. Performance-based functional assessment in older hospitalized patients: Feasibility and clinical correlates. J Gerontol A Biol Sci Med Sci. 2008;63A:1393–1398. doi: 10.1093/gerona/63.12.1393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Cecchi F, Molino-Lova R, Di Iorio A, et al. Measures of physical performance capture the excess disabilty associated with hip pain or knee pain in older persons. J Gerontol A Biol Sci Med Sci. 2009;64:1316–1324. doi: 10.1093/gerona/glp125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Eggermont LHP, Bean JF, Guralnik JM, et al. Comparing pain severity versus pain location in the MOBILIZE Boston Study: Chronic pain and lower extremity function. J Gerontol A Biol Sci Med Sci. 2009;63A:1393–1398. doi: 10.1093/gerona/glp016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bombard JM, Powell KE, Martin LM, et al. Validity and reliability of self-reported arthritis: Georgia senior centers, 2000-2001. Am J Prev Med. 2005;28:251–258. doi: 10.1016/j.amepre.2004.12.004. [DOI] [PubMed] [Google Scholar]
- 30.Martin LM, Leff M, Calonge N, et al. Validation of self-reported chronic conditions and health services in a managed care population. Am J Prev Med. 2000;18:215–218. doi: 10.1016/s0749-3797(99)00158-0. [DOI] [PubMed] [Google Scholar]
- 31.Goldman N, Lin IF, Weinstein M, et al. Evaluating the quality of self-reports of hypertension and diabetes. J Clin Epidemiol. 2003;56:148–154. doi: 10.1016/s0895-4356(02)00580-2. [DOI] [PubMed] [Google Scholar]
- 32.Kehoe R, Wu SY, Leske MC, et al. Comparing self-reported and physician-reported medical history. Am J Epidemiol. 1994;139:813–818. doi: 10.1093/oxfordjournals.aje.a117078. [DOI] [PubMed] [Google Scholar]
- 33.Indian Health Service. Regional Differences in Indian Health, 2002 - 2003. Department of Health and Human Services; Washington, D.C.: 2009. [Google Scholar]
- 34.Cesari M, Kritchevsky SB, Newman AB, et al. Added value of physical performance measures in predicting adverse health-related events: Results from the Health, Aging and Body Composition Study. J Am Geriatr Soc. 2009;57:251–259. doi: 10.1111/j.1532-5415.2008.02126.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Stevens J, Mack K, Paulozzi L, et al. Self-reported falls and fall-related injuries among persons aged ≥65 years-United States, 2006. J Saf Res. 2008;39:345–349. doi: 10.1016/j.jsr.2008.05.002. [DOI] [PubMed] [Google Scholar]