

Abstract
Objective:
To determine the time to efficacy onset of glatiramer acetate (GA) 40 mg/mL 3-times-weekly formulation (GA40).
Methods:
This post hoc analysis of data from the 1-year, double-blind, placebo-controlled phase of the Glatiramer Acetate Low-Frequency Administration study (NCT01067521) of GA40 in patients with relapsing-remitting MS (RRMS) sought to determine the timing of efficacy onset using a novel data-censoring approach.
Results:
Compared with placebo-treated patients, those receiving GA40 exhibited a >30% reduction in the accumulated annualized relapse rate (ARR) within 2 months of initiating treatment and generally sustained this treatment difference during the 1-year study. Similarly, the proportion of GA40-treated patients who remained relapse-free was distinctly greater by month 2 and continued to increase up to a 10.8% difference at the end of the study. In addition, GA40 treatment was associated with a significant reduction in the number of gadolinium-enhancing T1 lesions and new/enlarging T2 lesions by month 6, with full treatment effect observed after 1 year.
Conclusions:
GA40 contributes to efficacy within 2 months of the start of treatment in patients with RRMS. These results are consistent with the observed time to efficacy onset for patients treated with GA 20 mg/mL daily in previous randomized, placebo-controlled clinical trials.
Classification of evidence:
This study provides Class II evidence that for patients with RRMS, a 3-times-weekly formulation of GA 40 mg/mL leads to a >30% reduction in the ARR within 2 months.
Glatiramer acetate (GA) is a first-line disease-modifying therapy (DMT) approved for the treatment of relapsing-remitting MS (RRMS), with more than 2 million patient-years of overall exposure to date.1,2 Before the 2014 approval of the GA 40 mg/mL formulation, administered by 3-times-weekly SC injection (GA40), GA was available exclusively as a once-daily 20 mg/mL SC injection (GA20).2 Across 5 randomized controlled clinical trials, GA20 has consistently demonstrated efficacy in reducing relapse rate and MRI disease activity and slowing of disability progression in patients with RRMS, while possessing a favorable and well-characterized safety record in both short- and long-term studies.3–11 In pivotal placebo-controlled trials, GA20 treatment was associated with a 29% reduction in the relapse rate (p = 0.007 vs placebo) and a 33% reduction in the total number of enhancing lesions (p = 0.003 vs placebo).6,9
The Glatiramer Acetate Low-Frequency Administration (GALA) study was a phase III trial undertaken to assess the efficacy and safety of GA40 in patients with RRMS over a 1-year period.12 Patients treated with GA40 in the GALA study experienced a 34.4% reduction in the annualized relapse rate (ARR) compared with patients receiving placebo (p < 0.0001), and significant reductions were also observed with GA40 for the cumulative number of gadolinium-enhancing (GdE) T1 lesions (44.8% reduction, p < 0.0001) and new/enlarging T2 lesions (34.7% reduction, p < 0.0001).12 Although GA20 is associated with high rates of both treatment efficacy and treatment adherence,13 the GA40 formulation offers reduced rates of injection-related adverse events (AEs) and injection-site reactions (ISRs) compared with GA20,2,14 which can potentially lead to improvements in treatment tolerability, adherence, and clinical outcomes. GA40 was well tolerated, with a low rate of AEs, consistent with the GA20 safety profile. ISRs were the most common AE, the majority of which were of mild or moderate severity.12
With regard to promptness of efficacy, the interval between treatment initiation and the detection of a treatment effect may be an important factor in treatment selection. The 9003 European/Canadian study, which conducted monthly MRIs, demonstrated a statistically significant treatment effect with GA20 vs placebo in the number of total enhancing lesions per participant starting as soon as 6 months after treatment initiation.6 The purpose of this post hoc analysis of results from the GALA study is to determine the timing of efficacy onset of GA40 during the 1-year placebo-controlled phase of the study.
METHODS
Study design and procedures.
The GALA study was a randomized, placebo-controlled, double-blind, parallel-group study conducted at 142 sites in 17 countries.12 The study design, eligibility criteria, and conduct of the double-blind, placebo-controlled phase of the GALA study have been previously reported.12 In brief, patients were eligible for inclusion if they were aged 18–55 years, had an RRMS diagnosis based on the Revised McDonald Criteria, scored ≤5.5 on the Expanded Disability Status Scale (EDSS), were relapse-free for ≥30 days, had ≥1 documented relapse in the 12 months preceding screening, and either ≥2 documented relapses in the 24 months before screening or 1 documented relapse 12–24 months before screening with ≥1 documented T1 GdE lesion.12
Eligible patients were randomized 2:1 to receive GA40 (n = 943) or placebo (n = 461) during the 7 scheduled visits: at screening, baseline (month 0), and months 1, 3, 6, 9, and 12 (figure 1). Patients underwent a complete neurologic assessment, including EDSS and functional system assessment, at screening, baseline, and months 3, 6, 9, and 12. MRI assessments were conducted at baseline and months 6 and 12. Safety assessment included recording of all AEs, in addition to the performance of standard clinical laboratory tests, vital signs, and electrocardiograph (ECG) measurements. Eligible patients completing the 1-year placebo-controlled, double-blind phase were invited to participate in an open-label extension.12
Figure 1. GALA study design.

*Only clinical visits involving complete neurologic and physical examination are represented in this figure. GA40 = glatiramer acetate 40 mg/mL 3-times-weekly SC injection; R = randomization.
Standard protocol approvals, registrations, and patient consents.
All institutional review boards or ethics committees of the participating centers approved the protocol, and all patients provided written informed consent before any study-related procedures were performed. The GALA study (clinicaltrials.gov; NCT01067521) was conducted in accordance with good clinical practice and International Conference on Harmonization guidelines. Study progress was overseen by an independent data-monitoring committee.
End points.
The primary end point for the GALA study was ARR, based on the total number of confirmed relapses over the course of the 1-year study period among the intent-to-treat (ITT) population, which comprised all patients randomized to receive GA40 or placebo.12 The definition of relapse was the appearance of ≥1 new or previously observed neurologic abnormalities, lasting ≥48 hours and immediately preceded by an improvement in neurologic state lasting ≥30 days from the onset of the previous relapse. Furthermore, an event was considered a relapse if symptoms were accompanied by neurologic changes consistent with a ≥0.5-point increase in the EDSS score compared with the previous evaluation, if ≥2 of the 7 functional system assessments yielded an increase of 1 grade in scoring, or a 2-grade score increase in a single functional system assessment.12 Secondary end points included the number of new or newly enlarging T2 lesions, number of GdE T1 lesions, and percent brain volume change. Exploratory end points included the time to first relapse, proportion of relapse-free patients, number of severe confirmed relapses, and time to 6-month confirmed disability progression. Safety was assessed by the incidence of AEs and serious AEs, changes in vital signs, clinical laboratory parameters, and ECG findings over time.12
Post hoc statistical analyses.
Calculating accumulating ARR.
As a descriptive measure, the ARR can be calculated as the number of confirmed relapses divided by the annual exposure to the drug, i.e., the number of relapses in the population divided by the number of years of exposure. ARR, it should be noted, can be calculated at any time point in the study. To calculate the accumulating ARR for the present analysis, the relapse data were censored at each study day and the statistic was estimated. The accumulating ARR at a given study day for a treatment group is therefore calculated as the total number of relapses that occurred in that group on or prior to the study day of interest divided by the corresponding number of patient-years of exposure up to the study day. The accumulating ARR at the last study day is therefore equivalent to the typical ARR presented as the primary study end point. The resulting statistics calculated at each study day provide a description of the estimated relapse rate over time and more specific insights into the timing of efficacy on relapses.
Additional analytic methods.
The percentage of patients experiencing confirmed relapses was calculated using Kaplan-Meier methodology. Reductions in the numbers of GdE T1 and new or newly enlarging T2 lesions were analyzed separately at months 6 and 12 using a negative-binomial model. Covariates used in this model included the interaction of visit and treatment group, number of GdE T1 lesions at baseline, and country or geographic region.
Classification of evidence.
This article answers the question of the timing of efficacy onset of GA40 for patients with RRMS, based on the phase III GALA study. This study provides Class II evidence that for patients with RRMS, a 3-times-weekly formulation of GA40 mg/mL leads to a >30% reduction in the ARR within 2 months.
RESULTS
Patients.
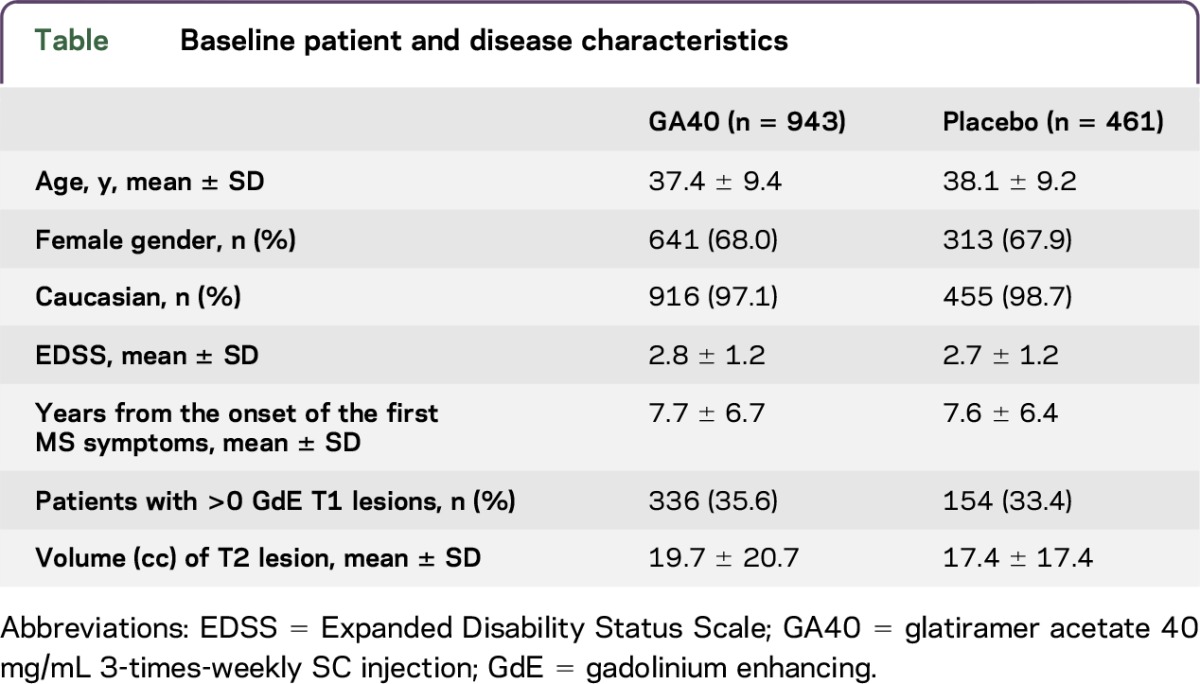
The baseline demographics and disease characteristics of the GALA ITT population are shown in the table. There are no significant differences between the 2 groups. Approximately two-thirds of the patient population were female, with an average of approximately 7.7 years since the onset of MS symptoms.
Table.
Baseline patient and disease characteristics
Clinical outcomes.
The pattern of accumulating ARR over the course of 1 year of the GALA study shows an early treatment effect with GA40 and separation between groups (figure 2). Within 2 months of treatment initiation, patients receiving GA40 exhibited an ARR reduction of >30% vs patients receiving placebo. Despite early fluctuations in accumulating ARR, this separation between GA40 and placebo was generally sustained for the rest of the analysis period, with 28.7% ARR reduction at month 6 and 33.4% ARR reduction at the end of the study.
Figure 2. Accumulating annualized relapse rate.

Accumulating ARR is not adjusted for baseline characteristics. ARR = annualized relapse rate; GA40 = glatiramer acetate 40 mg/mL 3-times-weekly SC injection.
Differences in the proportion of participants in the GA40 and placebo groups who remained relapse-free showed separation within 2 months of treatment initiation (figure 3). At the 6-month time point, the difference seen at 2 months had more than doubled, and by the end of 1 year, the difference in proportion of relapse-free participants in the GA40 group was nearly 11% less than that seen in the placebo group.
Figure 3. Proportion of patients with a confirmed relapse in the GALA study.

GA40 = glatiramer acetate 40 mg/mL 3-times-weekly SC injection.
GA40-treated patients demonstrated a reduced number of GdE T1 lesions and new/enlarging T2 lesions compared with placebo at 6 months (figure 4). At month 6 of the GALA study, GA40 was associated with a 38.0% reduction (p = 0.001) in the number of GdE T1 lesions and a 24.2% reduction (p = 0.0050) in the number of new/enlarging T2 lesions vs placebo. By the end of the study, at month 12, the treatment effect was further pronounced, with 52.5% and 47.3% difference in lesion counts (p < 0.0001, both), respectively. Thus, a significant treatment effect of MRI disease activity was observed by month 6, with the full treatment effect of GA40 observed at the end of the study.
Figure 4. MRI lesion activity in the GALA study.

GA40 = glatiramer acetate 40 mg/mL 3-times-weekly SC injection; GdE = gadolinium enhancing; SE = standard error.
DISCUSSION
This post hoc analysis of data from the phase III GALA clinical trial demonstrates that, compared with placebo, GA40 treatment in patients with RRMS provided notable improvements in accumulating ARR and lengthening of time to first relapse within 2 months of treatment initiation. MRI outcomes were observed to be significantly different between GA40-treated and placebo-treated patients at the 6-month time point, which was the first MRI conducted after baseline in the GALA study. The relevance of establishing the time to efficacy onset of a DMT in MS derives from the importance of early intervention and the need for rapid therapeutic efficacy in minimizing MRI disease activity and the frequency of relapses.1,15–17
ARR is the most common method for reporting relapse end points in RRMS trials, in part due to its ease of quantification—and thus transparency—and also because of the explicit benefit to patients of a reduction in relapses.18 However, ARR values are derived from a cumulative relapse count over the course of a trial and therefore obscure time-dependent effects that may be relevant. By contrast, the use of the accumulating ARR end point in this analysis has the specific advantage of displaying the time course of ARR over the length of the entire GALA trial. The rationale for the present analysis was to establish a clear picture of the time to efficacy onset for GA using data from a controlled clinical trial. In addition, ascertaining temporal aspects of relapse-related efficacy allows for a qualitative comparison with additional pharmacologic effects over time, such as the accumulation of MRI lesions. The accumulating ARR metric will be useful to analyze the time course of efficacy on relapses in future MS clinical trials with a relapse end point.
The results reported herein show that GA40 has a relatively rapid time to efficacy onset in patients with RRMS, with potential implications for disease management and both short- and long-term clinical and MRI outcomes. The key limitation of this study is the post hoc nature of the analysis because calculating the accumulating ARR and analyzing MRI separately at the 6- and 12-month time points were not the stated end points in the GALA study.
While the efficacy and safety profiles of GA20 and GA40 have been extensively studied, the question of the time to efficacy onset has been much less explored. Prior to this analysis, the only previous study that evaluated the time to efficacy onset in GA treatment of patients with RRMS was the 9003 European/Canadian study of GA20, which was specifically designed to evaluate MRI at frequent intervals, with scans being performed every month during the 9-month placebo-controlled phase of the study.6,19,20 Although the 9003 study was conducted well before the development of the GA40 formulation, it offers the best data source for a comparison with the results of our analysis of the time to efficacy onset in the GALA study. Of course, direct comparisons of 2 separate studies must be approached with caution, and no definitive conclusions based on such a comparison are entirely reliable. Nevertheless, the GALA and 9003 studies had similar designs and patient eligibility criteria.6,12 MRI lesion activity among patients receiving daily GA20 or placebo in the 9003 study showed separation between the 2 groups by month 2: the mean number of total enhancing lesions at month 2 was 19.4% lower in the GA20-treated group compared with the placebo-treated group. By month 6, a significant difference had been achieved, with 35.9% fewer enhancing lesions in the GA20 group (p < 0.01). The differences were even greater at month 8 (49.7%, p < 0.001) and month 9 (40.1%, p < 0.02).6,21 Taken together, these results parallel those seen in our analysis of the GALA data. Although approximately 36% less lesion activity was observed among GA20-treated patients in the 9003 study at month 6, the number of GdE T1 lesions was reduced by 38% after 6 months in the GALA study, whereas new and newly enlarging T2 lesions were reduced by approximately 24% among those treated with GA40; these differences were, in all cases, statistically significant in favor of GA therapy. In addition, results after 9 months of GA20 treatment in the 9003 study (which, of course, are not directly comparable with 6-month data) show the number of T1 lesions to have been reduced by 35%, while new T2 lesions (not including enlarging T2 lesions) were reduced by 30%, differences that were statistically significant in both cases.6
This post hoc analysis of results from the GALA study shows an improvement with regard to the development of new or newly enlarging lesions as detected by MRI in patients treated with GA40 compared with those receiving placebo; this improvement occurred early, within 2 months of the start of treatment, and was generally sustained throughout the trial. With regard to occurrence of relapses in RRMS, the use of the accumulating ARR metric provides clinically meaningful insight into the time course of the efficacy of GA. The efficacy of GA40 in reducing numbers of MRI inflammatory lesions occurred by 6 months in the GALA study, an effect similar to that previously seen in the 9003 study of GA20. These results indicate that GA40 contributes to early efficacy in RRMS through the reduction of inflammatory lesions and relapses.
ACKNOWLEDGMENT
The authors thank the patients and site personnel involved with this study; and Peter Feldman, PhD (Teva Pharmaceutical Industries) and Rhonda Charles, PhD (Chameleon Communications International with funding from Teva Pharmaceutical Industries) for editorial assistance in the preparation of this article.
GLOSSARY
- AE
adverse event
- ARR
annualized relapse rate
- DMT
disease-modifying therapy
- ECG
electrocardiograph
- EDSS
Expanded Disability Status Scale
- GA
glatiramer acetate
- GALA
Glatiramer Acetate Low-Frequency Administration
- GdE
gadolinium enhancing
- ISR
injection-site reaction
- ITT
intent to treat
- RRMS
relapsing-remitting MS
AUTHOR CONTRIBUTIONS
Mat D. Davis: design and conceptualization of the study; analysis and interpretation of the data; and drafting and revising the manuscript for intellectual content. Natalia Ashtamker and Joshua R. Steinerman: analysis and interpretation of the data and drafting and revising the manuscript for intellectual content. Volker Knappertz: design and conceptualization of the study; analysis and interpretation of the data; and drafting and revising the manuscript for intellectual content.
STUDY FUNDING
This study was funded by Teva Pharmaceutical Industries, Petach Tikva, Israel.
DISCLOSURE
M.D. Davis is employed by and owns stock or stock options in Teva Pharmaceuticals. N. Ashtamker is employed by and received research support from Teva Pharmaceuticals. J.R. Steinerman served on the data safety monitoring board for an NIH-sponsored study, is employed by Teva Pharmaceuticals, has consulted for Click Therapeutics, and holds stock or stock options in Teva Pharmaceuticals and Click Therapeutics. V. Knappertz is employed by Teva Pharmaceuticals and holds stock and stock options in Teva and Knopp Biosciences. Go to Neurology.org/nn for full disclosure forms.
REFERENCES
- 1.Boster AL, Ford CC, Neudorfer O, Gilgun-Sherki Y. Glatiramer acetate: long-term safety and efficacy in relapsing-remitting multiple sclerosis. Expert Rev Neurother 2015;15:575–586. [DOI] [PubMed] [Google Scholar]
- 2.Copaxone [Prescribing Information]. Overland Park, KS: TEVA Neuroscience, Inc.; 2014. [Google Scholar]
- 3.Arnal-Garcia C, Amigo-Jorrin Mdel C, Lopez-Real AM, et al. Long-term effectiveness of glatiramer acetate in clinical practice conditions. J Clin Neurosci 2014;21:2212–2218. [DOI] [PubMed] [Google Scholar]
- 4.Debouverie M, Moreau T, Lebrun C, Heinzlef O, Brudon F, Msihid J. A longitudinal observational study of a cohort of patients with relapsing-remitting multiple sclerosis treated with glatiramer acetate. Eur J Neurol 2007;14:1266–1274. [DOI] [PubMed] [Google Scholar]
- 5.Rovaris M, Codella M, Moiola L, et al. Effect of glatiramer acetate on MS lesions enhancing at different gadolinium doses. Neurology 2002;59:1429–1432. [DOI] [PubMed] [Google Scholar]
- 6.Comi G, Filippi M, Wolinsky JS. European/Canadian multicenter, double-blind, randomized, placebo-controlled study of the effects of glatiramer acetate on magnetic resonance imaging–measured disease activity and burden in patients with relapsing multiple sclerosis. European/Canadian Glatiramer Acetate Study Group. Ann Neurol 2001;49:290–297. [PubMed] [Google Scholar]
- 7.Filippi M, Rovaris M, Rocca MA, Sormani MP, Wolinsky JS, Comi G. Glatiramer acetate reduces the proportion of new MS lesions evolving into “black holes.” Neurology 2001;57:731–733. [DOI] [PubMed] [Google Scholar]
- 8.Johnson KP, Brooks BR, Cohen JA, et al. Extended use of glatiramer acetate (Copaxone) is well tolerated and maintains its clinical effect on multiple sclerosis relapse rate and degree of disability. Copolymer 1 Multiple Sclerosis Study Group. Neurology 1998;50:701–708. [DOI] [PubMed] [Google Scholar]
- 9.Johnson KP, Brooks BR, Cohen JA, et al. Copolymer 1 reduces relapse rate and improves disability in relapsing-remitting multiple sclerosis: results of a phase III multicenter, double-blind placebo-controlled trial. The Copolymer 1 Multiple Sclerosis Study Group. Neurology 1995;45:1268–1276. [DOI] [PubMed] [Google Scholar]
- 10.Mikol DD, Barkhof F, Chang P, et al. Comparison of subcutaneous interferon beta-1a with glatiramer acetate in patients with relapsing multiple sclerosis (the REbif vs Glatiramer Acetate in Relapsing MS Disease [REGARD] study): a multicentre, randomised, parallel, open-label trial. Lancet Neurol 2008;7:903–914. [DOI] [PubMed] [Google Scholar]
- 11.O'Connor P, Filippi M, Arnason B, et al. 250 microg or 500 microg interferon beta-1b versus 20 mg glatiramer acetate in relapsing-remitting multiple sclerosis: a prospective, randomised, multicenter study. Lancet Neurol 2009;8:889–897. [DOI] [PubMed] [Google Scholar]
- 12.Khan O, Rieckmann P, Boyko A, Selmaj K, Zivadinov R, Group GS. Three times weekly glatiramer acetate in relapsing-remitting multiple sclerosis. Ann Neurol 2013;73:705–713. [DOI] [PubMed] [Google Scholar]
- 13.Oleen-Burkey M, Cyhaniuk A, Swallow E. Retrospective US database analysis of persistence with glatiramer acetate vs. available disease-modifying therapies for multiple sclerosis: 2001–2010. BMC Neurol 2014;14:11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wolinsky JS, Borresen TE, Dietrich DW, et al. GLACIER: an open-label, randomized, multicenter study to assess the safety and tolerability of glatiramer acetate 40mg three-times weekly versus 20 mg daily in patients with relapsing-remitting multiple sclerosis. Mult Scler Relat Disord 2015;4:370–376. [DOI] [PubMed] [Google Scholar]
- 15.Zivadinov R, Dwyer M, Barkay H, Steinerman JR, Knappertz V, Khan O. Effect of glatiramer acetate three-times weekly on the evolution of new, active multiple sclerosis lesions into T1-hypointense “black holes”: a post hoc magnetic resonance imaging analysis. J Neurol 2015;262:648–653. [DOI] [PubMed] [Google Scholar]
- 16.Caporro M, Disanto G, Gobbi C, Zecca C. Two decades of subcutaneous glatiramer acetate injection: current role of the standard dose, and new high-dose low-frequency glatiramer acetate in relapsing-remitting multiple sclerosis treatment. Patient Prefer Adherence 2014;8:1123–1134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Edan G, Kappos L, Montalban X, et al. Long-term impact of interferon beta-1b in patients with CIS: 8-year follow-up of BENEFIT. J Neurol Neurosurg Psychiatry 2014;85:1183–1189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lavery AM, Verhey LH, Waldman AT. Outcome measures in relapsing-remitting multiple sclerosis: capturing disability and disease progression in clinical trials. Mult Scler Int 2014;2014:262350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Comi G, Cohen JA, Arnold DL, Wynn D, Filippi M. Phase III dose-comparison study of glatiramer acetate for multiple sclerosis. Ann Neurol 2011;69:75–82. [DOI] [PubMed] [Google Scholar]
- 20.Cohen JA, Rovaris M, Goodman AD, Ladkani D, Wynn D, Filippi M. Randomized, double-blind, dose-comparison study of glatiramer acetate in relapsing-remitting MS. Neurology 2007;68:939–944. [DOI] [PubMed] [Google Scholar]
- 21.Teva Pharmaceutical Industries. Data on File.