

Abstract
Extracorporeal membrane oxygenation (ECMO) refers to specific mechanical devices used to temporarily support the failing heart and/or lung. Technological advances as well as growing collective knowledge and experience have resulted in increased ECMO use and improved outcomes. Veno-arterial (VA) ECMO is used in selected patients with various etiologies of cardiogenic shock and entails either central or peripheral cannulation. Central cannulation is frequently used in postcardiotomy cardiogenic shock and is associated with improved venous drainage and reduced concern for upper body hypoxemia as compared to peripheral cannulation. These concerns inherent to peripheral VA ECMO may be addressed through so-called triple cannulation approaches. Veno-venous (VV) ECMO is increasingly employed in selected patients with respiratory failure refractory to more conventional measures. Newer dual lumen VV ECMO cannulas may facilitate extubation and mobilization. In summary, the pathology being addressed impacts the ECMO approach that is deployed, and each ECMO implementation has distinct virtues and drawbacks. Understanding these considerations is crucial to safe and effective ECMO use.
Keywords: Acute respiratory failure, cardiogenic shock, extracorporeal membrane oxygenation, extracorporeal membrane oxygenation cannulation strategies, triple cannulation
Introduction
Extracorporeal membrane oxygenation (ECMO) falls under the broader heading of extracorporeal life support (ECLS) and refers to specific types of invasive devices that augment, and in severe cases, supplant, native circulation, and/or gas exchange to temporarily support patients experiencing cardiac and/or pulmonary failure, respectively. The first successful application of ECMO in an adult patient was described in 1972.[1] Subsequently, interest in using ECMO in adults waned following a multicenter NIH-sponsored trial showing no mortality benefit in adults with respiratory failure, and it was primarily used to manage respiratory failure in the neonatal and pediatric populations.[2,3] Since then, technical and other advancements have led to the current environment, where ECMO is increasingly utilized as a temporizing measure in selected patients with various etiologies of severe cardiac and/or pulmonary dysfunction.
In general terms, an ECMO circuit is a closed system comprised a venous drainage cannula, pump, control console, oxygenator, blender, heater/cooler, and a return cannula. As detailed in the following text, the condition being treated impacts the specific ECMO cannulation strategy employed, which in turn confers certain advantages, limitations, and considerations. Finally, it must be noted that this review is based largely on expert opinion, case reports, case series, and retrospective analyses. Given the nature of the technology and the patients in whom it is applied, there are few prospective studies regarding ECMO.
Nomenclature
As described in the following text, ECMO has its own lexicon and set of acronyms. By convention, the terms inflow (in this context, synonymous with drainage and afferent) and outflow (synonymous with return and efferent) refer to the direction of blood flow relative to the pump, not the patient.
Veno-arterial Extracorporeal Membrane Oxygenation
Veno-arterial (VA) ECMO is a form of mechanical circulatory support where the ECMO circuit functions in parallel to the native heart and lungs. In VA ECMO, the return cannula resides in the arterial system, and the size and location of the venous and arterial cannulas impact tissue oxygenation as well as the degree of cardiac support provided.
Central versus Peripheral Cannulation
As depicted in Figure 1, there are two principle VA ECMO configurations: Central and peripheral. Central cannulation [Figure 1a] generally refers to drainage of venous blood through a cannula placed in the right atrium (RA) and an arterial cannula inserted into the ascending aorta; these cannulas can be tunneled to permit chest closure. In contrast, peripheral cannulation [Figure 1b] entails drainage of venous blood from the infrahepatic inferior vena cava (IVC) through a cannula that exits the femoral vein or, if needed, more complete drainage using a long 21–25 Fr multistage cannula inserted in the femoral vein with its tip in the RA. Less commonly, the right internal jugular (IJ) vein may also be used, with either a single lumen or a two-stage bicaval cannula.[4,5] Typically, the arterial cannula is a short 17–21 Fr catheter placed in the femoral artery with the tip in the common iliac artery. Alternatively, arterial blood can also be returned using an end-to-side graft to the right subclavian or axillary artery.[6,7]
Figure 1.

Basic veno-arterial extracorporeal membrane oxygenation configurations. (a) Central veno-arterial extracorporeal membrane oxygenation with the venous cannula exiting the right atrium and the arterial cannula entering the ascending aorta. (b) Peripheral veno-arterial extracorporeal membrane oxygenation with a venous cannula exiting the femoral vein and the arterial cannula entering the femoral artery with the tip in the common iliac artery
Central cannulation is frequently used in postcardiotomy cardiogenic shock.[8] It employs cannulas already in place for typical cardiopulmonary bypass (CPB). The short, large-bore venous cannulas used during CPB permit adequate venous drainage and typically allow for greater cardiac decompression than in peripheral cannulation. In addition, as oxygenated blood is returned to the ascending aorta, there is less concern for retrograde flow and upper body hypoxemia. A key disadvantage of central cannulation is that it requires entering the chest for initiation and discontinuation of ECMO. As such, central cannulation confers increased risk of bleeding, surgical re-exploration, and mediastinitis.[9,10] Furthermore, central cannulation generally precludes extubation and patient mobilization, both of which have been reported with certain peripheral approaches.[11]
The main advantages of peripheral cannulation are the ease of cannulation, either through Seldinger technique or cut down, and the lack of need for surgery. Peripheral VA ECMO cannulation is often done bedside and can even be accomplished in patients undergoing chest compressions. Disadvantages include upper body hypoxemia, aortic root thrombus formation, left ventricular distension, and lower extremity ischemia. Furthermore, femoral cannulation may not be feasible in patients with significant peripheral vascular disease.
Differential Hypoxemia in Peripheral Veno-arterial Extracorporeal Membrane Oxygenation
The so-called Harlequin, or North-South, syndrome occurs due to differential hypoxemia between the upper body and lower body in peripherally cannulated VA ECMO patients with concomitant lung failure or ventilator mismanagement. This is a result of the mixing cloud or watershed that forms in the aorta when retrograde oxygenated blood from the femoral arterial cannula joins undrained blood from the RA that transits the pulmonary vasculature and is ejected from the left ventricle (LV). Depending on native lung function, volume status, and cardiac function, blood ejected from the LV may be poorly oxygenated, and this blood may mal-perfuse the coronary arteries and cerebral circulation.[12]
This watershed may in turn lead to a persistent dual circuit circulation. Here, the upper body is perfused with poorly oxygenated blood that cycles from the heart to the upper body to the superior vena cava (SVC) and back into the heart but never enters the ECMO circuit. Well-oxygenated blood from the ECMO circuit perfuses the lower body and reenters the ECMO circuit through the IVC. An animal model of dual circuit circulation, in which femoral VA ECMO was applied to sheep in respiratory failure, showed that oxygen saturation in the SVC, pulmonary artery, and ascending aorta ranged from 33% to 40% while it was 84% in the IVC.[13,14]
Detection of differential hypoxemia and its treatment requires meticulous attention through frequent blood gas monitoring from a right upper extremity arterial line. It is particularly relevant in femorally cannulated patients with poor lung function and marked pulsatility, which indicates significant ejection of blood from the LV. It is generally not an issue with central or subclavian arterial cannulation as oxygenated blood easily reaches the arch vessels in these situations.
Alternative Configurations of Peripheral Veno-arterial Extracorporeal Membrane Oxygenation
Various strategies have been described to mitigate specific limitations of peripheral VA ECMO. Veno-veno-arterial ECMO [VVA ECMO; Figure 2a] refers to insertion of an additional venous drainage cannula, typically into the right IJ vein. This may be indicated in patients with significant LV distention due to inadequate drainage or certain intracardiac shunts as well as in patients where small vessel caliber prevents insertion of larger bore drainage cannulas. The two drainage cannulas are joined through a Y-connector. Of note, there is no consensus nomenclature for such triple cannula ECMO configurations, and VVA ECMO has also been used to describe the addition of an arterial outflow cannula to patients on veno-venous (VV) ECMO that develop cardiac failure, specifically of the right ventricle (RV).[15]
Figure 2.
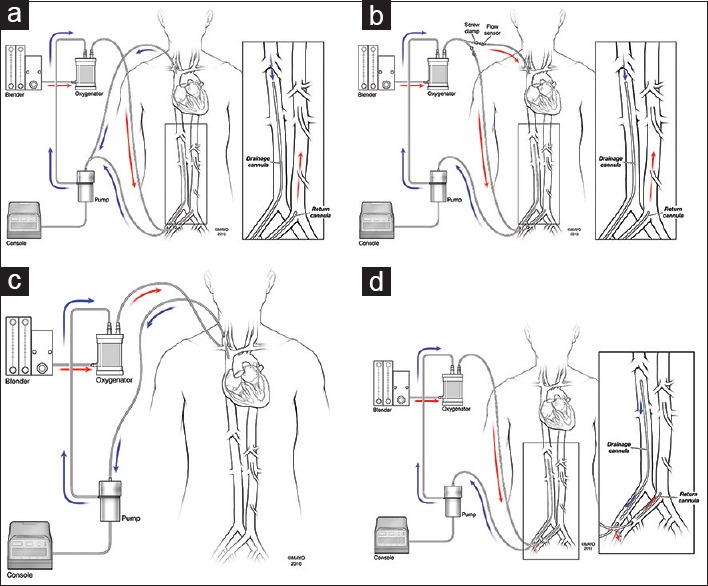
Alternative peripheral veno-arterial extracorporeal membrane oxygenation configurations. (a) Veno-veno-arterial extracorporeal membrane oxygenation with two venous drainage cannulas joined by a Y-connector. (b) Veno-arterial-venous extracorporeal membrane oxygenation with an additional venous cannula conveying oxygenating blood. Please note the screw clamps and flow sensors on the two efferent limbs. (c) Upper body cannulation using the right internal jugular vein and right subclavian or axillary artery. (d) A distal perfusion catheter may be used to maintain perfusion distal to the arterial cannula in the ipsilateral lower extremity
Veno-arteriovenous ECMO [VAV ECMO; Figure 2b] has been used in peripherally cannulated patients with significant heart and lung dysfunction.[16] Here, part of the arterial outflow is directed toward the RA, providing mechanical circulatory and respiratory support. Oxygenated blood can be returned to the venous system through a distinct cannula inserted into the SVC, in which case the two venous cannulas should be positioned at the cava-right atrial junctions, as in VV ECMO, or through the efferent lumen of a dual lumen cannula while drainage is achieved through the afferent lumen. The relative flows of the two outflow limbs (arterial and oxygenated venous) are modulated using adjustable clamps and flow sensors and must be carefully regulated as each change will impact preload, afterload, oxygenation, and location of the watershed.[15]
Interestingly, animal data suggest that VVA ECMO may also be used to treat upper body hypoxemia. This is thought to be due to disruption of two circuit circulation although the ensuing decrease in intrinsic cardiac output from increased venous drainage may also result in reduced ejection of poorly oxygenated blood and hence a more proximal location of the watershed in the aorta.[13] Alternative measures to address differential hypoxemia include ventilator optimization or more proximal aortic perfusion through either insertion of a longer arterial cannula into the aorta, insertion of an outflow graft into the subclavian artery, or central cannulation.
As mentioned above, subclavian or axillary artery cannulation may be used for the return of oxygenated blood. This is generally achieved through an end-to-side anastomosis using a Dacron® graft. As with ascending aortic cannulation, arterial return here reduces concern for root thrombus and upper body hypoxemia. A further advantage is that upper body cannulation, achieved using the right IJ vein and the right axillary or subclavian artery [Figure 2c], may permit patient mobilization.[11] Potential complications of this approach are highlighted in a cases series from Columbia University Medical Center (New York, USA), in which three out of twenty VA ECMO patients required conversion from subclavian to femoral artery outflow due to one case each of hematoma, infection, and arm swelling.[17]
Lower extremity ischemia, ipsilateral and distal to the arterial cannula site, is also a risk with peripheral VA ECMO. In fact, a meta-analysis of 1866 VA ECMO patients reports a 16.9% incidence of lower extremity ischemia, fasciotomy or compartment syndrome in 10.3%, and amputation in 4.7%.[18] Some centers routinely place a distally directed 6–10 Fr catheter in the cannulated limb [Figure 2d]. This distal perfusion cannula is connected to the arterial outflow of the ECMO circuit and is associated with decreased limb ischemia.[19] Risk factors for distal ischemia include the use of larger bore cannulas as well as peripheral vascular disease.[20] Of note, weaning VA ECMO flow will also decrease flow through the distal perfusion cannula such that ischemia may result from a prolonged duration of low ECMO flow despite the presence of a distal perfusion catheter.
Other Considerations
Regardless of VA ECMO configuration, maintaining some degree of pulsatility is important to decrease the incidence of intracardiac or aortic root thrombus as well as to reduce LV distention. Intracardiac or aortic root thrombus is dangerous due to the risk of embolus and occlusion of the coronary ostia. LV distension results in increased LV wall tension and ischemia as well as mitral regurgitation, left atrial hypertension, and pulmonary edema. Patients with poor contractility are at high risk for both thrombus formation and LV distension. Back pressure from blood exiting the femoral cannula opposes LV ejection and thus increases LV afterload, predisposing to blood stagnating in the LV and aortic root. In addition, blood arriving from transpulmonary flow that is not ejected will cause LV distention independent of any concomitant aortic insufficiency, particularly if there is a marked improvement in RV but not LV function.
As such, most ECMO centers will use inotropes to maintain some degree of pulsatility, often 10–20 mmHg, to decrease LV distension and thrombus formation, both of which may be detected through echocardiography. There are multiple reports of successful LV decompression using a transaortic pigtail drain. Although venting of the left atrium, through atrial septostomy or otherwise, will reduce pulmonary edema, it is debatable if this will also reduce LV distention in the absence of significant mitral regurgitation. IABP insertion may reduce LV afterload but will not directly reduce LV distention. Insertion of an Impella® 2.5 device (Abiomed Inc., Danvers MA, USA) is another effective, albeit expensive, means of decompressing the LV.[21] Surgical LV venting is also commonly employed. In fact, there is a report of converting an LV apical drain into a short-term left ventricular assist device (LVAD) inflow cannula in peripheral VA ECMO patients that require prolonged support. One virtue of this approach is that this conversion can be done without reentering the chest.[22]
Cannula Sizing
The main determinants of cannula sizing in VA ECMO are anatomical considerations and the targeted flow rate. Generally, cannulas are chosen to support a flow equivalent to a cardiac index of 2.2–2.5 L/m2/min, which is considered full flow. Arterial cannulas are typically 15–25 Fr and venous cannulas are usually 19–25 Fr.[23] Kohler et al. provide a thorough review of the physics underlying cannula selection.[24] As noted in their review, the intent of appropriate cannula choice is to provide full flow without damaging cells, particularly erythrocytes, from excessive shear stress and turbulence. In addition to small diameter, kinks, side hole occlusion or reduced number of side holes, and increased cannula length, all increase impedance. In contrast to venous cannulas, arterial cannulas tend to be smaller but shorter to provide less resistance to flow.
Large arterial cannulas can be more difficult to place during emergency settings and may be associated with increased incidence of limb ischemia due to vessel occlusion. There is some evidence that smaller arterial cannulas (15 Fr) may result in adequate cardiac support as assessed through hemodynamic and laboratory parameters with a significant decrease in bleeding at the cannulation site. However, these data are difficult to interpret given small sample size and increased Impella® 2.5 use in the small cannula group.[25]
Veno-arterial Extracorporeal Membrane Oxygenation Compared to Right Ventricular Assist Device
As described above, a typical VA ECMO circuit will drain blood from the RA and return blood to the aorta, bypassing the heart and the pulmonary circulation. Right ventricular assist devices (RVADs), which are often used to address right ventricular failure after implantation of LVADs or orthotopic heart transplantation, drain blood from the RA and return blood, with or without first passing through a membrane oxygenator, to the pulmonary artery, generally through a Dacron® graft anastomosed to the pulmonary artery.[23]
Although both VA ECMO and RVADs are used to manage acute RV dysfunction, the RVAD may have certain advantages including the ability to wean the oxygenator separately from flow as well as increased duration of support.[26,27] A published case of RV failure following LVAD implantation reported weaning the oxygenator in 3 days while the RVAD remained in situ for 3 weeks.[28] A case series of 45 patients in whom an RVAD was inserted after LVAD insertion describes a mean duration of RVAD therapy of up to 33 days.[26] Transpulmonary flow from an RVAD allows normal LVAD speeds and flows. In addition, a small case series of ten peripheral VA ECMO patients versus eight RVAD patients reports a 60% incidence of thrombotic complications in the ECMO group as opposed to none in the RVAD group.[29] Furthermore, tunneling the Dacron® graft from the pulmonary artery through the subxiphoid area allows the chest to be closed and subsequent RVAD weaning and discontinuation without reoperative sternotomy.[30] In the future, less invasive devices such as the Impella RP™ (Abiomed, Danvers MA, USA) may be increasingly used for short-term RV support.
Veno-venous Extracorporeal Membrane Oxygenation
VV ECMO is an advanced therapy for patients in respiratory failure that is refractory to standard, less invasive therapies. In contrast to VA ECMO, where the ECMO circuit is in parallel to the bypassed organs, VV ECMO exists in series with the lungs. As such, VV ECMO provides no cardiac support, and all organs are exposed to approximately the same oxygen content, which is determined by the relative contributions of the VV ECMO device, native lung function and oxygen extraction, and blood returning from the coronary sinus.[31]
Veno-venous Extracorporeal Membrane Oxygenation Cannulation Strategies
VV ECMO requires deoxygenated venous blood to be withdrawn from the patient, circulated through an oxygenator, and then return of oxygenated and decarboxylated blood to the venous system. The most common cannulation configuration is percutaneous insertion of two cannulas, one inserted into the right IJ vein and the other into either femoral vein [Figure 3a]. This cannulation arrangement relies on a drainage cannula that terminates at or just distal to the RA-IVC junction and a return cannula whose tip lies either at the RA-SVC junction or within the RA.[15,32] This allows deoxygenated blood to be removed from the IVC and oxygenated blood to be returned to the SVC or RA.[33] Femoral-femoral VV ECMO is less commonly employed and involves insertion of a drainage cannula into the IVC 5–10 cm caudal to the IVC-RA junction, and the tip of the return cannula is advanced into the RA through the contralateral femoral vein [Figure 3b]. This arrangement is reportedly associated with a greater incidence of recirculation than femoral-jugular cannulation.[34]
Figure 3.

Common veno-venous extracorporeal membrane oxygenation configurations. (a) Conventional veno-venous extracorporeal membrane oxygenation, where the tip of the drainage cannula lies at the inferior vena cava-right atria junction and the tip of the return cannula is in the right atrium. (b) Femoral-femoral veno-venous extracorporeal membrane oxygenation, where the tip of the drainage cannula is in the infrahepatic inferior vena cava and the tip of the outflow cannula is in the right atrium. (c) The Avalon Elite® veno-venous extracorporeal membrane oxygenation cannula, with bicaval drainage ports and a return port that directs oxygenated blood toward the tricuspid valve
Alternatively, a single dual lumen ECMO cannula can be placed into the right IJ vein. This cannula is frequently referred to as the “Avalon” since the brand name of a popular dual lumen ECMO cannula is the Avalon Elite® (Maquet, Germany). Such a cannula comprised two lumens contained within one 16–31 Fr cannula. This cannula is placed percutaneously into the right IJ vein such that the most distal portion of the cannula rests in the IVC. One lumen drains deoxygenated venous blood from the SVC and IVC through proximal and distal ports, respectively, while the return lumen directs oxygenated blood toward the tricuspid valve [Figure 3c]. Proper function of this cannula requires that the return lumen orifice is situated superior (cranial) to the tricuspid valve, with the orifice oriented toward the tricuspid valve.[35] Positioning the cannula in this manner allows drainage of mainly deoxygenated blood from the SVC and IVC as well as return of mainly oxygenated blood into the RA, where it is then ejected through the heart in standard fashion.
Of note, a novel dual lumen VV ECMO cannula, the Protek Duo (Cardiac Assist, Pittsburgh, PA, USA) received Food and Drug Administration approval in 2014. The Protek Duo is also inserted into the right IJ vein but, in contrast to the Avalon Elite®, the distal tip of this cannula is placed into the main pulmonary artery.[36] Thus, the Protek Duo may decompress the RV in addition to providing gas exchange. At present, this cannula is new and infrequently used and, as such, will not be discussed further in this review.
Recirculation
Under optimal conditions, VV ECMO support will provide sufficient oxygenation to meet the patient's metabolic needs. Recirculation is a limitation of VV ECMO related to cannula position and requisite return and drainage of venous blood. In the context of VV ECMO, recirculation most commonly occurs when one cannula is too close to the other and refers to a situation where oxygenated blood returned from the ECMO circuit to the RA is immediately drained from the RA by the drainage cannula instead of entering the systemic circulation. Alternatively, recirculation may also occur as a result of increased VV ECMO flow as compared to native flow or due to increases in intracardiac or intrathoracic pressure which impede venous return to the heart.[37]
Diagnosing recirculation requires a high index of suspicion and should be considered when VV ECMO initiation does not result in improved oxygenation. Imaging through chest radiography, echocardiography, or fluoroscopy may show close proximity of the drainage and return cannulas. Furthermore, blood from the drainage cannula may have a similar color (“redness”) and partial pressure of oxygen as blood in the tubing of the return cannula. Recirculation is addressed by withdrawing one or both cannulas as appropriate based on imaging, inserting an additional drainage cannula, or using a properly positioned dual lumen cannula.[31]
Dual Lumen Cannula Pro/Con
The Avalon Elite® is the most common dual lumen cannula used in contemporary VV ECMO, and many ECMO centers preferentially insert such catheters as the first choice cannulation technique for VV ECMO if possible. This is because dual lumen catheters for VV ECMO permit single site cannulation in the upper body. This facilitates patient extubation (and reduces the risks inherent to prolonged mechanical ventilation), mobilization, and “pre-habilitation”/rehabilitation, increases patient comfort, and may also decrease the infectious risk of groin cannulation. Sitting the patient up at 30 degrees or greater elevation often prevents insertion site bleeding or oozing. Obviously, mobilization must be done with great care as reported complications include caudad or cephalad cannula migration as well as rotation of the return port away from the tricuspid valve.[35,38] From a mechanical standpoint, the design of the Avalon Elite® allows for bicaval drainage of deoxygenated blood at a considerable distance from the oxygenated blood return orifice. In the optimally positioned Avalon Elite® cannula, this allows for very little recirculation of oxygenated blood into the ECMO circuit when compared to two cannulas (femoral-jugular or femoral-femoral) VV ECMO strategies.[39]
There are several limitations of the Avalon Elite®. The cannula is designed for right IJ vein insertion and so may not be appropriate for patients in whom this vessel cannot accommodate a large bore catheter although there are reports of using the left IJ and subclavian veins.[40,41] Unsurprisingly, for a dual lumen catheter, cannula size limitations may limit ECMO flow and predispose to hemolysis at higher flows.[15] Proper Avalon Elite® cannula deployment involves precise placement of the distal tip into the IVC and correct orientation of the return lumen in relation to the tricuspid valve and requires a team (physician cannulator, perfusionist/ECMO specialist, and sonographer/fluoroscopist) that is available and well versed in this technique. Femoral-femoral or femoral-jugular cannulation is much more expeditious. Therefore, the Avalon Elite® is poorly suited to emergency situations. Moreover, the Avalon Elite® is significantly more expensive than more conventional VV ECMO cannulas.
A recent case series of 72 patients cannulated with the Avalon Elite®; at Papworth Hospital (Cambridge, UK) reported an approximately 3% incidence of pneumothorax, 3% incidence of tamponade (due to RV perforation), 10% incidence of culture-proven infection (which is comparable to that seen in other forms of ECMO), and a 6% incidence of cannula migration.[35] This highlights the care with which this promising technology must be implemented and maintained.
Appropriate/Necessary Flow Rate for Veno-venous Extracorporeal Membrane Oxygenation (Oxygenation versus Decarboxylation)
To accomplish adequate oxygenation, VV ECMO requires minimum blood flow rates which are determined by cannula size, hemoglobin concentration, and properties of the oxygenator. A core principle of ECMO for respiratory failure is that decarboxylation occurs with much greater ease than oxygenation. When compared to oxygenation, blood flow rates, and hemoglobin concentration are much less important factors in decarboxylation. VV ECMO flow rates needed to support systemic oxygenation in adults should be 60–80 mL/kg/min. As such, an 80 kg adult would ideally receive a VV ECMO flow rate of 4.8 L/min, underscoring the importance of placing venous cannula that allows high blood flow rates. Selective decarboxylation requires decidedly less blood flow as compared to that needed for adequate blood oxygenation. Carbon dioxide clearance through ECMO is performed using “sweep gas” flow (the membrane lung ventilating gas) being blown over the blood in the ECMO circuit and also relies on properties of the membrane oxygenator. Approximately, 25% of native cardiac output is required to pass through the sweep gas flow and membrane lung to successfully clear carbon dioxide, which may represent as little as 15–20 mL/kg/min.[42]
Conclusions
Although ECMO is being more widely adopted, and there is a movement toward simpler ECMO configurations, the technology has certain intrinsic complexities and limitations which the astute clinician will be cognizant of VVA and VAV ECMO mitigate inadequate venous drainage (or, in the case of VV ECMO, concomitant cardiac dysfunction) and upper body hypoxemia, respectively. Distal perfusion cannulas treat distal ischemia in peripherally cannulated patients. Maintaining pulsatility and several other approaches have been described to treat LV distention and/or left atrial hypertension, which may improve myocardial perfusion and reduce the likelihood of intracardiac and aortic root thrombus. Recirculation may be seen in VV ECMO as a result of cannula position, the balance between ECMO and patient flows, as well as increased intrathoracic or intracardiac pressure. Newer dual lumen VV ECMO cannulas reduce the likelihood of recirculation and may facilitate extubation and patient mobilization at the expense of increased cost as well as technically challenging cannula insertion and positioning.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Hill JD, O’Brien TG, Murray JJ, Dontigny L, Bramson ML, Osborn JJ, et al. Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock-lung syndrome).Use of the Bramson membrane lung. N Engl J Med. 1972;286:629–34. doi: 10.1056/NEJM197203232861204. [DOI] [PubMed] [Google Scholar]
- 2.Zapol WM, Snider MT, Hill JD, Fallat RJ, Bartlett RH, Edmunds LH, et al. Extracorporeal membrane oxygenation in severe acute respiratory failure. A randomized prospective study. JAMA. 1979;242:2193–6. doi: 10.1001/jama.242.20.2193. [DOI] [PubMed] [Google Scholar]
- 3.Bartlett RH, Gazzaniga AB, Toomasian J, Coran AG, Roloff D, Rucker R. Extracorporeal membrane oxygenation (ECMO) in neonatal respiratory failure 100 cases. Ann Surg. 1986;204:236–45. doi: 10.1097/00000658-198609000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Truby L, Mundy L, Kalesan B, Kirtane A, Colombo PC, Takeda K, et al. Contemporary outcomes of venoarterial extracorporeal membrane oxygenation for refractory cardiogenic shock at a large tertiary care center. ASAIO J. 2015;61:403–9. doi: 10.1097/MAT.0000000000000225. [DOI] [PubMed] [Google Scholar]
- 5.Bacchetta M, Javidfar J, Sonett J, Kim H, Zwischenberger J, Wang D. Ease of conversion from venovenous extracorporeal membrane oxygenation to cardiopulmonary bypass and venoarterial extracorporeal membrane oxygenation with a bicaval dual lumen catheter. ASAIO J. 2011;57:283–5. doi: 10.1097/MAT.0b013e31821d3f35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Squiers JJ, Lima B, DiMaio JM. Contemporary extracorporeal membrane oxygenation therapy in adults: Fundamental principles and systematic review of the evidence. J Thorac Cardiovasc Surg. 2016;152:20–32. doi: 10.1016/j.jtcvs.2016.02.067. [DOI] [PubMed] [Google Scholar]
- 7.Shekar K, Mullany DV, Thomson B, Ziegenfuss M, Platts DG, Fraser JF. Extracorporeal life support devices and strategies for management of acute cardiorespiratory failure in adult patients: A comprehensive review. Crit Care. 2014;18:219. doi: 10.1186/cc13865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rupprecht L, Flörchinger B, Schopka S, Schmid C, Philipp A, Lunz D, et al. Cardiac decompression on extracorporeal life support: A review and discussion of the literature. ASAIO J. 2013;59:547–53. doi: 10.1097/MAT.0b013e3182a4b2f6. [DOI] [PubMed] [Google Scholar]
- 9.Mikus E, Tripodi A, Calvi S, Giglio MD, Cavallucci A, Lamarra M. CentriMag venoarterial extracorporeal membrane oxygenation support as treatment for patients with refractory postcardiotomy cardiogenic shock. ASAIO J. 2013;59:18–23. doi: 10.1097/MAT.0b013e3182768b68. [DOI] [PubMed] [Google Scholar]
- 10.Sangalli F, Patroniti N, Pesenti A, editors. ECMO-Extracorporeal Life Support in Adults. Milan: Springer-Verlag Mailand; 2014. [Google Scholar]
- 11.Abrams D, Javidfar J, Farrand E, Mongero LB, Agerstrand CL, Ryan P, et al. Early mobilization of patients receiving extracorporeal membrane oxygenation: A retrospective cohort study. Crit Care. 2014;18:R38. doi: 10.1186/cc13746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hoeper MM, Tudorache I, Kühn C, Marsch G, Hartung D, Wiesner O, et al. Extracorporeal membrane oxygenation watershed. Circulation. 2014;130:864–5. doi: 10.1161/CIRCULATIONAHA.114.011677. [DOI] [PubMed] [Google Scholar]
- 13.Hou X, Yang X, Du Z, Xing J, Li H, Jiang C, et al. Superior vena cava drainage improves upper body oxygenation during veno-arterial extracorporeal membrane oxygenation in sheep. Crit Care. 2015;19:68. doi: 10.1186/s13054-015-0791-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cove ME. Disrupting differential hypoxia in peripheral veno-arterial extracorporeal membrane oxygenation. Crit Care. 2015;19:280. doi: 10.1186/s13054-015-0997-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Napp LC, Kühn C, Hoeper MM, Vogel-Claussen J, Haverich A, Schäfer A, et al. Cannulation strategies for percutaneous extracorporeal membrane oxygenation in adults. Clin Res Cardiol. 2016;105:283–96. doi: 10.1007/s00392-015-0941-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Choi JH, Kim SW, Kim YU, Kim SY, Kim KS, Joo SJ, et al. Application of veno-arterial-venous extracorporeal membrane oxygenation in differential hypoxia. Multidiscip Respir Med. 2014;9:55. doi: 10.1186/2049-6958-9-55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Javidfar J, Brodie D, Costa J, Miller J, Jurrado J, LaVelle M, et al. Subclavian artery cannulation for venoarterial extracorporeal membrane oxygenation. ASAIO J. 2012;58:494–8. doi: 10.1097/MAT.0b013e318268ea15. [DOI] [PubMed] [Google Scholar]
- 18.Cheng R, Hachamovitch R, Kittleson M, Patel J, Arabia F, Moriguchi J, et al. Complications of extracorporeal membrane oxygenation for treatment of cardiogenic shock and cardiac arrest: A meta-analysis of 1,866 adult patients. Ann Thorac Surg. 2014;97:610–6. doi: 10.1016/j.athoracsur.2013.09.008. [DOI] [PubMed] [Google Scholar]
- 19.Mohite PN, Fatullayev J, Maunz O, Kaul S, Sabashnikov A, Weymann A, et al. Distal limb perfusion: Achilles’ heel in peripheral venoarterial extracorporeal membrane oxygenation. Artif Organs. 2014;38:940–4. doi: 10.1111/aor.12314. [DOI] [PubMed] [Google Scholar]
- 20.Bisdas T, Beutel G, Warnecke G, Hoeper MM, Kuehn C, Haverich A, et al. Vascular complications in patients undergoing femoral cannulation for extracorporeal membrane oxygenation support. Ann Thorac Surg. 2011;92:626–31. doi: 10.1016/j.athoracsur.2011.02.018. [DOI] [PubMed] [Google Scholar]
- 21.Koeckert MS, Jorde UP, Naka Y, Moses JW, Takayama H. Impella LP.2.5 for left ventricular unloading during venoarterial extracorporeal membrane oxygenation support. J Card Surg. 2011;26:666–8. doi: 10.1111/j.1540-8191.2011.01338.x. [DOI] [PubMed] [Google Scholar]
- 22.Sladen RN. New Innovations in ECMO and VAD Therapy. Lecture at the Society of Cardiovascular Anesthesiologists Annual Meeting. 2016 [Google Scholar]
- 23.Fukuhara S, Takeda K, Garan AR, Kurlansky P, Hastie J, Naka Y, et al. Contemporary mechanical circulatory support therapy for postcardiotomy shock. Gen Thorac Cardiovasc Surg. 2016;64:183–91. doi: 10.1007/s11748-016-0625-4. [DOI] [PubMed] [Google Scholar]
- 24.Kohler K, Valchanov K, Nias G, Vuylsteke A. ECMO cannula review. Perfusion. 2013;28:114–24. doi: 10.1177/0267659112468014. [DOI] [PubMed] [Google Scholar]
- 25.Takayama H, Landes E, Truby L, Fujita K, Kirtane AJ, Mongero L, et al. Feasibility of smaller arterial cannulas in venoarterial extracorporeal membrane oxygenation. J Thorac Cardiovasc Surg. 2015;149:1428–33. doi: 10.1016/j.jtcvs.2015.01.042. [DOI] [PubMed] [Google Scholar]
- 26.Aissaoui N, Morshuis M, Schoenbrodt M, Hakim Meibodi K, Kizner L, Börgermann J, et al. Temporary right ventricular mechanical circulatory support for the management of right ventricular failure in critically ill patients. J Thorac Cardiovasc Surg. 2013;146:186–91. doi: 10.1016/j.jtcvs.2013.01.044. [DOI] [PubMed] [Google Scholar]
- 27.Kai M, Tang GH, Malekan R, Lansman SL, Spielvogel D. Venoarterial extracorporeal membrane oxygenation for right heart failure complicating left ventricular assist device use. J Thorac Cardiovasc Surg. 2014;147:e31–3. doi: 10.1016/j.jtcvs.2013.10.040. [DOI] [PubMed] [Google Scholar]
- 28.Mohite PN, Sabashnikov A, De Robertis F, Popov AF, Simon AR. Oxy-RVAD: Rescue in pulmonary complications after LVAD implantation. Perfusion. 2015;30:596–9. doi: 10.1177/0267659114566062. [DOI] [PubMed] [Google Scholar]
- 29.Noly PE, Kirsch M, Quessard A, Leger P, Pavie A, Amour J, et al. Temporary right ventricular support following left ventricle assist device implantation: A comparison of two techniques. Interact Cardiovasc Thorac Surg. 2014;19:49–55. doi: 10.1093/icvts/ivu072. [DOI] [PubMed] [Google Scholar]
- 30.Haneya A, Philipp A, Puehler T, Rupprecht L, Kobuch R, Hilker M, et al. Temporary percutaneous right ventricular support using a centrifugal pump in patients with postoperative acute refractory right ventricular failure after left ventricular assist device implantation. Eur J Cardiothorac Surg. 2012;41:219–23. doi: 10.1016/j.ejcts.2011.04.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Sen A, Callisen HE, Alwardt CM, Larson JS, Lowell AA, Libricz SL, et al. Adult venovenous extracorporeal membrane oxygenation for severe respiratory failure: Current status and future perspectives. Ann Card Anaesth. 2016;19:97–111. doi: 10.4103/0971-9784.173027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Douflé G, Roscoe A, Billia F, Fan E. Echocardiography for adult patients supported with extracorporeal membrane oxygenation. Crit Care. 2015;19:326. doi: 10.1186/s13054-015-1042-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Brodie D, Bacchetta M. Extracorporeal membrane oxygenation for ARDS in adults. N Engl J Med. 2011;365:1905–14. doi: 10.1056/NEJMct1103720. [DOI] [PubMed] [Google Scholar]
- 34.Sidebotham D, Allen SJ, McGeorge A, Ibbott N, Willcox T. Venovenous extracorporeal membrane oxygenation in adults: Practical aspects of circuits, cannulae, and procedures. J Cardiothorac Vasc Anesth. 2012;26:893–909. doi: 10.1053/j.jvca.2012.02.001. [DOI] [PubMed] [Google Scholar]
- 35.Rubino A, Vuylsteke A, Jenkins DP, Fowles JA, Hockings L, Valchanov K. Direct complications of the Avalon bicaval dual-lumen cannula in respiratory extracorporeal membrane oxygenation (ECMO): Single-center experience. Int J Artif Organs. 2014;37:741–7. doi: 10.5301/ijao.5000357. [DOI] [PubMed] [Google Scholar]
- 36.Aggarwal V, Einhorn BN, Cohen HA. Current status of percutaneous right ventricular assist devices: First-in-man use of a novel dual lumen cannula. Catheter Cardiovasc Interv. 2016;88:390–6. doi: 10.1002/ccd.26348. [DOI] [PubMed] [Google Scholar]
- 37.Abrams D, Brodie D. Identification and management of recirculation in venovenous ECMO. ELSO Guidelines 2015. 2015 [Google Scholar]
- 38.Bermudez CA, Rocha RV, Sappington PL, Toyoda Y, Murray HN, Boujoukos AJ. Initial experience with single cannulation for venovenous extracorporeal oxygenation in adults. Ann Thorac Surg. 2010;90:991–5. doi: 10.1016/j.athoracsur.2010.06.017. [DOI] [PubMed] [Google Scholar]
- 39.Javidfar J, Brodie D, Wang D, Ibrahimiye AN, Yang J, Zwischenberger JB, et al. Use of bicaval dual-lumen catheter for adult venovenous extracorporeal membrane oxygenation. Ann Thorac Surg. 2011;91:1763–8. doi: 10.1016/j.athoracsur.2011.03.002. [DOI] [PubMed] [Google Scholar]
- 40.Abrams D, Brodie D, Javidfar J, Brenner K, Wang D, Zwischenberger J, et al. Insertion of bicaval dual-lumen cannula via the left internal jugular vein for extracorporeal membrane oxygenation. ASAIO J. 2012;58:636–7. doi: 10.1097/MAT.0b013e31826feda5. [DOI] [PubMed] [Google Scholar]
- 41.Shafii AE, McCurry KR. Subclavian insertion of the bicaval dual lumen cannula for venovenous extracorporeal membrane oxygenation. Ann Thorac Surg. 2012;94:663–5. doi: 10.1016/j.athoracsur.2012.02.024. [DOI] [PubMed] [Google Scholar]
- 42.Bartlett RH, Zwischenberger JB. Management of blood flow and gas exchange during ECLS. In: Annich G, Lynch W, MacLaren G, Wilson J, Bartlett R, editors. ECMO: Extracorporeal Cardiopulmonary Support in Critical Care. 4th ed. Ann Arbor, Michigan: ELSO; 2012. [Google Scholar]