

Abstract
Fetal cholelithiasis is a rare finding during a third-trimester ultrasound with an average incidence rate of 0.07–1.15%. We report a case of fetal cholelithiasis in twins, observed in a patient with monochorionic diamniotic twin pregnancy hospitalized at our unit for signs of premature labor. We present the outcome of the 2 neonates with a clinical and sonographic follow-up. In addition, we offer a comprehensive review of the literature available to date.
Key words: fetal cholelithiasis, fetal gallstones, intrahepatic cholestasis of pregnancy
Introduction
The first descriptions of fetal cholelithiasis (FC) reported in the literature were the 2 cases diagnosed at the time of autopsy cited by Potter in 1928 1, whereas the first prenatal diagnosis was reported in 1983 by Beretsky and Lankin 2. FC is a rare and typically incidental finding during a third-trimester ultrasound exam. Although very few cases are reported in the literature, its frequency of diagnosis has increased over the last 20 years, probably due to technological progress and the increasing use of ultrasound examination during prenatal controls. In this article we report a case of FC in a monochorionic diamniotic twin pregnancy, associated with a cholestasis of pregnancy, afflicting the mother. In addition, we present a comprehensive review of the current literature available to date.
Methods
We prospectively collected and reviewed clinical and radiographic data of the above-mentioned patients. In addition, we performed a systematic review of the literature available to date. We used a multimethod approach to identify all reported cases of FC from 1980 to 2015. We performed a systematic search in the PubMed and Google Scholar databases. The terms used in the search were “fetal gallbladder” combined with any of the following words: “sludge”, “gallstones”, “lithiasis”, and “echogenic material”. Other search terms were “fetal cholelithiasis”, “fetal gallstones”, and “prenatal/antenatal gallstones/cholelithiasis”. We included all relevant original articles written in any language with an English abstract. Bibliographies of all included articles were reviewed for other relevant articles. We selected all of the articles reporting observed cases of FC. Articles describing FC but not reporting observed cases were rejected. We finally selected 28 articles with a total of 133 reported cases.
Case report
A 36-year-old woman (gravida 2, para 2), with a monochorionic diamniotic twin pregnancy, was hospitalized at 30 5/7 gestational weeks (GW) for premature contractions. The maternal medical situation highlighted a group B beta-hemolytic streptococcus positive test, an AB Rh+ blood type, and a previous uncomplicated pregnancy with term vaginal delivery 4 years before. After the admission we established tocolytic therapy with hexoprenaline (from 30 5/7 GW), an antibiotic therapy with amoxicillin for 1 week and a glucocorticoid therapy with betamethasone to induce fetal lung maturation. At 32 0/7 GW the patient reported a generalized cutaneous itch, especially on the palms of the hands and on the abdomen. The laboratory blood tests showed high levels of bile acids, and alteration of the common hepatic tests (Table 1). Intrahepatic cholestasis of pregnancy was diagnosed. The patient was treated with a tritherapy with ursodeoxycholic acid, levocetirizine, and cholestyramine. At 33 3/7 GW, an ultrasound exam was performed. Twin A showed a cephalic position I, an estimated weight of 2 400 g (83rd percentile), an amniotic fluid index in the normal range, and a hyperechogenic intra-cystic cholelithiasis (Fig. 1a). Twin B showed a cephalic position II, an estimated weight of 1 900 g (30th percentile), an amniotic fluid index in the normal range, and a suspected intra-cystic cholelithiasis (Fig. 1b). At 36 0/7 GW an iterative cesarean section was performed, with no maternal complications during and after the surgery. During the postpartum period, we observed complete regression of the mother’s itching symptoms and normalization of her laboratory tests (Table 1). Because of an anemic state (Hb 98 g/l at second pp-day), the patient was treated with oral iron supplements. The 2 newborn males showed the following: twin A had a birth weight of 2 915 g (50–75th percentile), a length of 50 cm, a head circumference of 34 cm, an Apgar score of 9/10/10, an umbilical artery pH of 7.26, and an umbilical vein pH of 7.31. Twin B showed a birth weight of 2 230 g (25–50th percentile), a length of 47 cm, a head circumference of 32.5 cm, an Apgar score of 9/9/10, an umbilical artery pH of 7.26, and an umbilical vein pH of 7.32. After birth, both neonates were transferred to the pediatric unit due to hypoglycemia. The measured glycemia was 2.2 mmol/l and 1.6 mmol/l for twin A and B, respectively. The newborns were treated with a glucose infusion from the first to the third postnatal day when the condition completely resolved. On the seventh postnatal day, a neonatal transabdominal ultrasound control was performed. We were able to confirm the diagnosis of cholecystolithiasis in twin B (Fig. 2a), while the ultrasound of twin A showed no signs suggesting the presence of gallstones (Fig. 2b), possibly due to complete intrauterine resolution. During the following months, twin B remained completely asymptomatic. An ultrasound at 6 months of life showed complete disappearance of the lithiasis. No further exams were undertaken. Currently, the children aged 2 years and 6 months are completely asymptomatic and have adequate food tolerance without associated disorders.
Table 1 Blood laboratory tests.
| 32 2/7 GW | 32 4/7 GW | 32 6/7 GW | 33 3/7 GW | 33 6/7 GW | 34 4/7 GW | 35 3/7 GW | 3rd pp-day | |
|---|---|---|---|---|---|---|---|---|
| AST (N<36) | 90 | 101 | 109 | 122 | 98 | – | 97 | 58 |
| ALT (N<37) | 163 | 192 | 201 | 272 | 232 | – | 190 | 94 |
| GGT (N<36) | 47 | 47 | 44 | – | – | – | 17 | – |
| LDH (N<500) | 283 | – | – | 353 | 322 | – | 379 | 495 |
| Bile Acids (N<11.3) | 69 | – | – | – | 58 | 46 | – | 15 |
GW=gestational weeks; pp=postpartum; AST=aspartate aminotransferase (U/L); ALT=alanine aminotransferase (U/L); GGT=gamma-glutamyl transferase (U/L); LDH=lactate dehydrogenase (U/L); bile acids (μmol/L)
Fig. 1.
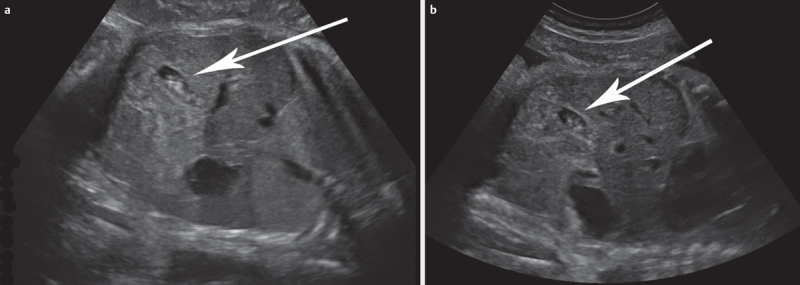
Ultrasound at 33 3/7 gestational weeks showing a hyperechogenic intra-cystic cholelithiasis in twin A and b suspected intra-cystic cholelithiasis in twin B. Abb. 1Ultraschall bei 33 3/7 Schwangerschaftswochen zeigt a hyperechogene intrazystische Gallensteine bei Zwilling A und b. Verdacht auf intrazystische Cholelithiasis bei Zwilling B.
Fig. 2.
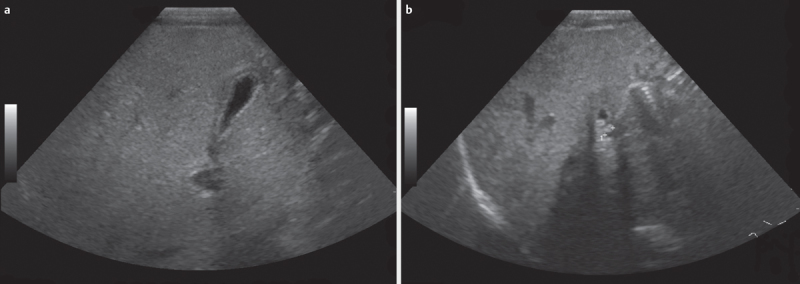
Transabdominal ultrasound on seventh postnatal day showing a no lithiasis in twin A’s cholecyst and b hyperechogenic cholecystolithiasis in twin B. Abb. 2 Der transabdominale Neugeborenen-Ultraschall am 7. Lebenstag zeigt (a) keine Lithiasis in der Gallenblase von Zwilling A und (b) eine hyperechogene Chlezystolithiasis bei Zwilling B.
Discussion
Anomalies of the gallbladder, including biliary sludge and gallstones, are uncommon in fetal life. Their rate of incidence seems to be between 0.07% and 1.15% 3 4 5 6 7 8. The etiopathogenesis of FC is currently unknown. In contrast to the cases of gallstones observed in pediatric and adult patients, where specific risk factors are well known, no established correlations are described for the fetal cases 9 10. Several authors have suggested different maternal, obstetric, and fetal predisposing risk factors (Table 2) 2 3 4 5 6 7 8 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31. Some reported patients presented more than one risk factor, while others presented none. Although at least one associated factor was present in about 1 in 4 cases, the remaining three-quarters of patients presented no abnormality or special condition that could explain the FC. Even in cases associated with a proposed risk factor, it was often difficult to determine its actual contribution to the pathogenesis of this disorder.
Table 2 Maternal and fetal conditions associated with fetal cholelithiasis 2 3 4 5 6 7 8 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31.
| Maternal factors | Number of reported cases |
|---|---|
| Hemolytic diseases | 1 |
| Placental abruption | 2 |
| History of cholelithiasis | 7 |
| All types of diabetes | 6 |
| Narcotics use (methadone) | 4 |
| Ceftriaxone treatment | 1 |
| Prostaglandin E2 treatment | 1 |
| Twin pregnancy | 7 |
| Twin pregnancy with fetal demise of one twin | 1 |
| Intrahepatic cholestasis of pregnancy | 2 |
| Increased estrogen and progestin levels | * |
| Fetal factors | Number of reported cases |
| Hemolytic diseases | 1 |
| Congenital malformations (cardiovascular, gastrointestinal, urologic, skeletal) | 7 |
| Chromosome anomalies (trisomy 21, translocation 10;11) | 2 |
| Intrauterine growth restriction | 11 |
| Oligohydramnios | 5 |
| Polyhydramnios | 5 |
| Prenatal leukemoid reaction | 1 |
| Anomalies of the biliary tract | – |
| Fetal-maternal blood group incompatibility | – |
* unquantifiable
Augmented erythrocyte degradation increases the bilirubin levels and has been shown to predispose to gallstone formation in postnatal life. An analogous situation could be involved in the development of FC during maternal or fetal hemolytic diseases, fetal-maternal blood group incompatibility, and following placental abruption or single-fetal demise in twin pregnancy 2 4 5 11 14 25 29 30. Ceftriaxone is known to enhance the precipitation of insoluble calcium salts, which is a predisposing factor for cholelithiasis 32. During pregnancy, the transplacental passage of ceftriaxone could produce the same effect on the fetal gallbladder, inducing gallstone formation 31. Conditions associated with raised maternal estrogen and progestin levels (e. g., twin pregnancy) could predispose the patient to FC as a result of increased cholesterol secretion and the reduction of biliary acids synthesis 11 14 25. Maternal narcotic use could reduce gastrointestinal activity, increasing gallbladder emptying time and resulting in augmented lithogenicity 3. A maternal history of gallstones has been observed in 7 cases, suggesting a possible genetic predisposition to cholelithiasis 11 14 18. In addition, maternal diabetes 14 24, prostaglandin use 4, prenatal fetal leukomoid reaction 4, chromosomal aberrations 4, intrauterine growth restriction 3 4 13 14 15 17 27, amniotic fluid disorders 4 7 13 14 17 24 25 31, and different cardiac, gastrointestinal, and urologic malformations 4 7 13 14 have been observed in association with FC, but no clear correlation has been proposed. Some authors have suggested that FC may be sex-linked 7 11 18 26 31. After having analyzed the totality of the reported cases, no significant difference between the 2 sexes has been observed (62 males and 56 females) 2 3 4 5 7 8 11 12 13 14 15 16 17 18 19 21 23 24 25 26 27 29 30 31. In our case, we hypothesize that the cholestatic effects of the raised circulating reproductive hormones associated with twin pregnancy, combined with a genetic predisposition of the 3 subjects, could have played an important role in the pathogenesis behind both the maternal intrahepatic cholestasis of pregnancy and the FC 14 33 34. However, a direct effect of the elevated maternal bile acids on the fetal lithogenicity could not be excluded.
The FC appears to be a specific condition of the third trimester of pregnancy. All but 3 cases reported in the literature were diagnosed after 28 weeks of gestation 15 27 31. Even in the systematic control of 1 656 consequent high-risk pregnancies examined before 28 weeks of gestation by Kiserud et al., no case of FC was discovered 4. Starting with the second trimester, it is possible to visualize the fetal gallbladder on ultrasonography. It appears as an elliptical, anechogenic structure placed on the right side of the intrahepatic umbilical vein 35 36. Echogenic material in the fetal gallbladder can be observed in the form of single, multiple, or diffuse foci. The diffuse form, known as “biliary sludge”, seems to be a precursor of gallstones, and was reported to be present in around 40% of cases 3 4 5 6 7 11 12 14 20 25. Unlike in pediatric and adult patients, FC may present with extremely varied ultrasound features. Echogenicity, homogeneity, and degrees of acoustic shadowing may vary greatly from one case to another. This wide range of possibilities may make the diagnosis difficult. It is extremely important to ascertain the intra-cholecystic position of echogenic foci in order to distinguish between gallstones and other possible sources of echogenicity in the right upper quadrant 30. If FC is substantially a benign state, other conditions, such as hepatic calcifications, calcified hepatic masses, or meconial peritonitis, may be related to a high degree of morbidity and mortality 17 18 30. In special situations, such as when the gallbladder is contracted, differentiation between them may prove very difficult 11 27.
It is a common belief that FC resolves spontaneously with hydration and feeding soon after birth. Stringer et al. have proposed that characteristic conditions of the postnatal period, such as increased bile flow and changes in its composition, may allow for the dissolution of gallstones and their subsequent passage through the bile ducts 27. In the literature, there have been 63 reported cases of FC with postnatal ultrasonographic follow-up to complete resolution 2 3 4 5 6 7 8 11 12 13 14 15 16 17 18 19 21 23 24 26 27 28 29 30 31. More than 70% of the patients had resolution within 2 months from birth, and more than 90% within 6 months. Persistence beyond 12 months has been observed in only 2 patients 3 31. No substantial difference in resolution time has been observed between patients presenting solid gallstones and biliary sludge. The majority of the patients were treated conservatively, which, in most cases, meant by observation alone. 5 were treated with ursodeoxycholic acid with the intent to allow rapid resolution and decrease the risk of complications, but no relevant differences have been observed among the other cases 8 11 23. Until now, only 3 cases of suspected FC requiring surgery have been reported 15 21 37.
In contrast to pediatric and adult cases of gallstones, where spontaneous resolution is rare and surgery is often required, FC seems self-limiting. A conservative attitude appears to be suitable. Ultrasound exams are recommended at birth and until complete resolution. No medical treatment is advised, and surgery should be reserved for those rare symptomatic cases accompanied by complications. It has been suggested that FC may predispose individuals to future gallstone formation 2, but up to now no specific cases have been reported.
Conclusion
With this case, we report the association between FC and intrahepatic cholestasis of pregnancy, which was previously hypothesized by some authors, but had never been previously confirmed. Several questions remain unanswered about the actual frequency, pathogenesis and etiology of fetal cholelithiasis. What we do know is its self-limiting and benign character. Considering its high rate of spontaneous resolution, we recommend reassuring parents and closely observing the clinical evolution of the patients, without any medical or surgical treatment. However, clinical and ultrasonographic follow-up should continue until demonstration of resolution.
Footnotes
Conflict of Interest No conflict of interest has been declared by the author(s).
References
- 1.Potter A H. Gall-bladder disease in young subjects. Surg Gynecol Obstet. 1928;46:795–808. [Google Scholar]
- 2.Beretsky I, Lankin D H. Diagnosis of fetal cholelithiasis using real-time high-resolution imaging employing digital detection. J Ultrasound Med. 1983;2:381–383. doi: 10.7863/jum.1983.2.8.381. [DOI] [PubMed] [Google Scholar]
- 3.Devonald K J, Ellwood D A, Colditz P B. The variable appearances of fetal gallstones. J Ultrasound Med. 1992;11:579–585. doi: 10.7863/jum.1992.11.11.579. [DOI] [PubMed] [Google Scholar]
- 4.Kiserud T, Gjelland K, Bognø H, Waardal M, Reigstad H, Rosendahl K. Echogenic material in the fetal gallbladder and fetal disease. Ultrasound Obstet Gynecol. 1997;10:103–106. doi: 10.1046/j.1469-0705.1997.10020103.x. [DOI] [PubMed] [Google Scholar]
- 5.Agnifili A, Verzaro R, Carducci G, Mancini E, Gola P, Marino M. et al. Fetal cholelithiasis: a prospective study of incidence, predisposing factors, and ultrasonographic and clinical features. Clin Pediatr (Phila) 1999;38:371–373. doi: 10.1177/000992289903800610. [DOI] [PubMed] [Google Scholar]
- 6.Müller R, Döhmann S, Kordts U. Fetale Gallenblase und Gallensteine. Ultraschall Med. 2000;21:142–144. doi: 10.1055/s-2000-3796. [DOI] [PubMed] [Google Scholar]
- 7.Cancho Candela R, Díaz González J, Perandones Fernández C, Viñuela Rueda B, Relea Sarabia A, Andrés de Llano J M. Material ecogénico en vesícula biliar fetal: diagnóstico prenatal y seguimiento posnatal. An Pediatr (Barc) 2004;61:326–329. doi: 10.1016/s1695-4033(04)78396-4. [DOI] [PubMed] [Google Scholar]
- 8.Munjuluri N, Elgharaby N, Acolet D, Kadir R A. Fetal gallstones. Fetal Diagn Ther. 2005;20:241–243. doi: 10.1159/000085077. [DOI] [PubMed] [Google Scholar]
- 9.Svensson J, Makin E. Gallstone disease in children. Semin Pediatr Surg. 2012;21:255–265. doi: 10.1053/j.sempedsurg.2012.05.008. [DOI] [PubMed] [Google Scholar]
- 10.Afdhal N H Epidemiology, risk factors, and pathogenesis of gallstonesIn:New York: Marcel Dekker, Inc.2000127–146. [Google Scholar]
- 11.Iroh Tam P-Y, Angelides A. Perinatal detection of gallstones in siblings. Am J Perinatol. 2010;27:771–774. doi: 10.1055/s-0030-1254239. [DOI] [PubMed] [Google Scholar]
- 12.Abbitt P L, McIlhenny J. Prenatal detection of gallstones. J Clin Ultrasound. 1990;18:202–204. doi: 10.1002/jcu.1870180313. [DOI] [PubMed] [Google Scholar]
- 13.Broussin B, Daube E. La lithiase vésiculaire foetale. A propos de trois observations et revue de la littérature. J Gynecol Obstet Biol Reprod (Paris) 1990;19:90–95. [PubMed] [Google Scholar]
- 14.Brown D L, Teele R L, Doubilet P M, DiSalvo D N, Benson C B, Van Alstyne G A. Echogenic material in the fetal gallbladder: sonographic and clinical observations. Radiology. 1992;182:73–76. doi: 10.1148/radiology.182.1.1727312. [DOI] [PubMed] [Google Scholar]
- 15.Clarke J P, Roman J D. The outcome of two cases of fetal cholelithiasisN Z Med J. 1994. p. 270. [PubMed]
- 16.Heijne L, Ednay D. The development of fetal gallstones demonstrated by ultrasound. Radiography. 1985;51:155–156. [PubMed] [Google Scholar]
- 17.Hertzberg B S, Kliewer M A. Fetal gallstones in a contracted gallbladder: potential to simulate hepatic or peritoneal calcification. J Ultrasound Med. 1998;17:667–670. doi: 10.7863/jum.1998.17.10.667. [DOI] [PubMed] [Google Scholar]
- 18.Holloway S, Edwards H. Antenatal diagnosis of fetal cholelithiasis. Ultrasound. 2010;18:152–154. [Google Scholar]
- 19.Klingensmith W C, Cioffi-Ragan D T. Fetal gallstones. Radiology. 1988;167:143–144. doi: 10.1148/radiology.167.1.3279452. [DOI] [PubMed] [Google Scholar]
- 20.Lariviere M. Having K, Bullock S. Fetal Cholelithiasis. Journal of Diagnostic Medical Sonography. 2006;22:403–406. [Google Scholar]
- 21.López Gutiérrez J C, Ros Mar Z, López Santamaría M, Díez Pardo J A, González Gonzalez A, Pastor Abascal I. et al. Colelitiasis fetal. Caso clínico y revisión de la literatura. An Esp Pediatr. 1990;32:468–469. [PubMed] [Google Scholar]
- 22.Nishi T. Ultrasonographic diagnosis of fetal cholelithiasis. J Obstet Gynaecol Res. 1997;23:251–254. doi: 10.1111/j.1447-0756.1997.tb00840.x. [DOI] [PubMed] [Google Scholar]
- 23.Ozgun M T, Batukan C, Ozcelik B, Serin S, Basbug M. Prenatal sonographic diagnosis of fetal gallstones: a case report. Ultrasound Obstet Gynecol. 2006;28:535–536. [Google Scholar]
- 24.Petrikovsky B, Klein V, Holsten N. Sludge in fetal gallbladder: natural history and neonatal outcome. Br J Radiol. 1996;69:1017–1018. doi: 10.1259/0007-1285-69-827-1017. [DOI] [PubMed] [Google Scholar]
- 25.Sepulveda W, Stagiannis K D. Echogenic material in the fetal gallbladder in a surviving monochorionic twin. Pediatr Radiol. 1996;26:129–130. doi: 10.1007/BF01372091. [DOI] [PubMed] [Google Scholar]
- 26.Sheiner E, Abramowicz J S, Hershkovitz R. Fetal gallstones detected by routine third trimester ultrasound. Int J Gynaecol Obstet. 2006;92:255–256. doi: 10.1016/j.ijgo.2005.07.024. [DOI] [PubMed] [Google Scholar]
- 27.Stringer M D, Lim P, Cave M, Martinez D, Lilford R J. Fetal gallstones. J Pediatr Surg. 1996;31:1589–1591. doi: 10.1016/s0022-3468(96)90189-x. [DOI] [PubMed] [Google Scholar]
- 28.Suchet I B, Labatte M F, Dyck C S, Salgado L A. Fetal cholelithiasis: a case report and review of the literature. J Clin Ultrasound. 1993;21:198–202. doi: 10.1002/jcu.1870210309. [DOI] [PubMed] [Google Scholar]
- 29.Suma V, Marini A, Bucci N, Toffolutti T, Talenti E. Fetal gallstones: sonographic and clinical observations. Ultrasound Obstet Gynecol. 1998;12:439–441. doi: 10.1046/j.1469-0705.1998.12060439.x. [DOI] [PubMed] [Google Scholar]
- 30.Triunfo S, Rosati P, Ferrara P, Gatto A, Scambia G. Fetal cholelithiasis: a diagnostic update and a literature review. Clin Med Insights Case Rep. 2013;6:153–158. doi: 10.4137/CCRep.S12273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Troyano-Luque J, Padilla-Pérez A, Martínez-Wallin I, Alvarez de la Rosa M, Mastrolia S A, Trujillo J L. et al. Short and long term outcomes associated with fetal cholelithiasis: a report of two cases with antenatal diagnosis and postnatal follow-up. Case Rep Obstet Gynecol. 2014 doi: 10.1155/2014/714271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Rodríguez Rangel D A, Pinilla Orejarena A P, Bustacara Diaz M, Henao García L, López Cadena A, Montoya Camargo R. et al. Cálculos biliares asociados al uso de ceftriaxona en niños. Anales de Pediatría. 2014;80:77–80. doi: 10.1016/j.anpedi.2013.04.001. [DOI] [PubMed] [Google Scholar]
- 33.Geenes V, Williamson C. Intrahepatic cholestasis of pregnancy. World J Gastroenterol. 2009;15:2049–2066. doi: 10.3748/wjg.15.2049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Almashhrawi A A, Ahmed K T, Rahman R N, Hammoud G M, Ibdah J A. Liver diseases in pregnancy: diseases not unique to pregnancy. World J Gastroenterol. 2013;19:7630–7638. doi: 10.3748/wjg.v19.i43.7630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Moon M H, Cho J Y, Kim J H, Lee Y H, Jung S I, Lee M S. et al. In Utero Development of the Fetal Gall Bladder in the Korean Population. Korean Journal of Radiology. 2008;9:54–58. doi: 10.3348/kjr.2008.9.1.54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Albay S, Malas M A, Koyuncu E, Evcil E H. Morphometry of the gallbladder during the fetal period. Surg Radiol Anat. 2010;32:363–369. doi: 10.1007/s00276-009-0574-z. [DOI] [PubMed] [Google Scholar]
- 37.Gertner M, Farmer D L. Laparoscopic cholecystecomy in a 16-day-old infant with chronic cholelithiasis. J Pediatr Surg. 2004;39:E17–E19. doi: 10.1016/j.jpedsurg.2003.09.034. [DOI] [PubMed] [Google Scholar]