

Abstract
Background:
Multiple sclerosis (MS) is a chronic degenerative disease of the central nervous system (CNS) that can reduce health promoting behaviors in patients. One method of increasing health promoting behaviors is motivational interviewing that can explore and resolve client ambivalence.
Materials and Methods:
The present clinical trial was carried out among 60 patients with MS. The participants were selected through convenience sampling, and then, allocated to two groups using Mini Pay software. The intervention group participated in three sessions of motivational interviewing per week (1 session every 2 days, and each session lasting 1 h). A two-part questionnaire consisting of demographic data and the Health Promoting Lifestyle Profile (HPLP) II questionnaire was used for data collection. The collected data were analyzed using statistical tests such as independent t-test, and Mann–Whitney and Chi-square tests.
Results:
No statistically significant difference was observed between the groups in terms of the demographic variables (P > 0.05). The results also showed no significant difference in the overall score of the health promoting behaviors and its dimensions between the two groups before the intervention (P > 0.05). However, 2 weeks and 1 month after the intervention, there was a significant difference between the groups in terms of the overall score and the scores of dimensions, except the spiritual growth dimension (P > 0.05).
Conclusions:
The findings of this study showed that motivational interviewing can improve health promoting behaviors in patients with MS. Therefore, this method can be used by nurses to improve health promoting behaviors among these patients.
Keywords: Health promotion, motivational interviewing, multiple sclerosis
INTRODUCTION
The epidemiology of diseases has changed in comparison with the past, and noncommunicable diseases are increasing. In addition to factors, such as age and sex, these diseases are also influenced by factors such as physical activity, obesity, and diet, which are adjustable. Noncommunicable diseases such as diabetes, hypertension, cardiovascular disease (CVD), and multiple sclerosis (MS) can be controlled through lifestyle modifications and improvement in health care.[1]
MS is a chronic and progressive demyelination of the central nervous system (CNS) that affects a wide range of neurological functions.[2] Approximately 2.5 million individuals in the world and, according to the Multiple Sclerosis Society of Iran, more than 40 thousand individuals in Iran suffer from MS.[3,4] In Isfahan (Iran), the number of patients with this disease is approximately 4250 individuals. Isfahan, in proportion to the population of the region, has the highest rate of the disease in Iran.[5] MS affects patient's independence and ability to participate effectively in family and social activities. The complications of the disease incapacitate patients in self-care.[6] Ambivalence and failure to follow the prescribed therapeutic regimen are common problems in these patients, which can lead to disease progression, disability, increased mortality rates, and decreased health promoting behaviors in these patients. Ambivalence in the dimension of nutrition, physical activity and exercise, sleep pattern, and methods of coping with stress is common. Ambivalence is hesitation in following therapeutic behavior; this means that the patient has a combination of inclinations toward the performance and lack of performance of therapeutic behavior.[7,8]
In the past several decades, the World Health Organization (WHO) has changed the focus of health care from disease to disease prevention and health promotion.[9] Health promotion includes all activities that encourage individuals to perform physical, mental, and spiritual activities.[10]
Health-promoting behaviors are a major determinant criterion, and the prevention of diseases is directly linked to these behaviors.[11] Individuals’ lifestyle has a direct relationship with their health; a healthy lifestyle can improve health. The goal of improving health-promoting behaviors is to empower individuals to improve their lifestyles and have more control over their health.[12]
In recent years, the impact of different interventions on behavioral changes in chronic diseases has been examined. One of the recent interventions in the area of chronic diseases is motivational interviewing that is effective on behavioral and lifestyle changes in these patients.[13]
In order to increase intrinsic motivation, motivational interviewing directly identifies and resolves patients’ ambivalence toward change. Studies have shown that motivational interviewing can cause immense changes through increasing motivation.[14] In the study conducted by Smith and Lanesskog, motivational interviewing improved physical activity, reduced fatigue, and increased the duration of exercise in patients with MS.[15] Nevertheless, it was not effective on patients’ adherence to exercise programs.[15] The study conducted by Bombardier also showed that telephone-based motivational interviewing can improve health-promoting behaviors in patients with MS.[16] The study conducted by Ghasemipour showed motivational interviewing to be ineffective in the prevention of obesity in patients with coronary artery diseases (CADs).[17] In Iran, no study was found regarding the effectiveness of motivational interviewing on health-promoting behaviors of patients with MS. Statistics show the increasing prevalence of MS,[18] and if patients’ ambivalence is not resolved, the disease may progress and patients’ health-promoting behaviors may be reduced. Because of these problems, inconsistencies among studies, the importance of health-promoting behaviors, and the increasing use of motivational interviewing in the world, this study examined the impact of motivational interviewing on health-promoting behaviors of patients with MS. According to a previous study, Isfahan has the highest prevalence of MS in Iran.[18] Al-Zahra Hospital is one of the most important centers in the city and a large number of patients with MS refer to the hospital for medicine, education, and follow-up. Therefore, the Multiple Sclerosis Clinic of this hospital was selected as the research environment.
MATERIALS AND METHODS
This study was a clinical trial registered with the code IRCT 2015011620675n1. It had two study groups and was performed in three stages (before the intervention, 2 weeks after the intervention, and 1 month after the intervention for follow-up). The study population included 60 patients with MS who referred to the Multiple Sclerosis Clinic of Al-Zahra Hospital, affiliated with the Isfahan University of Medical Sciences, Isfahan. Because of the time limitation, sampling was performed via convenient sampling method. The inclusion criteria included the diagnosis of MS by a doctor, Expanded Disability Status Scale (EDSS) score of 0–5.5, lack of any other chronic diseases, lack of cognitive and learning disorders of axis 1 and 2 Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR), and ability to read and write. The exclusion criteria included lack of willingness to participate in the study, absent from more than one session out of three sessions of the motivational interviewing, hospitalization, and death before the end of the study. Data were collected using a questionnaire that consisted of two parts. The first part consisted of the Health Promoting Lifestyle Profile (HPLP) II questionnaire. The second part consisted of a demographic questionnaire including questions on age, sex, education, marital status, employment status, duration of the disease, and presence of other diseases. The HPLP II is a modified version of the HPLP expanded by Walker and Pender. The HPLP II evaluates health-promoting behaviors by focusing on individual initiative and perception.[19,20] The study conducted by Mohammadi Zeidi assessed the validity and reliability of the Persian version of the HPLP.[21] They reported the Cronbach's alpha coefficient of the tool as 0.82 and its dimensions as 0.64–0.91, and showed that the Persian version of the questionnaire has sufficient validity and reliability. The questionnaire includes six dimensions, namely, nutrition, physical activity, stress management, interpersonal relationships, responsibility for health, and spiritual growth (52 questions). The items are scored based on a 4-point Likert scale (never, sometimes, often, and usually).[21] The total score of the questionnaire ranges from a minimum of 52 to a maximum of 208. The score of each dimension is calculated separately and a higher scores mean better health.
This research was scientifically and ethically validated by the Ethics Committee of the Isfahan University of Medical Sciences. The researcher obtained a referral letter from the School of Nursing and Midwifery of Isfahan University of Medical Sciences. Subsequently, the researcher presented the introduction letter and explained the objectives of the study to the hospital management, and after obtaining their consent, performed sampling. Patients were randomly assigned to the intervention (n = 30) and control (n = 30) groups using Mini Pay software which distributes subjects between groups and prevents unwanted mismatch between groups.[22] The intervention group was divided into 3 groups (n = 10) and the intervention was performed in these small groups. These groups participated in three sessions of motivational interviewing per week (one session every 2 days and each session lasting 1 h). The intervention was conducted through group method because Miller and Rowling believed that motivational interviewing through group method is more effective than individual method. The structure of motivational interviewing sessions was extracted from the book Motivational Interviewing, Practical Guide, written by Navidian.[23]
The structure and content of motivational interviewing sessions:
First session: The introduction of norms, process, and purpose of the group, dimensions of the effects of behavior, alteration stages, evaluation of commitment and trust, and clarification opportunity
Second session: The positive and negative aspects of behavior and change, evaluation of the profits and losses arising from change, the description of the nature of human values, and identification, clarification, and confirmation of the values of patients
Third session: Perspective, recognition of tempting and helpful situations, the final evaluation of purpose, commitment, trust, and motivation to change.
Before the motivational interviewing sessions and 2 weeks and 1 month after the last session, the questionnaires were completed by both groups. The control group only participated in a group discussion session about the disease.
The collected data were analyzed using the Statistical Package for the Social Sciences software (version 19, SPSS Inc., Chicago, IL, USA). Descriptive and inferential statistical tests including independent t-test, and Mann–Whitney, Chi-square, repeated measures analysis of variance (ANOVA), Fisher's exact, and least significant difference (LSD) tests were used for statistical analysis.
Ethical considerations
The selected patients were reassured about data confidentiality and their access to the final results. Participants read and understood the information necessary to make an informed decision about their voluntary participation.
RESULTS
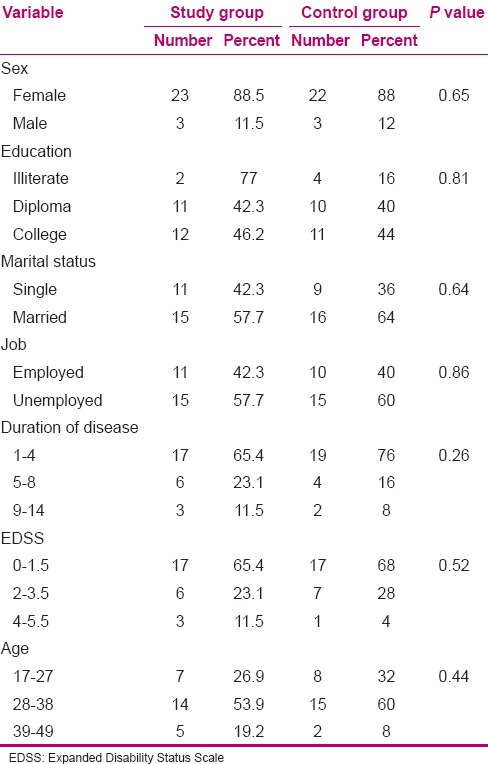
Out of the 60 patients who participated in the study, 26 patients in the intervention group and 25 patients in the control group completed the study. The patients, who completed the study, consisted of 49 women and 11 men. The mean age in the intervention group was 31.8 [standard deviation (SD): 7.4] and in the control group was 30.4 (6.2). In terms of education level, university education had the highest prevalence in both the intervention (46.2%) and control (44%) groups. In the intervention group, most patients were married (57.7%) and employed (42.3%), and at the beginning of the study, had a mean duration of disease of 4.5 (3.1). In the control group, most patients were married (64%) and employed (40%), and at the beginning of the study, had a mean duration of disease of 3.6 (2.5). The mean EDSS score in the intervention and control groups was 1.69 (1.3) and 1.48 (1.02), respectively. Independent t-test results showed no statistically significant difference before the intervention between the two groups in terms of the variables of age, disease duration, and EDSS score (P > 0.05). The Fisher's exact, Mann–Whitney, and Chi-square tests results showed no significant difference before the intervention between the two groups in terms of the variables of gender, educational level, marital status, and employment (P > 0.05), and the matched groups [Table 1].
Table 1.
Comparison of demographic variables between study and control groups
The repeated-measures ANOVA test results showed statistically significant differences in the intervention group before and 2 weeks and 1 month after the intervention in terms of the mean score of overall health-promoting behaviors and its dimensions (P < 0.05). In addition, the LSD test results showed that the scores of all the dimensions of the health-promoting behaviors increased significantly after the intervention (P < 0.05). However, there was no significant difference between the dimensions 2 weeks and 1 month after the intervention (P > 0.05). The repeated-measures ANOVA results showed no significant differences in the control group in terms of the mean overall score of health-promoting behaviors and its dimensions before the study and 2 weeks and 1 month after the study (P > 0.05) [Table 2].
Table 2.
Comparison of health-promoting behaviors and their domains before, 2 weeks and 1 month after intervention in study and control groups
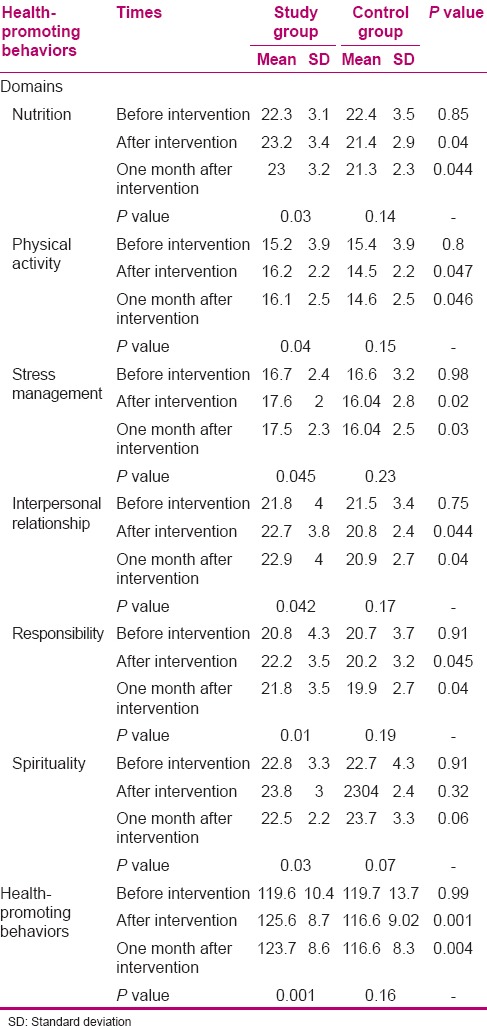
The comparison of the mean overall score of health-promoting behaviors and its dimensions between the experimental and control groups before the intervention using independent t-test showed no statistically significant difference between the two groups (P > 0.05). Nevertheless, independent t-test results showed significant differences between the two groups in terms of the mean overall score and the scores of the nutrition, physical activity, stress management, interpersonal relationships, and responsibility dimensions 2 weeks and 1 month after the intervention (P < 0.05). These results showed that the interventions could be effective on health-promoting behaviors. However, a significant difference was not observed between the groups in terms of mean score of the spiritual growth dimension (P > 0.05).
DISCUSSION
The results of this study showed that motivational interviewing was effective in the improvement of health-promoting behaviors in patients with MS. However, it was not effective in improving the spiritual growth dimension of the behaviors. No statistically significant difference was observed in the mean score of the spiritual growth dimension between the experimental and control groups 2 weeks and 1 month after the intervention (P > 0.05). In this respect, the results of the study conducted by Norouzinia et al. indicated that anxiety has a negative correlation with spiritual growth and can reduce the average score of this dimension.[24] The lack of significant difference in the spiritual growth dimension may be because of the patients’ presence in the motivational interviewing sessions, which intensified anxiety in them, and thus, interfered with the results of intervention. Insufficient number of motivational interviewing sessions, number of subjects, and duration of study may have also been effective on this outcome.
No studies were found regarding the effectiveness of motivational interviewing on the health-promoting behaviors of patients with MS. Smith and Lanesskog evaluated the efficacy of motivational interviewing in improvement of the exercise experience for individuals with MS.[15] Their findings indicated that motivational interviewing can improve physical activity, which is one of the dimensions of the health-promoting behaviors, reduce fatigue, and increase the duration of exercise in these patients.[15] The results of this study support the results of the present study.
The results of the present study are also in line with the results of a study conducted by Bombardier.[16] Bombardier's findings indicated that motivational interviewing-based telephone counseling improved health-promoting behaviors and the dimensions of physical activity, stress management, and spiritual growth in individuals with MS after the intervention.[16]
Rajabipour et al. indicated that the implementation of group motivational interviewing significantly increased quality of life and all its dimensions in patients with permanent ostomy.[25] On the other hand, there is a positive correlation between quality of life and health-promoting behaviors.[26]
According to the results of a study by Navidian et al. on patients with obsessive-compulsive disorder (OCD), integration of the principles of group motivational interviewing with routine cognitive-behavioral therapy can improve symptoms of patients with OCD and promote their mental and spiritual health.[27] On the other hand, mental health promotion is effective on improvement of health-promoting behaviors.[28] Therefore, these results are consistent with the results of the present study.
In this regard, the findings of Poursharifi et al. indicated that group motivational interviewing as an effective intervention improves quality of life and self-care in patients with type II diabetes and is more effective in the area of self-care than group cognitive-behavioral training.[29] Ghasemipour et al. conducted a study with the aim of investigating the effectiveness of motivational interviewing on satisfying the basic psychological needs of patients who had undergone coronary artery bypass grafting.[17] The findings of this study showed that motivational interviewing was effective on satisfying the basic psychological needs of these patients and the better controlling of risk factors for CVD.[17] Satisfying the basic psychological needs of humans can improve their mental health and health-promoting behaviors.[28,30]
CONCLUSIONS
The results of this study indicated that motivational interviewing can improve health-promoting behaviors in patients with MS and provide valuable guidance to nurses regarding effective follow-up and improvement of health-promoting behaviors among patients with MS. One of the limitations of this study was its short duration, and therefore, the compactness of the motivational interviewing sessions. Based on the findings of this study, it is suggested that motivational interviewing be used as a low-cost and effective intervention in health care systems.
Financial support and sponsorship
The present study was funded by the Isfahan University of Medical Sciences, Isfahan, Iran.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
This article was derived from a master's thesis by Alireza Dashti with project number 393589 at the Isfahan University of Medical Sciences, Isfahan, Iran. We appreciate the assistance of the administrators of the Nursing and Midwifery Research Center and Clinical Research Development Center of Al-Zahra Hospital. Our sincere appreciation goes to the Research Deputy of Isfahan University of Medical Sciences, the respected hospital staff, and all the patients who participated in this study.
REFERENCES
- 1.Valery P, Ibiebele T, Harris M, Green AC, Cotterill A, Moloney A, et al. Diet, physical activity, and obesity in school-aged indigenous youths in northern Australia. J Obes. 2012;89:50–8. doi: 10.1155/2012/893508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cameron MH, Lord S. Postural control in multiple sclerosis: Implications for fall prevention. Curr Neurol Neurosci Rep. 2010 Sep;10:407–12. doi: 10.1007/s11910-010-0128-0. [DOI] [PubMed] [Google Scholar]
- 3.Asche C, Singer M, Jhaveri M, Chung H, Miller A. All-cause health care utilization and costs associated with newly diagnosed multiple sclerosis in the United States. J Manag Care Pharm. 2010;16:703–12. doi: 10.18553/jmcp.2010.16.9.703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Abedini M, Habibi Saravi R, Zarvani A, Farahmand M. Epidemiologic study of multiple sclerosis in Mazandaran, Iran, 2007. J Mazandaran Uni Med Sci. 2008;18:82–6. [Google Scholar]
- 5.Iran Multiple Sclerosis Society [Online] 2011. [Last viewed on 2014 Oct 03]. Available from: URL: http://www.iranms.ir .
- 6.MorowatiSharifabad M, Momeni Z, Eslami M, DehghaniTafti A, Hakimzadeh A. Study of Factors Associated with Self-Care Behaviors in Patients with Multiplesclerosis in Yazd City Based on Health Belief Model. Toloo-e- Behdasht journal. 2016;15:82–93. [Google Scholar]
- 7.Dehghani A, Mohammadkhan-Kermanshahi S, Memarian R. Educational needs of patients with multiple sclerosis of Tehran in 1389. Zahedan J Res Med Sci. 2012;14:1. [Google Scholar]
- 8.Heidari Sureshjani S, Eslami A, Hassanzadeh A. The quality of life among multiple sclerosis patients in Isfahan, Iran. Health Sys Res. 2011;7:571–9. [Google Scholar]
- 9.Mooney B, Timmins F, Byrne G, Corroon AM. Nursing students’ attitudes to health promotion to: Implications for teaching practice. Nurse Educ Today. 2011;31:841–8. doi: 10.1016/j.nedt.2010.12.004. [DOI] [PubMed] [Google Scholar]
- 10.Leuven K, Prion S. Health promotion in care directed by nurse practitioners. JNP. 2007;3:456–60. [Google Scholar]
- 11.Barry P. An overview of special considerations in the evaluation and management of the geriatric patient. Am J Gastroenterol. 2000;93:8–10. doi: 10.1111/j.1572-0241.2000.01697.x. [DOI] [PubMed] [Google Scholar]
- 12.Ayaz S, Tezcan S, Akıncı F. Health promotion behavior of students at the nursing college. Cumhuriyet Universitesi Hemsirelik Yuksekokulu. 2005;9:26–34. [Google Scholar]
- 13.Ossman S. Motivational interviewing: A process to encourage behavioral change. Nephrol Nurs J. 2004;31:31–3. [PubMed] [Google Scholar]
- 14.Miller W, Rollinick S. Motivational Interviewing. 2nd ed. New York: The Guilford Press; 2002. [Google Scholar]
- 15.Smith DC, Lanesskog D, Cleeland L, Motl R, Weikert M, Dlugonski D. Motivational interviewing may improve exercise experience for people with multiple sclerosis: A small randomized trial. Health Soc Work. 2012;10:99–109. doi: 10.1093/hsw/hls011. [DOI] [PubMed] [Google Scholar]
- 16.Bombardier C, Cunniffe M, Wadhwani R, Gibbons L, Blake K, Kraft G. The efficacy of telephone counseling for health promotion in people with multiple sclerosis: A randomized controlled trial. Arch Phys Med Rehabil. 2008;89:1849–56. doi: 10.1016/j.apmr.2008.03.021. [DOI] [PubMed] [Google Scholar]
- 17.Ghasemipour Y, Bahrami-Ehsan H, Abbaspour-Ghahremanlunejad S, Poursharifie H. The effectiveness of motivational interviewing on satisfying basic psychological needs of the patients under coronary artery bypass grafting (CABG) J Clin Psychol. 2011;2:43–53. [Google Scholar]
- 18.WHO. Mental health, Neurological Disorders: Public Health Challenges [Online] 2011. [Last viewed on 2014 Sep 10]. Available from: URL http://www.who.int/mental_health/neurology/atlas-ms-web.pdf .
- 19.Walker SN, Sechrit K, Pender NJ. 1 screens. [Last cited on 2014 Jul 28] [Last viewed on 2014 Sep 03]. Available from: http://www.unmc.edu/nursing/Health_Promoting_Lifestyle_Profile_II.htm .
- 20.Walker SN, Sechrit K, Pender NJ. The health promoting lifestyle profile; development and psychometric characteristics. Nurs Res. 1987;36:76–81. [PubMed] [Google Scholar]
- 21.Mohammadi Zeidi I, Pakpour Hajiagha A, Banafsheh Mohammadi Z. Reliability and validity of Persian version of the health-promoting lifestyle profile. J Mazand Univ Med Sci. 2012;22(Supple 1):103–13. [Google Scholar]
- 22.Scott NW, McPherson GC, Ramsay CR, Campbell MK. The method of minimization for allocation to clinical trials: A review. Control Clin Trials. 2002;23:662–74. doi: 10.1016/s0197-2456(02)00242-8. [DOI] [PubMed] [Google Scholar]
- 23.Navidian A. Practical plan motivational interviewing. In: Navidian A, Poursharifi H, editors. Motivational interviewing (Practical Guide) 1st Ed. Mashhad: Sokhan gostar; 2012. pp. 83–175. [Google Scholar]
- 24.Norouzinia R, Aghabarari M, Kohan M, Karimi M. Health promotion behaviors and its correlation with anxiety and some students’ demographic factors of Alborz University of Medical Sciences. JHPM. 2013;2:39–9. [Google Scholar]
- 25.Rajabipour E, Maddah S, Falahi Khoshknab M, Zarei F, Anaraki F. Effect of group motivational interviewing on quality of life of patients with colorectal cancer and permanent ostomy. Iran Nurs Sci Assoc. 2014;2:58–68. [Google Scholar]
- 26.Naghibi F, Golmakani N, mohair F. The Relationship between life style and the health related quality of life among the girl students of high schools in Mashhad, 2012-2013. IJOGI. 2013;16:9–19. [Google Scholar]
- 27.Navidian A, Haghshenas L, Abedi M, Baghban I. Comparing the effectiveness of group cognitive behavior therapy and its integration with motivational interviewing on symptoms of patients with obsessive-compulsive disorder. J Res Behave Sci. 2010;9:13–23. [Google Scholar]
- 28.Alpar SE, Senturan L, Karabacak U, Sabuncu N. Change in the health promoting lifestyle behaviour of Turkish University nursing students from beginning to end of nurse training. Nurs Educ Pract. 2008;8:382–8. doi: 10.1016/j.nepr.2008.03.010. [DOI] [PubMed] [Google Scholar]
- 29.Poursharifi H, Zamani R, Mehryar A, Besharat M, Rajab A. Effectiveness of motivational interviewing improving physical health outcome (weight loss and glycogenic control) in adult with type 2 diabetes. Contemp Psychol. 2011:3. [Google Scholar]
- 30.Sheldon KM, Elliot AJ, Kim Y, Kasser T. What is satisfying about satisfying events? Testing 10 candidate psychological needs. J Personality and Soc Psychol. 2001;80:325–39. doi: 10.1037/0022-3514.80.2.325. [DOI] [PubMed] [Google Scholar]