

Abstract
BACKGROUND
Children with severe disability often develop osteoporosis and have an increased risk of fracture. In Rett syndrome, the prevalence of fracture is four times greater than in the general population and the femur is commonly affected. This study used qualitative methods to investigate the regaining of mobility within 12 months following femoral fracture in Rett syndrome and parent caregiver experiences.
METHODS
Caregivers (n=14) of cases registered with the Australian Rett Syndrome Database with a daughter with Rett syndrome were recruited if their daughter sustained a femoral fracture between 2009 and 2014. Median (IQR) age at fracture was 11 years 4 months (8 years 8 months to 22 years 3 months). Qualitative methods were used to investigate parent/caregiver experiences and their daughter’s recovery following fracture. Themes in the interview data were identified with thematic analysis.
RESULTS
Operative management was chosen for those walking independently and non-operative management for most of the remaining. All who walked independently and one of the four who required assistance recovered pre-operative walking skills within 6 months. Themes identified by caregivers related to the complexities of pain recognition, the caregiver emotional journey and later rebuilding of relationships with service providers.
CONCLUSIONS
Those who walked with assistance were vulnerable to loss of this skill. Difficulties in pain recognition increased time to diagnose fracture and the acute episode was associated with heightened caregiver stress. Service providers can use family-centred practice models to support the strengthening of family functioning following this acute event that is surprisingly common in those with severe disability.
Keywords: Rett syndrome, fracture, rehabilitation, family stress, qualitative
INTRODUCTION
Children with severe disability experience functional limitations and often develop comorbidities including osteoporosis, and those with limited ambulation are at higher risk of osteoporosis and subsequent fracture than those who can walk independently (Henderson et al. 2010, Leet et al. 2006, McDonald et al. 2002, Ness & Apkon 2014). Fracture of the femur has potential to further impair gross motor skills (Wright 2000) but there is limited orthopaedic literature on the management of femoral fractures in children with severe disability. Non-operative management is generally favoured for conditions such as cerebral palsy (Wright 2000, Leet et al. 2009) where conservative management methods are often used, although the complication of malunion has been reported in approximately one third of children treated in this way (Leet et al. 2009). Use of external fixators for children with spasticity or seizures has also been recommended (Kirschenbaum et al. 1990), although there has been no evaluation of operative management of fractures in children with severe disability.
Rett syndrome is a severe X-linked neurodevelopmental disorder primarily affecting females (Neul et al. 2010). It is characterized by a period of relatively normal early development followed by regression of communication and/or hand function skills, and the development of abnormal gait and hand stereotypies (Neul et al. 2010). As for other severe disabilities, females with Rett syndrome are at increased risk of osteoporosis (Leonard et al. 1999, Motil et al. 2008, Jefferson et al. 2011). However, the prevalence of fracture is four times greater than that of a similarly aged female population with the femur most commonly affected (Downs et al. 2008). A population-based study found that occurrence of bone fracture during a previous two-year period was associated with poorer caregiver mental and physical health (Laurvick et al. 2006).
Whilst these data indicate that the occurrence of fracture affects maternal health, there are no data that describe the impact on the child’s function and wellbeing nor how families manage during the recovery period. Using in-depth family interviews, the current study explored the regaining of motor skills and family experiences following femoral fracture in females with Rett syndrome.
METHODS
The Australian Rett Syndrome Database (ARSD) was established in 1993 and has registered cases with Rett syndrome born since 1976 across Australia.(Fehr et al. 2011) Families/carers of females with Rett syndrome are invited to complete an initial questionnaire at the time of registration and follow-up surveys have been administered in at approximately biennial intervals since 2000 (Wong et al. 2014). By March 2015, data had been provided to the ARSD by family members of 388 girls and women, 73 (18.3%) of whom were deceased.
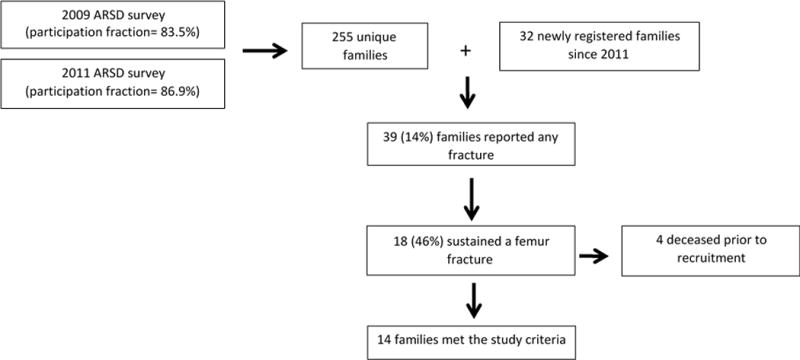
The 2009 and 2011 surveys included questions about the health and wellbeing of the child (eg occurrence of fractures) and family, and were completed by a total of 255 unique families. Participation fractions were 83.5% and 86.9% respectively for each of these waves of data collection. Thirty-two families registered with the ARSD after the 2011 family survey and three of those families also indicated to the research team that their daughter had sustained a femoral fracture. In total, the families of 39 females with a diagnosis of Rett syndrome confirmed genetically or using recent criteria (Neul et al. 2010) had reported the occurrence of a fracture in the previous six years. Almost half (n=18) were fractures of the femur. Four of these have since deceased, leaving 14 families (12 natural mothers, one foster mother and one grandmother) who were purposively invited and each agreed to participate (Fig. 1).
Fig 1.
The primary caregiver during the rehabilitative period was invited to participate in interviews that explored family experiences following fracture. The interview was a stem and leaf structure, using open-ended questions that allowed participants to describe experiences regarding diagnosis, management, and recovery. Probing questions aimed to reduce inferences of emotion and instead collect observable behaviours and contextual factors. The probing questions included: “How do you know this?” and “Can you describe this to me?” Interviews were conducted by TH and JD, digitally recorded, transcribed and sent to the participants for member checking. Twelve (85.7%) caregivers returned checked transcripts and made no changes to the original transcript. Data from the ARSD were interrogated to provide supplementary information including mutation type, if menarche had occurred prior to the fracture, demographic details of residence and the caregiver’s highest achieved education.
Ethical approvals for this study were obtained by the Human Research Ethics Committee at Princess Margaret Hospital for Children, Western Australia (1909EP) and the Curtin University Human Research Ethical Committee (RDHS-03-14). Informed consent was obtained by the primary caregivers before participating in this study.
Statistical analysis
Thematic analysis of the written interview transcripts was conducted to identify events, themes and concepts that arose in the written transcripts (TH, JD). The audio recordings were transcribed within 24 to 48 hours of the interview to ensure accurate transcription. Data were coded to identify the themes and concepts. For increased credibility and validity, the themes and concepts were discussed in detail with the investigative team for consensus of interpretation until agreement on the themes was reached. Qualitative software, NVivo10, was used to support the analysis of the data.
RESULTS
The median (interquartile range [IQR]) age of the child at the time of fracture was 11 years 4 months (8 years 8 months to 22 years 3 months), and their median (IQR) age at the time of interview was 15 years 8 months (10 years 9 months to 26 years 3 months). Prior to fracture, seven individuals, including three who could walk independently and four who required assistance, had the capacity to walk. The remaining seven individuals were totally wheelchair dependent. The characteristics of the girls and women with Rett syndrome and their caregivers are shown in Table 1.
Table 1.
Distribution of descriptive characteristics for each of the girls and women who sustained a femoral fracture and their families (n = 14).
| Characteristics | n (%) | |
|---|---|---|
| Mutation type | C-terminal deletion | 2 (14%) |
| Early truncating | 1 (7%) | |
| Large deletion | 1 (7%) | |
| p.Arg168* | 1 (7%) | |
| p.Arg255* | 1 (7%) | |
| p.Arg270* | 1 (7%) | |
| p.Arg294* | 2 (14%) | |
| p.Thr158Met | 1 (7%) | |
| Other | 3 (21%) | |
| Negative | 1 (7%) | |
| Residence at time of fracture | Parental home | 9 (64%) |
| Grandparent home | 1 (7%) | |
| Foster home | 1 (7%) | |
| Group home | 3 (21%) | |
| Remoteness Area (ARIA classificationa) | Major city of Australia | 11 (79%) |
| Inner regional Australia | 3 (21 %) | |
| Outer regional Australia | – | |
| Remote or very remote Australia | – | |
|
| ||
| Age group at time of fracture | 0–7 years | 3 (21%) |
| 7–12 years | 5 (36%) | |
| 13–18 years | 2 (14%) | |
| >18 years | 4 (29%) | |
| Mobility level | Independent walking | 3 (21%) |
| Walking with assistance | 4 (29%) | |
| Wheelchair dependent | 7 (50%) | |
| Previous fracture | Yes | 4 (29%) |
| No | 10 (71%) | |
| Pubertal status | Pre-menarche | 10 (71%) |
| Post-menarche | 4 (29%) | |
| Caregiver’s highest achieved education | University degree | 6 (43%) |
| Vocational qualification | 4 (29%) | |
| High school year 12 | 1 (7%) | |
| Some high school | 3 (21%) | |
accessibility/Remoteness Index of Australia
A fractured femur was diagnosed on the day of the injury for six individuals and on the following day for four. Three were diagnosed 3–6 days post-injury and one after one week. The reported mode of injury was trauma from falling (n=4) or trivial activities (n=4) such as range of motion exercises or repositioning in bed. The mode of injury for the remaining fractures was unknown. Operative management was provided for all who walked independently and one of four who walked with assistance. The remaining girls and women were managed non-operatively. The median (range) length of hospital stay overall was 3 days (0 to 51 days) for those managed operatively it was 31.5 days (14 to 51 days), and for those managed non-operatively it was 1 day (0 to 1 day).
Caregiver satisfaction in relation to the acute management of their daughter’s fracture was mostly positive. In contrast, three caregivers felt their daughter endured unnecessary pain caused by delays in identifying and managing the fracture. Families were generally satisfied with clear explanations of management and reassurances of recovery. However, some parents reported disappointment in the lack of knowledge of Rett syndrome amongst hospital staff and felt that this contributed to reduced levels of pain and therapy management.
All three of the girls who were independent ambulators pre-fracture regained this ability within 6 months post-fracture. Three of the four assisted-ambulators failed to return to their pre-fracture mobility status by 12 months, including the girl treated operatively. One of these became wheelchair dependent. Of these, one girl refused to walk; one mother was fearful her daughter would fracture again and declined rehabilitation; and one mother lacked confidence to support her daughter’s assisted walking. The individual who recovered her assisted walking level did so by 6-months and was managed non-operatively.
Three themes were identified from the interviews including complexities of pain recognition, the emotional journey of caregivers, and rebuilding relationships with service providers.
The complexities of pain recognition
Caregivers described a range of physical and behavioural symptoms that assisted with recognition that their daughter was in pain (Table 2) but these were often difficult to interpret with delayed diagnosis in some cases. Four caregivers reported their daughter had an increased tolerance to pain which they felt had contributed to delayed diagnosis. Four caregivers initially assumed the source of pain was in soft tissue structures and attempted to self-manage the injury at home. ‘I thought she pulled a muscle. I didn’t think she broke her leg because there wasn’t that much force put on her leg’.
Table 2.
Sample quotes describing parent reported recognition of fracture pain.
| Pain recognition | Sample quotes describing pain expression | |
|---|---|---|
| Physical | Breath holding and gulping air | ‘She was holding her breath like she was in extreme pain’ ‘Her stomach was swollen…they put it down to gulping air and being in so much pain’ |
| Body expression | ‘Every time we moved her she screamed and she would convulse again and not in a seizure way but she would convulse so much it looked similar to a seizure’ ‘When we over stretched her she gets very wide eyed and her tremors get worse’ ‘She seemed to have spasms as soon as we touched her legs’ ‘We were moving her around she would flinch and she wouldn’t really cry out but she would sort of flinch and wince’ ‘She would wiggle, she would do a pelvic thrust to show you she is uncomfortable’ |
|
| Vocalisation | ‘She was screaming in a way that we have not heard her cry before’ ‘She is very passive and quiet and it was the first time in her life and my life I ever heard her make a distinct noise’ |
|
| Eye gazing | ‘Communicating with her eyes, it gives us a good indication with a begging look or a happy look. She’s almost telling you everything with her eyes’. | |
| Facial expressions | ‘As I moved her hips she woke up with that very same wide eyed shaking expression…I had no idea it could have been her femur fractured’ ‘She doesn’t have that much movement of her forehead even when she frowns she very slightly gets a farrow in her forehead but with this her forehead was farrowing up and I’ve never seen her face so pained’ |
|
| Swelling | ‘By that stage the knee had swollen and it was concerning me something had wrenched on her knee. Maybe another child’ | |
| Behavioural | Sleeping | ‘Going off to sleep constantly was very new for her and I think it was that she was just in total shock and was trying to block it out’ ‘She did not sleep that night and we had to give her pain medication and a sedative to sleep’ |
| Change in mood | ‘Very quiet and not really smiling, to me that is showing signs of discomfort’ ‘She is so happy all the time, her whole persona changed dramatically in the space of two days’ |
The differential diagnosis during medical examination was also challenging. Caregivers reported that hospital medical teams identified the femur fracture by swelling, heat, redness, and X-ray investigation. Two mothers observed that the medical teams had difficulty interpreting X-rays due to low bone density and requested additional specialist opinion. One girl’s diagnosis was delayed as the pain was thought to be visceral in origin. One general practitioner prescribed pain medications without additional investigations. ‘The doctor said you can give her suppository pain killers, bring her back in a couple of days… if you feel there is a need to have an x-ray done you can go have an x-ray’.
The emotional journey of caregivers
Caregivers reported increased emotional stress during the acute period, describing guilt, anger, shock and fears surrounding lost mobility and the potential for future fractures.
Caregivers whose daughter was in their care at the time of fracture felt responsible for the injury. ‘Pretty guilty because I knew it most likely was me that had done it…there is that initial oh my goodness I just broke my child’s leg’. Other caregivers felt guilt (n=9) when they had known something was wrong but were unsure about the seriousness of injury and continued their daily routines. ‘My first thought was I am a terrible mother because I let my child go for the whole week with a broken femur’.
Feelings of anger were common amongst mothers whose daughter was in the care of others when the injury occurred. At the time of the femur fracture, five females were in the care of a community respite service and one was at school. Half of these mothers were concerned that lack of care or skill had contributed to their daughters sustaining their femur fracture. ‘Very angry because she is usually very careful…the initial version I got from the staff that she had fallen out of bed’.
Many felt shock that a femur fracture could occur with minimal force. ‘Devastated that this happened over something so minor. If it happened over a trauma I would have expected it, but this was a movement she did everyday’. Others found it difficult to comprehend that lower limb fractures could occur in non-ambulating girls. ‘How can this happen because she can’t stand? Totally shocked’. Many caregivers reported very limited knowledge prior to the fracture occurring regarding bone health in children who did not walk. ‘How could she break her bone the femur? It is supposed to be the strongest bone in the body’.
The caregivers expressed fear in relation to the risk of their daughter losing mobility. ‘My biggest fear was that she would not get her mobility back because I know Rett syndrome girls tend to lose their mobility. So I thought that was the end of that’. Following fracture, seven caregivers felt anxiety for the risk of further fractures after the femur had healed. ‘They are at a high risk, not necessarily Rett syndrome but any non-mobile child has a higher risk of a fracture’. Fear of future fractures influenced one mother’s decision to delay recommencement of mainstream childcare for her daughter. ‘They usually sleep her on the floor with other kids walking around her, I was nervous going to childcare so I had to take carers’ leave’.
All caregivers whose daughters received non-operative management needed assistance due to added weight and awkwardness of a leg cast or splint. This created additional burden that needed to be managed alongside the needs of other children and family members. Emotional stress levels were heightened during the recovery period. One mother was unaware of support services available; one family reported their respite centre was unable to provide an immediate service when it was required; and another mother felt she had no choice but to return her daughter to school as she was unable to stop working due to financial reasons. Others felt overwhelmed by the burden of fracture and post-fracture rehabilitation. ‘I don’t think anything helped with the physical burden really it just was what it was and you had to deal with it’. Recommended strategies to reduce physical and emotional stress are summarised in Table 3.
Table 3.
Sample quotes describing caregivers’ recommended strategies to reduce physical and emotional stress
| Theme | Advice to other families | |
|---|---|---|
| Child Related | Pain management regimen | ‘She was in a lot of pain which was tough so I guess better pain management would have made it easier. ‘Make sure there is good pain management straight away because we weren’t given any help on what to do’ |
| Change of scenery | ‘Wheeling her out with you into the garden to have a change of scenery. That will clear your head’ | |
| The right equipment | ‘Definitely the couch that is on wheels. It was comfortable for her and it supported her knee well, that was amazing help’ ‘Keep them the most comfortable as possible. Use pillows underneath the plaster whilst in bed to make it comfortable’ |
|
| Reestablishment of routine | ‘When she was in less pain it was easier to take her out. We could even take her to restaurants in her splints so we still tried to have some normality to life’ ‘She gets terribly bored. I knew she had to go back to kinder in that 6 weeks and I think it benefited her keeping interactive’ ‘I think it’s getting back to the normal environment they are used to living in’ |
|
| Rehabilitation | ‘Gentle range of motion of her upper body because she confined to the bed the whole time’ ‘If you can keep her busy and distracted so she has something to do while standing she will last longer’ ‘Having support from physio and carer support will help the child to recover quicker rather than having them in hospital’ |
|
| Parent Related | Breaks from caring | ‘World of good when you get out the house. Also just being kind to yourself and having little breaks and getting much sleep as you can. Quite often when she went to sleep during the day I would sleep. Not much around the place got done’ ‘A good routine of carers and have back-up friends and family who are pretty good’ ‘It doesn’t have to be a great length of time or an expensive activity. It could be a swim or a walk. Life doesn’t have to evolve around the girls. Well it does but you do need to do activities for yourself.’ |
| Social network | ‘Kinder is amazing because we get to speak to other parents there as well’ ‘Rett mums worldwide have a page called My Daughter has Rett syndrome’ |
|
| Support from partner | ‘I couldn’t manage without Pop though. Even now he is very good he helps me a lot with her’ ‘My husband and I are good at taking turns to relieve the burden on one person’ ‘Make sure you have plenty of support around you that is the biggest issue. It is a big task’ |
|
| Helpful organisations | ‘The one thing that did help me though was the fact I was able to talk to (organisation) that gave me a lot of confidence’ |
Rebuilding relationships with service providers
There was often strain in relationships with professionals from respite services or school settings if the fracture had occurred in those settings. Some caregivers were concerned that they had not been provided with all details of the injury and these relationships took time to rebuild. ‘They used to pick her up on Saturdays for a few hours, that was all the help until I was sure they were going to look after her and not hurt her anymore’. Some felt the care staff needed more education and training in relation to bone health for those with severe disability. For others, good rapport was maintained in relation to the ongoing care relationships with successful ingredients including clear and honest communication with staff members.
One fracture occurred during school hours. The caregiver reported not receiving information regarding the incident which delayed the time for diagnosis. Later discussions of the injury were difficult to organise and this caregiver felt the professional relationship was weakened. ‘I demanded a meeting at the school, the principal didn’t come and I was utterly disappointed’. However, the majority of caregivers whose daughter attended school had positive experiences when returning. ‘At her school, they really are great and are used to kids coming in with many sorts of injuries. They know how to support them’. Rebuilding trust and confidence was facilitated by familiar staff and capacity to support participation in the day to day school activities in a graded fashion.
DISCUSSION
Osteopenia and fracture occurs commonly in Rett syndrome (Downs et al. 2008, Jefferson et al. 2011, Leonard et al. 1999, Motil et al. 2008) yet many of the caregivers had minimal prior knowledge of the risks of poor bone health prior to the fracture. In our study, more than three quarters who sustained a femur fracture were unable to walk independently, consistent with findings that ambulatory impairment is a determinant for poorer bone health in Rett syndrome (Gonnelli et al. 2008, Jefferson et al. 2015, Roende et al. 2011). Non-operative management was more likely chosen for those with limited ambulation skill although currently, no literature articulates the clinical reasoning for these management decisions. Recovery of ambulation skills was more likely for those walking independently with those who required assistance to walk being vulnerable to losing this skill, regardless of the mode of orthopaedic management. Assisted ambulation has been associated with a gentler trajectory of scoliosis compare to those unable to walk (Downs et al. in press) and is associated with benefits for quality of life (Epstein et al. in press). The development of clinical strategies that prevent avoidable loss of assisted ambulation is an important topic of future research.
Inability to self-report pain creates barriers for injury identification and in Rett syndrome, caregivers have previously indicated uncertainty as to whether their daughter had pain (Symons et al. 2013). This influenced early detection of injury. Expression of pain was variable, often subtle, and ranged from alterations in moods, sleeping patterns, facial expressions, body expressions and vocalisations. With the exception of breath holding these signs of distress are supported by previous findings (de Knegt et al. 2013). In our study, caregivers felt that their daughter’s high pain tolerance (Downs et al. 2010) created further uncertainty as to the presence of pain. Together, these findings suggest that each child demonstrates a distinct pattern of behaviours in response to pain consistent with the notion of a pain signature (Regnard et al. 2007). Furthermore, almost a third fractured their femur during trivial activity highlighting a vulnerability to low-energy fractures (Roende et al. 2011). We suggest the high propensity to fracture and difficulty of its recognition justify a low threshold for investigation of fractures in this population taking into account subtle and often very individual changes in behaviour.
Our study confirmed previous findings that caregiver health can be affected by bone fracture (Laurvick et al. 2006) and we also identified specific factors which contributed to heightened stress. Clinicians working in acute settings need to be aware of the emotional distress experienced by caregivers when their child sustains a femoral fracture and the increased physical burden of caring for their child during non-operative management. The professional relationships between service providers and caregivers were often strained if the fracture occurred at school or respite, and lack of trust and confidence with service providers sometimes prevented caregivers from using services that could potentially relieve their emotional distress and physical burden. Health care and service providers play a key role in family-centred practice that aims to strengthen the functioning of the family (Espe-Sherwindt 2008). There are many roles following femoral fracture in Rett syndrome including education in relation to bone health and its management; ensuring that families have access to appropriate equipment to reduce physical burden; and provide advice regarding pain regimens and any necessary rehabilitation; each of which were essential in relieving family stress.
Despite Rett syndrome being a rare disorder, the ARSD allowed identification of all Australian females with Rett syndrome who had had a femur fracture since 2009. With full recruitment from the population-based sample, our study was representative of both child and family characteristics. By employing probing questions concerning family events, we were able to more accurately determine the detail of the course of recovery of mobility skills. The high member checking fraction response also enhanced data accuracy. Restriction to fracture episodes occurring within the past 5 years reduced recall error but some was likely to still exist over this timeframe. We acknowledge that the primary caregiver’s appraisal of the fracture management regime was valuable. However, full interpretation would require access to medical notes which may provide the clinical reasoning for the chosen management.
Our paper extends knowledge of femoral fracture management and recovery in Rett syndrome. Each child can have unique pain expression and/or high pain tolerance which can influence the caregiver’s decision to seek immediate medical advice and thereafter clinician recognition of fracture. Greater mobility impairment appears to influence clinicians to favor non-operative management and further research is required to investigate clinical benefits of management choice for femur fractures in children with severe disability. Independent walking was regained after fracture but those who required assistance to walk were most at risk of losing mobility. The data highlighted the need for specific education regarding Rett syndrome, bone health and fracture for service providers and clinicians who could then provide targeted practical advice to relieve caregiver stress.
Key messages.
Pain recognition in Rett syndrome can be complex and lead to delayed diagnosis of femoral fracture.
Operative management was chosen for those with independent walking skills and non-operative for those requiring assistance or without mobility.
Recovery of pre-fracture mobility status occurred within a 6-month period for those who walked independently.
There is a need for better clinical understanding of parent/caregiver stress in reponse to their daughter’s fracture.
Acknowledgments
We express our gratitude to all the families and carers of females with Rett syndrome who have contributed to the Australian Rett syndrome Database. We thank those families who participate in the Australian Rett syndrome study and gave their time and thoughts for the interviews. We gratefully acknowledge the support from Adjunct Professor Diana Hopper and Dr Robyn Fary for their enthusiasm and passion in the role as Honours Coordinators to guide this paper to its maximal potential. We thank the Australian Paediatric Surveillance Unit (APSU) for collaboration in case ascertainment. We also thank Bill Callaghan and the Rett syndrome Association of Australia for their essential contribution over the years in regards to case ascertainment. We acknowledge our gratitude to the National Institutes of Health (5R01HD043100-05) and the National Health and Medical Research Council (NHMRC) project grants #303189, and #1004384 and an NHMRC program grant #572742 for funding the ARSD since it was established in 1993. The funding bodies for this study have not been involved in study design, data collection, data analysis, manuscript preparation and/or publication decisions.
Contributor Information
Thomas Horne, Physiotherapist, School of Physiotherapy and Exercise Science, Curtin University, GPO Box U1987, Perth, 6845, Australia.
Helen Leonard, Principal Research Fellow, Telethon Kids Institute, The University of Western Australia, PO Box 855, West Perth, 6872, Australia.
Katherine Stannage, Head of Orthopaedics, Princess Margaret Hospital, Roberts Rd, Subiaco, WA, 6008, Australia.
Jenny Downs, Telethon Kids Institute, The University of Western Australia, PO Box 855, West Perth, 6872, Australia; School of Physiotherapy and Exercise Science, Curtin University, GPO Box U1987, Perth, 6845, Australia.
References
- De Knegt NC, Pieper MJ, Lobbezoo F, Schuengel C, Evenhuis HM, Passchier J, Scherder EJ. Behavioral pain indicators in people with intellectual disabilities: a systematic review. Journal of Pain. 2013;14:885–896. doi: 10.1016/j.jpain.2013.04.016. [DOI] [PubMed] [Google Scholar]
- Downs J, Bebbington A, Woodhead H, Jacoby P, Jian L, Jefferson A, Leonard H. Early determinants of fractures in Rett syndrome. Pediatrics. 2008;121:540–546. doi: 10.1542/peds.2007-1641. [DOI] [PubMed] [Google Scholar]
- Downs J, Geranton SM, Bebbington A, Jacoby P, Bahi-Buisson N, Ravine D, Leonard H. Linking MECP2 and pain sensitivity: the example of Rett syndrome. American Journal of Medical Genetics Part A. 2010;152A:1197–1205. doi: 10.1002/ajmg.a.33314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Downs J, Torode I, Wong K, Ellaway C, Elliott EJ, Christodoulou J, Jacoby P, Thomson MR, Izatt MT, Askin GN, Mcphee BI, Bridge C, Cundy P, Leonard H. The natural history of scoliosis in females with Rett syndrome. Spine. doi: 10.1097/BRS.0000000000001399. (in press) [DOI] [PubMed] [Google Scholar]
- Epstein A, Leonard H, Davis E, Williams K, Reddihough D, Murphy N, Whitehouse A, Downs J. Conceptualizing a quality of life framework for girls with Rett syndrome using qualitative methods. American Journal of Medical Genetics Part A. doi: 10.1002/ajmg.a.37500. (in press) [DOI] [PubMed] [Google Scholar]
- Espe-Sherwindt M. Family-centred practice: collaboration, competency and evidence. Support Learn. 2008;23:136–143. [Google Scholar]
- Fehr S, Bebbington A, Nassar N, Downs J, Ronen GM, De Klerk N, Leonard H. Trends in the diagnosis of Rett syndrome in Australia. Pediatric Research. 2011;70:313–319. doi: 10.1203/PDR.0b013e3182242461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gonnelli S, Caffarelli C, Hayek J, Montagnani A, Cadirni A, Franci B, Lucani B, Rossi S, Nuti R. Bone ultrasonography at phalanxes in patients with Rett syndrome: a 3-year longitudinal study. Bone. 2008;42:737–742. doi: 10.1016/j.bone.2007.12.003. [DOI] [PubMed] [Google Scholar]
- Henderson RC, Berglund LM, May R, Zemel BS, Grossberg RI, Johnson J, Plotkin H, Stevenson RD, Szalay E, Wong B, Kecskemethy HH, Harcke HT. The relationship between fractures and DXA measures of BMD in the distal femur of children and adolescents with cerebral palsy or muscular dystrophy. Journal of Bone and Mineral Research. 2010;25:520–526. doi: 10.1359/jbmr.091007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jefferson A, Fyfe S, Downs J, Woodhead H, Jacoby P, Leonard H. Longitudinal bone mineral content and density in Rett syndrome and their contributing factors. Bone. 2015;74:191–198. doi: 10.1016/j.bone.2015.01.023. [DOI] [PubMed] [Google Scholar]
- Jefferson AL, Woodhead HJ, Fyfe S, Briody J, Bebbington A, Strauss BJ, Jacoby P, Leonard H. Bone mineral content and density in Rett syndrome and their contributing factors. Pediatric Research. 2011;69:293–298. doi: 10.1203/PDR.0b013e31820b937d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirschenbaum D, Albert MC, Robertson WW, Jr, Davidson RS. Complex femur fractures in children: treatment with external fixation. Journal of Pediatric Orthopaedics. 1990;10:588–591. doi: 10.1097/01241398-199009000-00003. [DOI] [PubMed] [Google Scholar]
- Laurvick CL, Msall ME, Silburn S, Bower C, De Klerk N, Leonard H. Physical and mental health of mothers caring for a child with Rett syndrome. Pediatrics. 2006;118:e1152–1164. doi: 10.1542/peds.2006-0439. [DOI] [PubMed] [Google Scholar]
- Leet AI, Mesfin A, Pichard C, Launay F, Brintzenhofeszoc K, Levey EB, Sponseller PD. Fractures in children with cerebral palsy. Journal of Pediatric Orthopaedics. 2006;26:624–627. doi: 10.1097/01.bpo.0000235228.45539.c7. [DOI] [PubMed] [Google Scholar]
- Leet AI, Shirley ED, Barker C, Launay F, Sponseller PD. Treatment of femur fractures in children with cerebral palsy. Journal of Children’s Orthopaedics. 2009;3:253–258. doi: 10.1007/s11832-009-0191-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leonard H, Thomson MR, Glasson EJ, Fyfe S, Leonard S, Bower C, Christodoulou J, Ellaway C. A population-based approach to the investigation of osteopenia in Rett syndrome. Developmental Medicine and Child Neurology. 1999;41:323–328. doi: 10.1017/s0012162299000717. [DOI] [PubMed] [Google Scholar]
- Mcdonald DG, Kinali M, Gallagher AC, Mercuri E, Muntoni F, Roper H, Jardine P, Jones DH, Pike MG. Fracture prevalence in Duchenne muscular dystrophy. Developmental Medicine and Child Neurology. 2002;44:695–698. doi: 10.1017/s0012162201002778. [DOI] [PubMed] [Google Scholar]
- Motil KJ, Ellis KJ, Barrish JO, Caeg E, Glaze DG. Bone mineral content and bone mineral density are lower in older than in younger females with Rett syndrome. Pediatric Research. 2008;64:435–439. doi: 10.1203/PDR.0b013e318180ebcd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ness K, Apkon SD. Bone health in children with neuromuscular disorders. Journal of Pediatric Rehabilitation Medicine. 2014;7:133–142. doi: 10.3233/PRM-140282. [DOI] [PubMed] [Google Scholar]
- Neul JL, Kaufmann WE, Glaze DG, Christodoulou J, Clarke AJ, Bahi-Buisson N, Leonard H, Bailey ME, Schanen NC, Zappella M, Renieri A, Huppke P, Percy AK. Rett syndrome: revised diagnostic criteria and nomenclature. Annals of Neurology. 2010;68:944–950. doi: 10.1002/ana.22124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Regnard C, Reynolds J, Watson B, Matthews D, Gibson L, Clarke C. Understanding distress in people with severe communication difficulties: developing and assessing the Disability Distress Assessment Tool (DisDAT) Journal of Intellectual Disability Research. 2007;51:277–292. doi: 10.1111/j.1365-2788.2006.00875.x. [DOI] [PubMed] [Google Scholar]
- Roende G, Ravn K, Fuglsang K, Andersen H, Vestergaard A, Brondum-Nielsen K, Jensen JE, Nielsen JB. Patients with Rett syndrome sustain low-energy fractures. Pediatric Research. 2011;69:359–364. doi: 10.1203/PDR.0b013e31820bc6d3. [DOI] [PubMed] [Google Scholar]
- Symons FJ, Byiers B, Tervo RC, Beisang A. Parent-reported pain in Rett syndrome. Clinical Journal of Pain. 2013;29:744–746. doi: 10.1097/AJP.0b013e318274b6bd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wong K, Leonard H, Jacoby P, Ellaway C, Downs J. The trajectories of sleep disturbances in Rett syndrome. Journal of Sleep Research. 2014 doi: 10.1111/jsr.12240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright JG. The treatment of femoral shaft fractures in children: a systematic overview and critical appraisal of the literature. Canadian Journal of Surgery. 2000;43:180–189. [PMC free article] [PubMed] [Google Scholar]