

Abstract
Objectives
To investigate whether adult patients with unilateral developmental dysplasia of the hip (UDDH) have pelvic asymmetry and what correlation existing between them.
Methods
A total of 100 adult patients with UDDH were enrolled in the retrospective observational study in Shanghai Jiaotong University Affiliated Sixth People’s Hospital, Shanghai, China, between January 2012 and February 2014. The anteroposterior pelvic radiographs were reviewed and the pelvic heights and ischium heights were measured and compared between the affected and non-affected sides to find out the relationship between the pelvic morphology and hip dysplasia.
Results
The pelvic heights demonstrated significant differences between the non-affected side and the affected side in patients with Crowe type II-IV UDDH (p<0.05), but not in patients with Crowe type I UDDH (p=0.09). There were significant differences in the bilateral ischium heights in patients with Crowe type III and IV UDDH (p<0.05), but not in patients with Crowe type I and II UDDH (p=0.78, p=0.055). In addition, the degree of hip dysplasia was positively associated with the degrees of asymmetry of pelvis (r=0.78, p<0.001) and ischium (r=0.72, p<0.001) in UDDH patients.
Conclusion
The pelvic asymmetry exists in adult patients with UDDH. In addition, the degree of asymmetry has correlation with the degree of hip dysplasia. We recommend that it should be taken more cautions to use teardrops and ischial tuberosity as anatomy landmarks to balance leg-length discrepancy for unilateral DDH patients in preoperative planning and total hip arthroplasty.
Developmental dysplasia of the hip (DDH) is a common disease of hip joint in Asia, whose incidence in infants is 1/1000 far higher than that in Western countries. Unilateral developmental dysplasia of the hip (UDDH) in adults is continuation of the same disease in infants and children.1 Therefore, it is composed of several morphological abnormalities caused by dysplasia changes including insufficient coverage of the femoral head, shallow acetabulum, increased femoral anteversion, coxa valga, and shortening of the femoral neck.2-5 Some authors have reported that developmental retardation affects not only the acetabulum, but also the entire pelvis.6,7 However, few studies have been focused on the morphological changes of the entire pelvis in this condition. Total hip arthroplasty (THA) has been reported to be the most successful procedure for patients with symptomatic end-stage arthritis secondary to DDH, providing a high success rate of functional improvement, leg-length balancing, and pain relief.8-11 In addition, equalization of leg length following THA, is an important reconstructive criteria. A review of the global literatures revealed that the anatomic deformity of the femur and acetabular contributed to leg length discrepancy.12-14 However, it is unclear whether DDH patients’ pelvic morphology contributes to leg length discrepancy. In order to better understand the pathogenesis of DDH, it is important to know whether and how it impacts the entire pelvis. In addition, such knowledge may be useful when considering the corrective maneuver to optimize the acetabular position and leg length balancing during THA. Therefore, we conducted this study to determine the morphology of pelvis in adult patients with UDDH. We were trying to find out whether adult patients with UDDH have pelvic asymmetry, and whether there was a correlation between the degrees of asymmetry and Crowe classification.
Methods
We reviewed the anteroposterior pelvis films of 100 patients who were diagnosed with UDDH. All the films were taken in Shanghai Jiaotong University Affiliated Sixth People’s Hospital, Shanghai, China between January 2012 and February 2014, including 78 female and 22 male. The average age is 56.3 years (range 21-79 years). Our selection criteria are as follows: 1) the diagnosis was UDDH, not accompanied by other congenital or acquired deformities of the hip joint. 2) ages were more than 18 years, 3) the anteroposterior pelvic radiographs were taken as patients lay supinely while the lower extremities were kept straight and rotated 15-20° internally with the femoral neck parallel to the film.
Exclusion criteria were patients who had undergone surgery in the affected hip before, or who suffered from Charcot’s joint disease, with infection, history of trauma.
We used the Crowe classification,15 based on the degrees of subluxation of the femoral heads out of the true acetabulum, which is associated especially well with the magnitude and pattern of anatomic deformation of dysplastic hips. The vertical subluxation is measured as the vertical height from the reference line (through the radiographic teardrops) to the femoral head-neck junction. The “degree of subluxation” is then calculated as percentage subluxation=[(the amount of vertical subluxation)/(the vertical height of the true acetabulum)]×100. In this classification, type I hips have less than 50% subluxation; type II, 50-74%; type III, 75-100%; and type IV, more than 100% (Figure 1).
Figure 1.
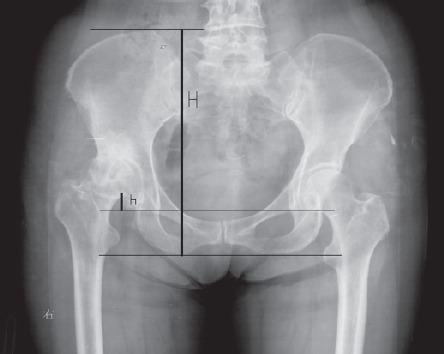
Anteroposterior pelvis films showing the anatomic deformation of dysplastic hips. h - the vertical height from the reference line (through the radiographic teardrops) to the femoral head-neck junction, H - the vertical height of the pelvis, the vertical height of the true acetabular = 1/5H. The “degree of subluxation” is then calculated as percentage subluxation= [(the amount of vertical subluxation)/(the vertical height of the true acetabulum)] ×100.
The definitions of parameters
We used preoperative pelvic radiographs in the supine position to determine the heights of pelvis and ischium. The height of pelvis is the distance between the highest point of the iliac crest to the line across the bottom edges of the bilateral ischial tuberosity. The ischium height is the distance from the teardrop to the line across the bottom edges of bilateral ischial tuberosity. All measurements were performed by 2 investigators at a 2-week interval. We assessed the intra-observer variabilities for all the parameters and determined that they were relatively low with no significant differences. We decided to use the average of the 2 measurements of each parameter for further analysis (Figure 2).
Figure 2.

Anteroposterior pelvis films showing the anatomic deformation of dysplastic hips. H - pelvic height (the distance between the highest point of the iliac crest to the line across the bottom edges of the bilateral ischial tuberosity), L - ischium height (the distance from the teardrop to the line across the bottom edges of bilateral ischial tuberosity).
The data analysis was performed by using IBM SPSS Version 20.0 (SPSS, Chicago, USA). The paired t-test was used to compare between the affected side and the non-affected side. One-way analysis of variance was performed to determine the differences among 4 types of Crowe classification. A p<0.05 was considered statistically significant.
Results
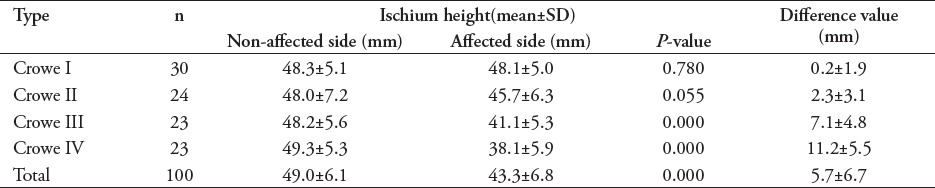
We found significant differences existing between the non-affected and affected sides in patients in the Crowe II, III, IV subgroups, but not in Crowe I subgroup (p=0.09). From Crowe type I to IV, the difference values of the pelvic heights were 1.9 mm, 8.2 mm, 12.8 mm, and 18.7 mm, in which there were significant differences (F=71.35, p=0.00). As the degrees of hip dysplasia were increasing, the pelvic heights increased on the non-affected side and decreased on the affected side, resulting in continuously increasing difference values (D-values) of bilateral pelvic heights (Table 1). With regard to the ischium heights, the DDH-side were significantly different from the healthy-side for types IV ((p=0.000) and III (p=0.000), but not for types II (p=0.055) and I (p=0.780). For all patients, the ischium heights were 49.0 mm and 43.3 mm between the non-affected side and the affected side (p=0.000). The mean difference values were 0.2 mm in Crowe I, 2.3 mm in Crowe II, 7.1 mm in Crowe III, and 11.2 mm in Crowe IV patients (F=96.48, p=0.00). With the degrees of hip dysplasia were increasing, the ischium heights on the non-affected side were constant while they were decreasing on the affected side, resulting in continuously increasing D-values of bilateral ischium heights (Table 2).
Table 1.
Pelvic heights among 4 types of Crowe classification.
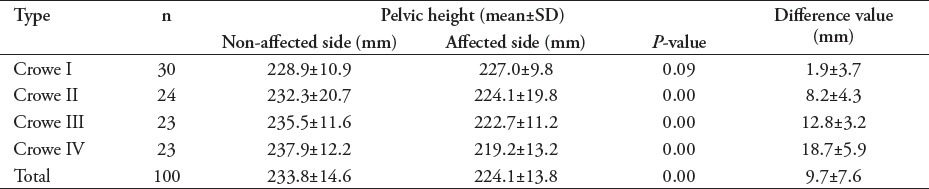
Table 2.
Ischium heights among 4 types of Crowe classification.
We analyzed the correlation of this asymmetry with the degrees of hip dysplasia. The correlation coefficients between the degrees of hip dysplasia and the D-values of pelvic was 0.78 (p=0.000) and ischium heights was 0.72 (p=0.000). It appeared to be a trend that the more degrees of hip dysplasia, the greater pelvic and ischium asymmetry.
Discussion
Every patient with DDH has unique anatomic abnormalities of both the acetabulum and the proximal femur. The acetabulum of the dysplastic hip is found shallow, sloping and narrow and the changes of femur include proximal femur stenosis, shrunken femoral head, femoral neck length loss, and so on.4,16-18 The anatomic abnormalities of hips lead to follows: 1) biomechanical changes of the dysplastic hip joint; 2) shortening of the leg length on the affected side, 3) joint pain and dysfunction.19,20 All above may contribute to the abnormal development of the pelvis on the affected side, because pelvic structure development depends in a large part on the biomechanics of normal hip.21,22
Albiñana et al7 studied a total of 83 patients with unilateral developmental hip dysplasia to evaluate the relationship between the pelvic shape and innominate bone in the initial anteroposterior radiographs. Statistically significant differences were observed in most cases, and pelvic asymmetry was obvious. In their opinion, changes of the pelvic shape occurred to patients with DDH, possibly due to growth disturbance of the triradiate cartilage. However, they did not follow the subjects to their adulthood for the further study on pelvic asymmetry. We believe that the pelvic asymmetry of DDH in adults is caused by the development of pelvic deformation during childhood.
Figure 3.
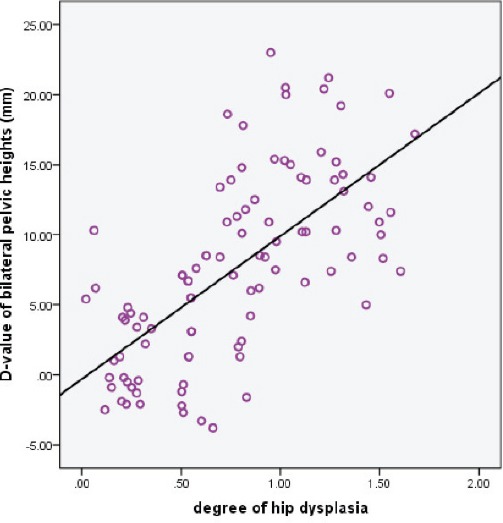
The correlation of the degree of hip dysplasia with D-value of bilateral pelvic heights (Y=10.2X-0.3, R=0.78, p=0.000).
Fujii et al1 reported that structural abnormalities were present throughout the entire pelvis in patients with DDH and that the morphological abnormalities of the acetabulum were not entirely caused by local dysplasia around the hip, but influenced by the morphologic features of the entire pelvis. However, their study focused only on acetabular version and coverage, rather than the entire pelvic morphology. We measured and compared bilateral pelvic and ischium heights in order to reflect the entire anatomy of the pelvic abnormalities.
The reviews of literatures have shown that THA is a common therapy for adult patients with hip developmental dysplasia with a high success rate. Equalization of low extremities lengths following THA is an important reconstructive criteria.12-14,23 However, the complex anatomy of femur and acetabulum makes the reconstruction standard technically challenging.11,17 Preoperative planning should include the causes of lower extremities length discrepancy and these should be taken into account during the procedures in order to equalize bilateral lower extremities length. So far, few literatures show that pelvis itself contributes to low extremities length discrepancy. For Crowe I and II, pelvic asymmetry has little effect on lower extremities length range, but for Crowe III and IV, the asymmetry should be paid enough attention to within the context of the causes of lower extremities length discrepancy.
Figure 4.
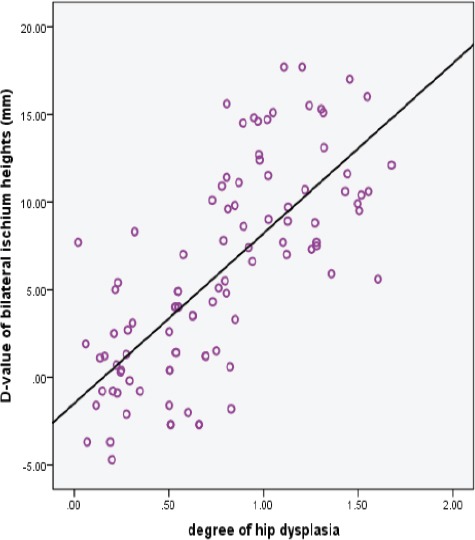
The correlation of the degree of hip dysplasia with D-value of bilateral ischium heights (Y=9.7X-1.5, R=0.72, p=0.000).
Among the majority of studies9-12,24 regarding to DDH, acetabular teardrops and ischial tuberosity have been used as fixed reference points in preoperative planning. Radiology methods using acetabular teardrops as reference points can accurately determine the hip joint’s center of hip rotation.24 Liu et al25 reported that when measuring lower extremities length discrepancy in THA, acetabular teardrops could be used as markers in the same way as the ischial notch because acetabular teardrops had separate anatomic structures. However, we found that the distances from teardrops to the line jointing bilateral ischial tuberosity among UDDH patients were not equal. In addition, inequalities had positive correlation with the degree of dysplasia. The mean difference value of bilateral ischium heights was 11.2 mm in Crowe IV patients. It might be misguided to take the teardrops and ischial tuberosity as marks to balance leg-length discrepancy. Although superior position of the false acetabulum is a main reason of leg length discrepancy, we find the anatomic abnormalities of teardrops, and ischial tuberosity may be a potential reason of leg length discrepancy for DDH patients. Therefore, we suggest that it should be taken more cautions to use teardrops and ischial tuberosity as anatomy landmarks to balance leg-length discrepancy for DDH patients in preoperative planning and THA.
In the present study, we found that the pelvic asymmetry is associated with unilateral developmental dysplasia of the hip in adult patients. In addition, the degree of pelvic asymmetry has correlation with the degree of hip dysplasia. The more the degrees of hip dysplasia are, the less the pelvic and ischium heights of the affected side are.
Study limitation
The limitation of this study was the relatively small sample size. In addition, our study was a retrospective; thus, clinical and radiological data were not readily available for all patients. While we observed the pelvic asymmetry in adult patients with unilateral developmental hip dysplasia, it was not clear how it affected lower extremities discrepancy and whether the teardrops were still appropriate as reference points for balancing lower extremities discrepancy. Further study are needed.
In conclusion, the pelvic asymmetry exists in adult patients with UDDH. The degree of asymmetry has correlation with the degree of hip dysplasia. Furthermore, we recommend that it should be taken more cautions to use teardrops and ischial tuberosity as anatomy landmarks to balance leg-length discrepancy for DDH patients in preoperative planning and THA.
Footnotes
References
- 1.Fujii M, Nakashima Y, Sato T, Akiyama M, Iwamoto Y. Pelvic deformity influences acetabular version and coverage in hip dysplasia. Clin Orthop Relat Res. 2011;469:1735–1742. doi: 10.1007/s11999-010-1746-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Liu S, Zuo J, Li Z, Yang Y, Liu T, Xiao J, et al. Study of three-dimensional morphology of the proximal femur in developmental adult dysplasia of the hip suggests that the on-shelf modular prosthesis may not be an ideal choice for patients with Crowe type IV hips. Int Orthop. 2016;14 doi: 10.1007/s00264-016-3248-6. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 3.Nakahara I, Takao M, Sakai T, Miki H, Nishii T, Sugano N. Three-dimensional morphology and bony range of movement in hip joints in patients with hip dysplasia. Bone Joint J. 2014;96:580–589. doi: 10.1302/0301-620X.96B5.32503. [DOI] [PubMed] [Google Scholar]
- 4.Jia J, Li L, Zhang L, Zhao Q, Wang E, Li Q. Can excessive lateral rotation of the ischium result in increased acetabular anteversion? A 3D-CT quantitative analysis of acetabular anteversion in children with unilateral developmental dysplasia of the hip. J Pediatr Orthop. 2011;31:864–869. doi: 10.1097/BPO.0b013e31823832ce. [DOI] [PubMed] [Google Scholar]
- 5.Mao C, Liang Y, Ding C, Guo L, Wang Y, Zeng Q, et al. The consistency between measurements of the femoral neck anteversion angle in DDH on three-dimensional CT and MRI. Acta Radiol. 2016;57:716–720. doi: 10.1177/0284185115603244. [DOI] [PubMed] [Google Scholar]
- 6.Jia J, Zhang L, Zhao Q, Li L, Liu X. Does medial rotational deformity of the whole pelvis universally exist in unilateral DDH? Arch Orthop Trauma Surg. 2011;131:1383–1388. doi: 10.1007/s00402-011-1326-1. [DOI] [PubMed] [Google Scholar]
- 7.Albiñana J, Morcuende JA, Delgado E, Weinstein SL. Radiologic Pelvic Asymmetry in Unilateral Late-Diagnosed Developmental Dysplasia of the Hip. J Pediatr Orthop. 1995;15:753–762. doi: 10.1097/01241398-199511000-00007. [DOI] [PubMed] [Google Scholar]
- 8.Yoon PW, Kim JI, Kim DO, Yu CH, Yoo JJ, Kim HJ, et al. Cementless total hip arthroplasty for patients with Crowe type III or IV developmental dysplasia of the hip: two-stage total hip arthroplasty following skeletal traction after soft tissue release for irreducible hips. Clin Orthop Surg. 2013;5:167–173. doi: 10.4055/cios.2013.5.3.167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Li L, Yu M, Yang C, Gu G. Total hip arthroplasty (S-ROM stem) and subtrochanteric osteotomy for Crowe type IV developmental dysplasia of the hip. Indian J Orthop. 2016;50:195–200. doi: 10.4103/0019-5413.177575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sakellariou VI, Christodoulou M, Sasalos G, Babis GC. Reconstruction of the Acetabulum in Developmental Dysplasia of the Hip in total hip replacement. Arch Bone Jt Surg. 2014;2:130–136. [PMC free article] [PubMed] [Google Scholar]
- 11.Yildirim T, Guclu B, Karaguven D, Kaya A, Akan B, Cetin I. Cementless total hip arthroplasty in developmental dysplasia of the hip with end stage osteoarthritis 2-7 years’ clinical results. Hip Int. 2015;25:442–446. doi: 10.5301/hipint.5000240. [DOI] [PubMed] [Google Scholar]
- 12.Murayama T, Ohnishi H, Mori T, Okazaki Y, Sujita K, Sakai A. A novel non-invasive mechanical technique of cup and stem placement and leg length adjustment in total hip arthroplasty for dysplastic hips. Int Orthop. 2015;39:1057–1064. doi: 10.1007/s00264-014-2613-6. [DOI] [PubMed] [Google Scholar]
- 13.Zhang Y, Chang F, Wang C, Yang M, Wang J. Pelvic reference selection in patients with unilateral Crowe type IV DDH for measuring leg length inequality. Hip Int. 2015;25:457–460. doi: 10.5301/hipint.5000235. [DOI] [PubMed] [Google Scholar]
- 14.Liu R, Li Y, Bai C, Song Q, Wang K. Effect of preoperative limb length discrepancy on abductor strength after total hip arthroplasty in patients with developmental dysplasia of the hip. Arch Orthop Trauma Surg. 2014;134:113–119. doi: 10.1007/s00402-013-1899-y. [DOI] [PubMed] [Google Scholar]
- 15.Crowe JF, Mani VJ, Ranawat CS. Total hip replacement in congenital dislocation and dysplasia of the hip. J Bone Joint Surg Am. 1979;61:15–23. [PubMed] [Google Scholar]
- 16.Tannast M, Pfannebecker P, Schwab JM, Albers CE, Siebenrock KA, Büchler L. Pelvic morphology differs in rotation and obliquity between developmental dysplasia of the hip and retroversion. Clin Orthop Relat Res. 2012;470:3297–3305. doi: 10.1007/s11999-012-2473-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Jia J, Zhang L, Zhao Q, Li L, Liu X. Does medial rotational deformity of the whole pelvis universally exist in unilateral DDH? Arch Orthop Trauma Surg. 2011;131:1383–1388. doi: 10.1007/s00402-011-1326-1. [DOI] [PubMed] [Google Scholar]
- 18.Jia J, Li L, Zhang L, Zhao Q, Wang E, Li Q. Can Excessive Lateral Rotation of the Ischium Result in Increased Acetabular Anteversion? A 3D-CT Quantitative Analysis of Acetabular Anteversion in Children With Unilateral Developmental Dysplasia of the Hip. J Pediatr Orthop. 2011;31:864–869. doi: 10.1097/BPO.0b013e31823832ce. [DOI] [PubMed] [Google Scholar]
- 19.Bilgen OF, Salar N, Bilgen MS, Mutlu M, Kara GK, Gürsel E. The Effect of Dislocation Type (Crowe Types I–IV) on Pelvic Development in Developmental Dysplasia of the Hip: A Radiologic Study of Anatomy. J Arthroplasty. 2015;30:875–878. doi: 10.1016/j.arth.2014.11.032. [DOI] [PubMed] [Google Scholar]
- 20.Rosenberg MR, Walton R, Rae EA, Bailey S, Nicol RO. Intra-articular dysplasia of the femoral head in developmental dysplasia of the hip. J Pediatr Orthop B. 2016 doi: 10.1097/BPB.0000000000000356. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 21.Liu RY, Wen XD, Tong ZQ, Wang KZ, Wang CS. Changes of gluteus medius muscle in the adult patients with unilateral developmental dysplasia of the hip. BMC Musculoskelet Disord. 2012;13:101–108. doi: 10.1186/1471-2474-13-101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Tannast M, Pfannebecker P, Schwab JM, Albers CE, Siebenrock KA, Büchler L. Pelvic morphology differs in rotation and obliquity between developmental dysplasia of the hip and retroversion. Clin Orthop Relat Res. 2012;470:3297–3305. doi: 10.1007/s11999-012-2473-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Manzotti A, Cerveri P, Momi ED, Pullen C, Confalonieri N. Does computer-assisted surgery benefit leg length restoration in total hip replacement? Navigation versus conventional Freehand. Int Orthop. 2011;35:19–24. doi: 10.1007/s00264-009-0903-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Li X, Guan G, Li J. Reconstruction of hip center in total hip arthroplasty for developmental dysplasia of hip [Article in Chinese] Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2012;26:1037–1040. [PubMed] [Google Scholar]
- 25.Liu R, Li Y, Fan L, Mu M, Wang K, Song W. Depression and anxiety before and after limb length discrepancy correction in patients with unilateral developmental dysplasia of the hip. J Psychosom Res. 2015;79:574–579. doi: 10.1016/j.jpsychores.2015.08.002. [DOI] [PubMed] [Google Scholar]