

Abstract
Objectives
To analyze and evaluate the safety and cost-effectiveness of a gradually-implemented antimicrobial stewardship programs (ASP) in a tertiary care center.
Methods
Prospective data were collected from an ASP that was gradually introduced between April 2012 and December 2013 in 6 hospital departments, over successive periods of 3 months each. A multidisciplinary team supervised antibiotic use and regulated pharmacy dispensations of a list of restricted antimicrobials (RAs). Indicators were prospectively monitored and included hospital mortality as the safety indicator; incidence of multi-drug resistance (MDR) infections as the effectiveness indicator, RA cost savings as the cost-effectiveness indicator and RA consumption indicated the process implementation.
Results
Between 2012 and 2014, dispensations of RAs decreased by 67% and prescriptions by 75%; no increase in mortality rate was observed. Microbiologically, there was a decreasing trend of incidence across all monitored infections, but this was only significant for Acinetobacter baumannii (p=0.007). Cost analysis showed a decrease in expenditure for RAs, with an average monthly saving of up to 326,020USD.
Conclusions
Stepwise implementation of ASPs is a safe and cost-effective strategy for improving antibiotic prescribing practice and to reduce multi-drug resistance.
Misprescription and misuse of antibiotics are major factors underlying the development of multi-drug resistance (MDR), which constitutes a public health issue of growing importance.1,2 The global mortality attributable to antimicrobial resistance is estimated to reach 10 million annual deaths by 2050, making it one of the leading causes of death with an economic impact of up to 100 trillion US dollars (USD).3 Recent reports from the Middle-East, including Saudi Arabia, show a considerable and increasing prevalence of resistant and MDR infectious agents such as Acinetobacter baumannii,4-6 methicillin-resistant Staphylococcus aureus (MRSA),7-10 MDR Salmonella enterica serovar typhi,11 extended spectrum b-lactamase (ESBL)-producing Klebsiella pneumonia,12 ESBL-producing Escherichia coli13 and Pseudomonas aeruginosa.14 In the USA, approximately 2,000,000 MDR infections are diagnosed each year and are responsible for 23,000 deaths per year.15 Data from the European Antimicrobial Resistance Surveillance System (EARSS) showed that MRSA was present in up to 60% of isolates in some European countries in 2014.16 The worldwide rise in antimicrobial resistance is correlated to the increase in antibiotic consumption, estimated at 40% in the last decade with some regional discrepancies.3 The highest rates of antimicrobial resistance are usually recorded in the countries with the high consumption of antibiotics.17 Since several common pathogens have become resistant to conventional antibiotics, there is an increasing empirical routine use of broad-spectrum (BS) combinations, which jeopardize their future efficacy.18 It has been found that even with optimal use, BS antimicrobial therapy is associated with detrimental effects on the patient, such as the disturbance of gut microbiota resulting in abnormal distribution of infective and life-threatening microorganisms.19-21 The other alarming aspect of the problem is the failure of the pharmaceutical industry to develop new molecules, with no more than 2 new antimicrobial classes launched in the 4 last decades.18,22 As a consequence, there is an urgent need to raise awareness among physicians and patients worldwide to improve antibiotic prescribing and use; otherwise, the current trends predict a pessimistic future.23
At the hospital level, antimicrobial stewardship programs (ASPs) are among the most cost-effective strategies to improve antimicrobial use and prescribing without negatively affecting patient outcomes. Such programs provide a comprehensive picture of antimicrobial consumption within a given health care facility, allow evidence-based prescribing recommendations, and can provide timely feedback on the efficacy of the actions implemented. From an economic point of view, ASPs can lead to substantial cost savings.24 The objective of this article is to analyze the safety and cost-effectiveness of a gradually-implemented ASP in a tertiary care center.
Methods
Presentation of the antibiotic stewardship program
The program was launched in 2011 at the King Abdulaziz University Hospital (KAUH), Jeddah, Saudi Arabia, and a stepwise implementation was adopted. King Abdulaziz University Hospital is a tertiary care center with a total capacity of 1002 beds, among which 157 are dedicated for critical care units. It includes 12 medical departments with a broad-range of specialties; along with 7 supporting departments such as laboratories, pharmacy, anesthesia, and blood bank.
Situational analysis
As a precursor to ASP implementation, we conducted a retrospective review of antibiotic consumption, prescription patterns, and MDR data for 2011. Analyses of these preliminary data provided 3 major findings: 1) antibiotics were a substantial annual expense, 2) there was a lack of clear guidelines for perioperative antimicrobial prophylaxis, and 3) there was a high incidence of MDR.
Formation of the antimicrobial approval team
In the light of these findings, a multidisciplinary team was formed comprising an infection control consultant, 2 clinical pharmacists and one medical-surgical critical physician. The team, designated as the antimicrobial approval team (AAT), was assigned the role of gradually setting up the ASPs in the hospital units. The main roles of the AAT were to: 1) supervise antibiotic use by verifying the appropriateness of all prescriptions, using microbiological and clinical data, 2) restrict the use of certain antibiotics (Table 1), and 3) ensure compliance with the peri-operative antimicrobial prophylaxis guidelines by interested departments.
Table 1.
Restricted antimicrobials of Group A, which are the restricted antimicrobials not commonly prescribed on an emergency basis and Group B which are the restricted antimicrobials that are classed as life-saving medicines and are likely to be prescribed on an emergency basis.
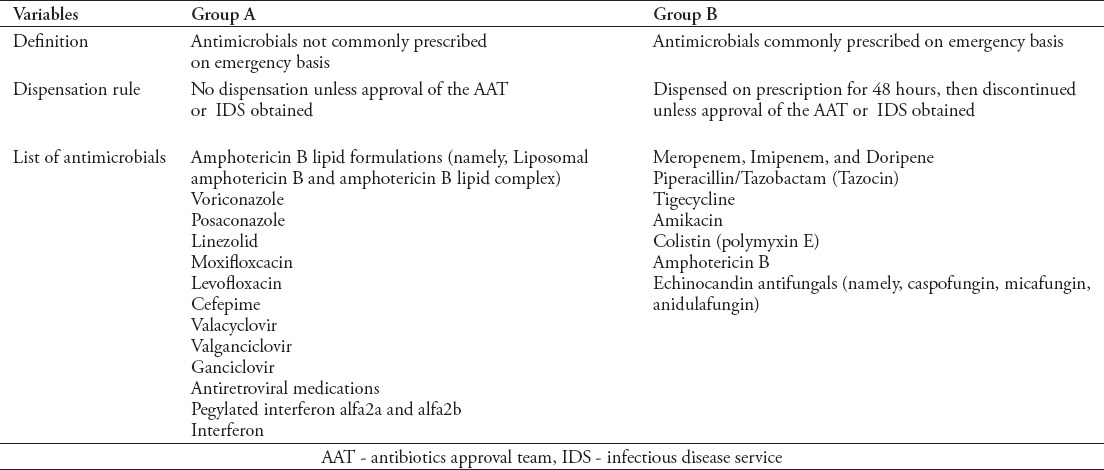
Restricted antimicrobials
The list of restricted antimicrobials (Table 1) included 2 groups: Group A: restricted antimicrobials not commonly prescribed on an emergency basis. Group B: restricted antimicrobials that are classed as life-saving medicines and are likely to be prescribed on an emergency basis. Antibiotics not in these 2 categories were dispensed without restriction, by simple prescription by a physician.
Approval, procedure, and dispensation rule
For any prescription of a restricted antimicrobial, prescribers must complete the prescription notification; a form designed for the purpose of the ASP. The notification was communicated to the AAT and infectious diseases (IDS) teams, either via a pager number dedicated for the approval process, or through electronic referral. The AAT assesses the prescription and rapid feedback is given to the prescriber. Antimicrobials from group A: if the ATT approves the prescription, the pharmacy is instructed to either dispense or not dispense the antimicrobial. If the latter, an alternative class is suggested to the prescriber, if needed, with reference to the patient’s clinical data. Antimicrobials from group B: the pharmacy dispenses the antimicrobial, on prescription, for only 48 hours pending ATT, or IDS assessment. If the ATT approves the prescription, the order is given to the pharmacy to continue dispensation. Otherwise, the order is given to discontinue the dispensation and the prescriber is recommended to switch to a more appropriate class, if clinically indicated. In case of conflict, physicians are encouraged to discuss the patient’s case with the AAT or the IDS. In any case, they are recommended to consult the IDS as soon as the treatment is prescribed, in order to avoid automatic interruption (Figure 1).
Figure 1.
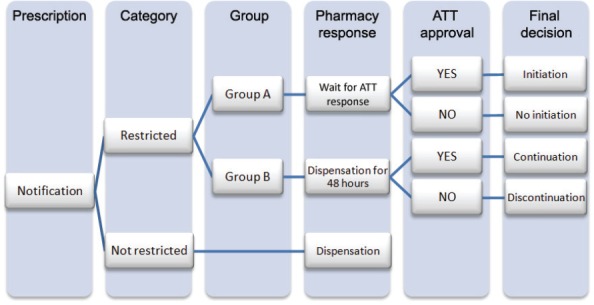
Decision tree for antimicrobial dispensation according to the antimicrobial stewardship program. AAT - antibiotics approval team.
Stepwise implementation of the antimicrobial stewardship program
The ASP was piloted in the surgical department (male and female units) for a 6-month period starting April 2012. In view of a successful implementation, indicated by a rapid and significant reduction in antimicrobial consumption, the ASP was expanded to incorporate the Obstetrics and Gynecology Department October 2012. Between October 2012 and December 2013, the ASP expanded again to include the Medical Department (male and female unit), the Critical Care Unit (CCU), the Medical Intensive Care Unit (MICU), and the Surgical Intensive Care Unit (SICU). The gradual recruitment of the different departments enabled a relationship of trust to be established between the AAT and the newly included teams, where systemic audits on protocol compliance could be carried out, allowing constructive exchange with the physicians.
Evaluation of the antimicrobial stewardship program
The data collected from the units during the study period included BS antibiotic prescriptions, indications, ATT decisions (dispensation, switch or discontinuation), patient mortality, and microbiological results (including isolations of MDR bacteria). The implementation of the ASP was assessed by the number of prescriptions and dispensations. Results were calculated as annual averages. The effective implementation of the program was indicated by a significant reduction in dispensation/consumption, and secondarily in the number of prescriptions. Hospital mortality rate was used as an indicator of the safety of the program. We hypothesized that an increase in hospital mortality could indicate that the ASP may be too restrictive, risking under-treatment of patients. In contrast, no increase in hospital mortality would indicate the safety of the program. The principal indicator of ASP effectiveness was the incidence of MDR. A decrease in MDR incidence would indicate a more appropriate use of antibiotics and better compliance to protocols. Microbiology data were collected to analyze the monthly incidence of MRSA, Vancomycin-resistant enterococci (VRE), Pseudomonas aeruginosa, Acinetobacter baumannii (ABB), and ESBL-producing organisms. Cost saving was calculated for each year by subtracting the cost of restricted antibiotics dispensed from the cost of all prescribed restricted antibiotics. This was expressed as a monthly mean.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences version 16.0 for Windows (SPSS Inc., Chicago, IL, USA). Means and standard deviations (SD) were calculated for continuous variables and frequencies/percentages for categorical variables. Correlations between categorical variables were analyzed using Chi-square tests. Means were analyzed using either independent t-tests or one-way analysis of variance as appropriate, and post hoc analysis was carried out using Tukey’s HSD test for multiple comparisons of means. A p-value <0.05 was considered significant.
Results
A remarkable (67.2%) decrease was observed in dispensations of restricted antibiotics, from 17,763 dispensed units per month in 2012 to 5,819 in 2014. This was in parallel with a nearly 5-fold decrease in prescription of restricted antibiotics (from 52,144 to 11,867 units ordered per month) over the same period (Figure 2).
Figure 2.
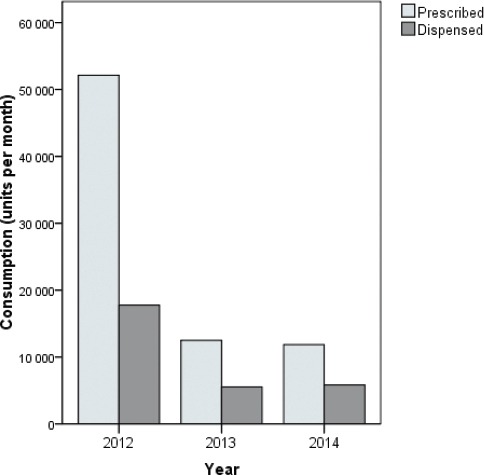
Hospital consumption of broad-spectrum antimicrobials as a progress indicator of the antimicrobial stewardship program.
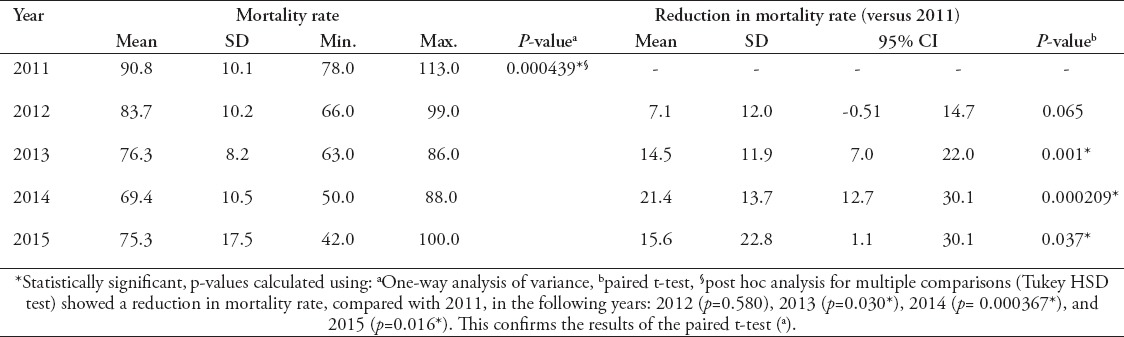
The mean mortality rate decreased from 90.83 (±10.12) deaths per 10,000 patient months in 2011 to 75.25 (±17.46) in 2015. The lowest rate of 69.42 (±10.51), observed in 2014, was found to be significantly lower than in the other years (p<0.001). Further analysis showed a significant decrease in mortality rate of up to 21.42 (±13.68; 95% CI=12.72-30.11], p<0.001) per 10,000 patients months (Table 2).
Table 2.
Evolution over time of mortality rate expressed per 10,000 patient months by year.
Analysis of microbiological data showed a decreasing trend in all monitored MDR infections from 2012 to 2015. However, this was only statistically significant in ABB infections, from 5.20 (± 3.18) isolates per 10,000 patient days in 2012 to 1.95 (± 1.28) in 2015 (p=0.007) (Figure 3). Cost analysis showed a considerable decrease in hospital expenditure on restricted antibiotics between 2012 and 2014. Unfortunately, data from 2011 could not be retrospectively collected to carry out comparative analysis. The average monthly saving was highest in 2012 at SAR1,222,613 ($326,020); while savings in 2013 at SAR488,834 ($130,350), and in 2014 at SAR391,594 ($104,420). The evolution by department of the number of dispensed RAs over the 3 years was presented in Figure 4.
Figure 3.
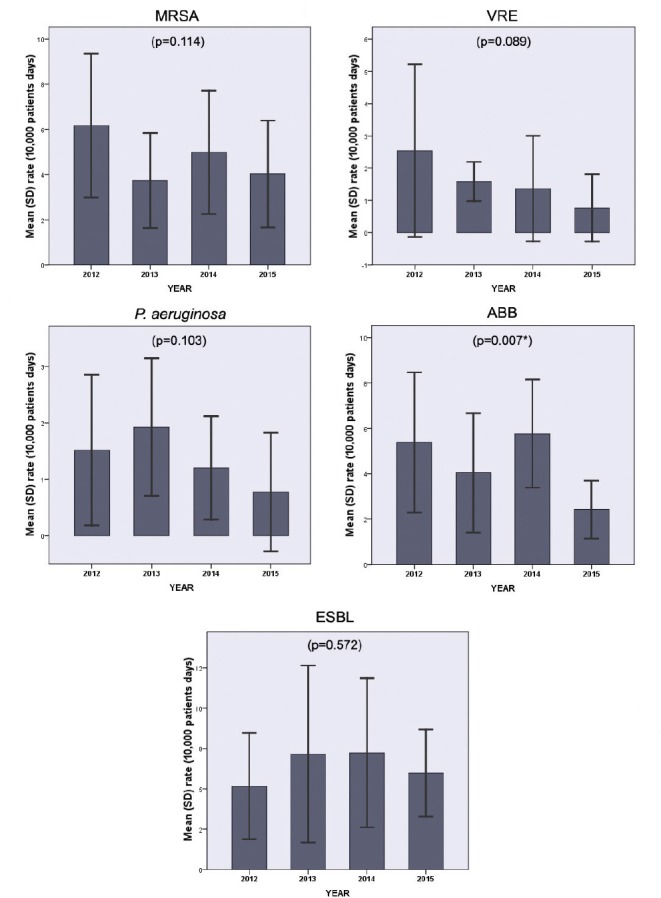
Evolution over time of multi drug resistance prevalence rate expressed per 10,000 patient days. MRSA - methicillin-resistant Staphylococcus aureus, VRE - vancomycin-resistant enterococci, P. aeruginosa - multidrug resitant Psedomonas aeruginosa, ABB - Acinetobacter baumannii, ESBL - extened-spectrum beta-lactamases-producing organisms, *statistically significant result. Statistical test used One-way analysis of variance and post hoc multiple comparisons analysis (Tukey Kramer test).
Figure 4.
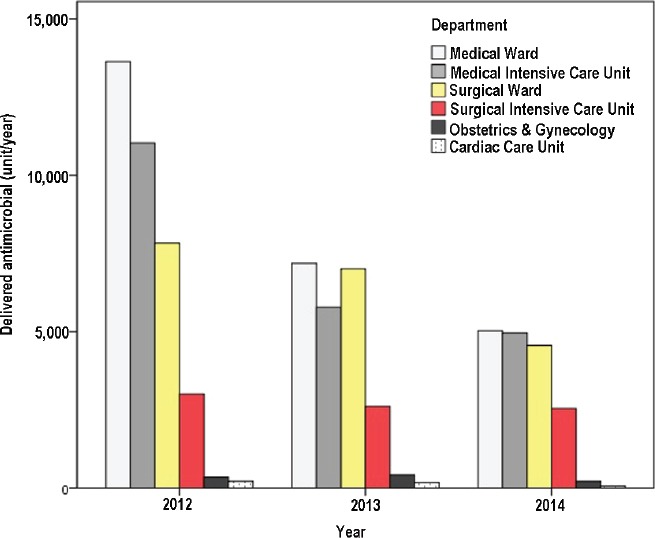
Hospital consumption of broad-spectrum antimicrobials per department as a progress indicator of the antimicrobial stewardship program.
Discussion
Our findings support the efficacy of a stepwise ASP in inducing safe, effective, and cost-effective change in antibiotic use in a hospital setting. Despite the gradual implementation, the ASP led to monthly cost-savings of up to $326,020 on restricted antibiotics, as an effect of the 67.2% decrease in consumption. The highest monthly saving occurred in 2012, indicating an important discrepancy between prescriptions and dispensations at the start of the program. In the following years, we observed smaller cost savings, indicating a subsequent reduction in the gap between prescriptions and dispensations. Other studies of ASPs have reported a decrease in antimicrobial consumption of up to 36% and annual savings of up to $0.9 million.24 Beyond their efficacy in reducing healthcare costs, ASPs are associated with better patient outcomes,25,26 including a reduction in both length of hospital stay and mortality.27 Although a concomitant decrease in patient mortality rate was observed, our data were not conclusive enough to establish a relationship between mortality and MDR, or to directly associate this decrease in mortality to the efficacy of the ASP. However, the absence of increase in mortality rate indicates, at least partially, the safety of this ASP regarding patient outcomes. Previous studies showed that there is a triangular relationship between MDR, inappropriate antibiotic use and mortality, especially in highly-exposed patient populations such as in an ICU or NICU, or in patients with bloodstream infections.28-32 Microbiologically, we noted a decrease in the prevalence of MDR, although this was not statistically significant. Infections that have been monitored throughout our program were the most frequently reported in Saudi Arabia and the Middle-East.4-10,12-14 Other studies report that the introduction of an ASP improved microbiologically-targeted therapy33 and decreased drug resistance in infectious agents including Clostridium difficile infections,34 and VRE.31
The decrease in consumption and the consequent cost-savings are directly attributed to the restrictive method, ensured by authorization-based dispensation at the prerogative of the ATT.24,35 Thus, the observed reduction in antimicrobial consumption does not necessarily reflect the improvement in physicians’ prescribing habits nor predict the upholding over time of these results. Indeed, one of the obstacles we faced was the physicians’ resistance to comply with the new guidelines, which required adoption of another core approach, in addition to the restrictive method. This approach consisted of systemic audits on protocol compliance in the participating departments, along with regular feedback to prescribers.22,24 This strategy aimed to prevent physicians’ resistance to changing their prescribing habits, by instigating a positive climate of exchange between them and the ATT and IDS. It was recommended that ASP prescribing guidelines should allow the physicians freedom to prescribe,18 promote clinical discussions, and offer an opportunity to provide infectious disease expertise for a specific patient.36
We observed a 75% decrease in the number of RAs prescribed, which could indicate a change in prescribing habits among physicians and their adherence to the ASP. However, this should be interpreted with caution because restrictive methods may simply induce a shift to prescribing other, non-restricted antimicrobial agents, which would give less successful long-term results.24 A meta-analysis showed that restrictive methods are generally more effective than persuasive ones in terms of both prescribing and microbial outcomes; however, no advantage was noticed in long-term outcomes.37 The role of physicians constitutes a double-edged sword in the long battle against MDR. Physicians may not understand the importance of restricting antibiotic use when this is contrary to the immediate interest of the patient. Adopting appropriate prescribing rules requires going beyond the patient-focused clinical approach, and being aware of the community issues related to antimicrobial overuse.38 The majority of doctors recognize that antimicrobials are overused; although only a few declare using them optimally.39 Data from Saudi Arabia showed that despite good levels of awareness among physicians regarding MDR and the existence of local and national antimicrobial prescribing guidelines, a great proportion of them stated that they do not always comply with these guidelines.40,41 Fear for patient’s prognosis, in addition to complacent prescribing, have been found to be the most significant risk factors of antibiotic misprescription.41-43 A communication from the National Institute for Health and Care Excellence (NICE) in the UK reported that 9 out of 10 general practitioners feel pressured to prescribe antibiotics and almost 100% of patients can get an antibiotic prescription on request.22 In short, correcting physicians’ attitudes and knowledge by means of targeted restrictive and persuasive interventions may be the crucial link for success.37,42,44 Beyond sharing a successful experience, publishing such results in a peer-reviewed journal is essential to raise awareness in the medical community, with the goal of inducing a change in the prescribing habits even in the most reluctant physicians. Moreover, the dissemination of ASP-related financial and microbiological outcomes can be used to argue in favor of a long-term community vision without undermining the outcome for an individual patient.38
Other important observations and lessons drawn from our experience are the tremendous time, staff mobilization, and daily efforts required to achieve the goals of the audit and feedback process. However, beyond the laborious aspect, execution of these tasks provided valuable learning opportunities for both physicians and antimicrobial approval team members, which enhanced persuasion and compliance to the program. It would be interesting to explore in further studies the sustainability of these results and the prospective need of implementing recall sessions of ASP in order to maintain the level of awareness among prescribers. In addition, fighting against MDR includes consideration of nosocomial infections and screening for potential carriers among care staff.7 Other factors of misprescribing, such as increased physician workload,43,45,46 insufficient guideline implementation44,47 or diagnostic challenges,42 should be investigated in each specific setting. When these are identified, relevant corrective measures should be included in the ASP for greater effectiveness.25 Moreover, assessing and monitoring physicians’ knowledge and attitude could be an excellent indicator of efficacy in ASPs with persuasive methods.47 To provide a more optimistic future, good clinical practice training programs must include and emphasize appropriate antibiotic prescribing, and factors related to bad prescribing habits should be detected and corrected at an early stage.48
Study limitations
Some departments such as pediatrics, emergency, and day care units were not included in the study, although involved in the ASP by the end 2014. Consequently, the presented efficacy of the ASP at the hospital level may be underestimated for the year 2014.
In conclusion, the step-approach implementation of the ASP is a safe, clinically- and cost-effective strategy for improving the practice of prescribing antibiotics, as a preventive measure against MDR. Our experience showed a considerable decrease in antibiotic consumption, prescriptions and cost, without any perceptible harm to patients over the 4 years of follow-up. To effectively fight against MDR, physicians are increasingly required to adopt a community-oriented clinical approach. Persuasive measures should be associated with ASP to ensure physician participation, by implementing targeted awareness-raising and educational actions. Bad prescribing habits should be detected and corrected at an early stage in medical training.
Acknowledgment
Authors would like to acknowledge Dr. Ayaz Khan and Dr. Shehata A. Abdelghany for their hard work with antibiotics review and approval. Special thanks are dedicated to Prof. Tarik Madani for his valuable guidance, expertise, and generosity throughout the implementation of the antimicrobial stewardship program. We also want to thank the administration of King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia who made possible the successful implementation of this antimicrobial stewardship program.
Footnotes
References
- 1.Roque F, Herdeiro MT, Soares S, Teixeira Rodrigues A, Breitenfeld L, Figueiras A. Educational interventions to improve prescription and dispensing of antibiotics: a systematic review. BMC Public Health. 2014;14:1276. doi: 10.1186/1471-2458-14-1276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Oldfield E, Feng X. Resistance-resistant antibiotics. Trends Pharmacol Sci [Internet] 2014;35:664–674. doi: 10.1016/j.tips.2014.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Antimicrobial Review on Resistance. Antimicrobial resistance: Tackling a crisis for the health and wealth of nations [Internet] London (UK): Wellcome Trust; 2014. [Google Scholar]
- 4.Lakshmana Gowda K, Marie MAM, Al-Sheikh YA, John J, Gopalkrishnan S, Chikkabidare Shashidhar P, et al. A 6-year surveillance of antimicrobial resistance patterns of Acinetobacter baumannii bacteremia isolates from a tertiary care hospital in Saudi Arabia during 2005-2010. Libyan J Med [Internet] 2014;9:24039. doi: 10.3402/ljm.v9.24039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Abdalhamid B, Hassan H, Itbaileh A, Shorman M. Characterization of carbapenem-resistant Acinetobacter baumannii clinical isolates in a tertiary care hospital in Saudi Arabia. New Microbiol [Internet] 2014;37:65–73. [PubMed] [Google Scholar]
- 6.Elabd FM, Al-Ayed MSZ, Asaad AM, Alsareii SA, Qureshi MA, Musa HAA. Molecular characterization of oxacillinases among carbapenem-resistant Acinetobacter baumannii nosocomial isolates in a Saudi hospital. J Infect Public Health. 2015;(3):242–247. doi: 10.1016/j.jiph.2014.10.002. [DOI] [PubMed] [Google Scholar]
- 7.Al-Humaidan OS, El-Kersh TA, Al-Akeel RA. Risk factors of nasal carriage of Staphylococcus aureus and methicillin-resistant Staphylococcus aureus among health care staff in a teaching hospital in central Saudi Arabia. Saudi Med J. 2015;36:1084–1090. doi: 10.15537/smj.2015.9.12460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Harastani HH, Tokajian ST. Community-associated methicillin-resistant Staphylococcus aureus clonal complex 80 type IV (CC80-MRSA-IV) isolated from the Middle East: a heterogeneous expanding clonal lineage. PLoS One. 2014;9:e103715. doi: 10.1371/journal.pone.0103715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Monecke S, Skakni L, Hasan R, Ruppelt A, Ghazal SS, Hakawi A, et al. Characterisation of MRSA strains isolated from patients in a hospital in Riyadh, Kingdom of Saudi Arabia. BMC Microbiol. 2012;23:146. doi: 10.1186/1471-2180-12-146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tokajian S. New epidemiology of Staphylococcus aureus infections in the Middle East. Clinical Microbiology and Infection. 2014;20:624–628. doi: 10.1111/1469-0691.12691. [DOI] [PubMed] [Google Scholar]
- 11.Rahman BA, Wasfy MO, Maksoud MA, Hanna N, Dueger E, House B. Multi-drug resistance and reduced susceptibility to ciprofloxacin among Salmonella enterica serovar Typhi isolates from the Middle East and Central Asia. New Microbes New Infect. 2014;2:88–92. doi: 10.1002/nmi2.46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Vali L, Dashti AA, Jadaon MM, El-Shazly S. The emergence of plasmid mediated quinolone resistance qnrA2 in extended spectrum b-lactamase producing Klebsiella pneumoniae in the Middle East. Daru. 2015;23:34. doi: 10.1186/s40199-015-0116-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bertrand X, Dowzicky MJ. Antimicrobial susceptibility among gram-negative isolates collected from intensive care units in North America, Europe, the Asia-Pacific Rim, Latin America, the Middle East, and Africa between 2004 and 2009 as part of the tigecycline evaluation and survey. Clin Ther. 2012;34:124–137. doi: 10.1016/j.clinthera.2011.11.023. [DOI] [PubMed] [Google Scholar]
- 14.Said KB, Al-Jarbou AN, Alrouji M, Al-Harbi HO. Surveillance of antimicrobial resistance among clinical isolates recovered from a tertiary care hospital in Al Qassim, Saudi Arabia. Int J Health Sci (Qassim) 2014;8:3–12. doi: 10.12816/0006066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Center for Disease Control and Prevention. Antibiotic Resistance Threats in the United States. 2013. [[cited 2016 Feb 8]]. Available from: http://www.cdc.gov/drugresistance/threat-report-2013/index.html .
- 16.European Centre for Disease Prevention and Control. Antimicrobial resistance surveillance in Europe. 2014. [[cited 2016 Feb 8]]. Available from: http://ecdc.europa.eu/en/healthtopics/antimicrobial_resistance/database/Pages/graph_reports.aspx .
- 17.van de Sande-Bruinsma N, Grundmann H, Verloo D, Tiemersma E, Monen J, Goossens H, et al. Antimicrobial drug use and resistance in Europe. Emerg Infect Dis. 2008;14:1722–1730. doi: 10.3201/eid1411.070467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Livermore DM. Minimising antibiotic resistance. Lancet Infect Dis. 2005;5:450–459. doi: 10.1016/S1473-3099(05)70166-3. [DOI] [PubMed] [Google Scholar]
- 19.Dubourg G, Lagier JC, Armougom F, Robert C, Audoly G, Papazian L, et al. High-level colonisation of the human gut by Verrucomicrobia following broad-spectrum antibiotic treatment. Int J Antimicrob Agents. 2013;41:149–155. doi: 10.1016/j.ijantimicag.2012.10.012. [DOI] [PubMed] [Google Scholar]
- 20.Panda S, El Khader I, Casellas F, López Vivancos J, García Cors M, Santiago A, et al. Short-term effect of antibiotics on human gut microbiota. PLoS One. 2014;9:e95476. doi: 10.1371/journal.pone.0095476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mason KL, Erb Downward JR, Mason KD, Falkowski NR, Eaton KA, Kao JY, et al. Candida albicans and bacterial microbiota interactions in the cecum during recolonization following broad-spectrum antibiotic therapy. Infect Immun. 2012;80:3371–3380. doi: 10.1128/IAI.00449-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.NICE antimicrobial stewardship: right drug, dose, and time? Lancet. 2015;386:717. doi: 10.1016/S0140-6736(15)61522-7. [DOI] [PubMed] [Google Scholar]
- 23.Spellberg B, Gilbert DN. The future of antibiotics and resistance: a tribute to a career of leadership by John Bartlett. Clin Infect Dis. 2014;59(Suppl 2):S71–S75. doi: 10.1093/cid/ciu392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dellit TH, Owens RC, McGowan JE, Jr, Gerding DN, Weinstein RA, Burke JP, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44:159–177. doi: 10.1086/510393. [DOI] [PubMed] [Google Scholar]
- 25.Aryee A, Price N. Antimicrobial stewardship - can we afford to do without it? Br J Clin Pharmacol. 2015;79:173–181. doi: 10.1111/bcp.12417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mendelson M. Role of antibiotic stewardship in extending the age of modern medicine. S Afr Med J. 2015;105:414–418. doi: 10.7196/samj.9635. [DOI] [PubMed] [Google Scholar]
- 27.Perez KK, Olsen RJ, Musick WL, Cernoch PL, Davis JR, Peterson LE, et al. Integrating rapid diagnostics and antimicrobial stewardship improves outcomes in patients with antibiotic-resistant Gram-negative bacteremia. J Infect. 2014;69:216–225. doi: 10.1016/j.jinf.2014.05.005. [DOI] [PubMed] [Google Scholar]
- 28.Viale P, Giannella M, Lewis R, Trecarichi EM, Petrosillo N, Tumbarello M. Predictors of mortality in multidrug-resistant Klebsiella pneumoniae bloodstream infections. Expert Rev Anti Infect Ther. 2013;11:1053–1063. doi: 10.1586/14787210.2013.836057. [DOI] [PubMed] [Google Scholar]
- 29.Zilberberg MD, Shorr AF, Micek ST, Vazquez-Guillamet C, Kollef MH. Multi-drug resistance, inappropriate initial antibiotic therapy and mortality in Gram-negative severe sepsis and septic shock: a retrospective cohort study. Crit Care. 2014;18:596. doi: 10.1186/s13054-014-0596-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Shorr AF, Zilberberg MD, Micek ST, Kollef MH. Predictors of hospital mortality among septic ICU patients with Acinetobacter spp. bacteremia: a cohort study. BMC Infect Dis. 2014;14:572. doi: 10.1186/s12879-014-0572-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Patel SJ, Saiman L. Antibiotic resistance in neonatal intensive care unit pathogens: mechanisms, clinical impact, and prevention including antibiotic stewardship. Clin Perinatol. 2010;37:547–563. doi: 10.1016/j.clp.2010.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Shorman M, Al-Tawfiq JA. Risk factors associated with vancomycin-resistant enterococcus in intensive care unit settings in Saudi Arabia. Interdiscip Perspect Infect Dis. 2013;2013:369674. doi: 10.1155/2013/369674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Katsios CM, Burry L, Nelson S, Jivraj T, Lapinsky SE, Wax RS, et al. An antimicrobial stewardship program improves antimicrobial treatment by culture site and the quality of antimicrobial prescribing in critically ill patients. Crit Care. 2012;16:R216. doi: 10.1186/cc11854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Wenisch JM, Equiluz-Bruck S, Fudel M, Reiter I, Schmid A, Singer E, et al. Decreasing Clostridium difficile infections by an antimicrobial stewardship program that reduces moxifloxacin use. Antimicrob Agents Chemother. 2014;58:5079–5083. doi: 10.1128/AAC.03006-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Schwartzberg E, Rubinovich S, Hassin D, Haspel J, Ben-Moshe A, Oren M, et al. Developing and implementing a model for changing physicians’ prescribing habits--the role of clinical pharmacy in leading the change. J Clin Pharm Ther. 2006;31:179–185. doi: 10.1111/j.1365-2710.2006.00724.x. [DOI] [PubMed] [Google Scholar]
- 36.Jump RLP, Olds DM, Seifi N, Kypriotakis G, Jury LA, Peron EP, et al. Effective antimicrobial stewardship in a long-term care facility through an infectious disease consultation service: keeping a LID on antibiotic use. Infect Control Hosp Epidemiol. 2012;33:1185–1192. doi: 10.1086/668429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Davey P, Brown E, Charani E, Fenelon L, Gould IM, Holmes A, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev. 2013;(4):CD003543. doi: 10.1002/14651858.CD003543.pub3. [DOI] [PubMed] [Google Scholar]
- 38.Mack A, Relman DA, Choffnes ER. Antibiotic resistance: implications for global health and novel intervention strategies: workshop summary. Washington (DC): National Academies; 2010. [PubMed] [Google Scholar]
- 39.Srinivasan A, Song X, Richards A, Sinkowitz-Cochran R, Cardo D, Rand C. A survey of knowledge, attitudes, and beliefs of house staff physicians from various specialties concerning antimicrobial use and resistance. Arch Intern Med. 2004;164:1451–1456. doi: 10.1001/archinte.164.13.1451. [DOI] [PubMed] [Google Scholar]
- 40.Baadani AM, Baig K, Alfahad WA, Aldalbahi S, Omrani AS. Physicians’ knowledge, perceptions, and attitudes toward antimicrobial prescribing in Riyadh, Saudi Arabia. Saudi Med J. 2015;36:613–619. doi: 10.15537/smj.2015.5.11726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Al-Harthi SE, Khan LM, Osman A-MM, Alim MA, Saadah OI, Almohammadi AA, et al. Perceptions and knowledge regarding antimicrobial stewardship among clinicians in Jeddah, Saudi Arabia. Saudi Med J. 2015;36:813–820. doi: 10.15537/smj.2015.7.11833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Gonzalez-Gonzalez C, López-Vázquez P, Vázquez-Lago JM, Piñeiro-Lamas M, Herdeiro MT, Arzamendi PC, et al. Effect of Physicians’ Attitudes and Knowledge on the Quality of Antibiotic Prescription: A Cohort Study. PLoS One. 2015;10:e0141820. doi: 10.1371/journal.pone.0141820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Lopez-Vazquez P, Vazquez-Lago JM, Figueiras A. Misprescription of antibiotics in primary care: a critical systematic review of its determinants. J Eval Clin Pract. 2012;18:473–484. doi: 10.1111/j.1365-2753.2010.01610.x. [DOI] [PubMed] [Google Scholar]
- 44.Pinder R, Sallis A, Berry D, Chadborn T. Behaviour change and antibiotic prescribing in healthcare settings. Literature review and behavioural analysis. Wellington House (UK): Public Health England; 2015. [Google Scholar]
- 45.Teixeira Rodrigues A, Ferreira M, Piñeiro-Lamas M, Falcão A, Figueiras A, Herdeiro MT. Determinants of physician antibiotic prescribing behaviour: a 3-year cohort study in Portugal. Curr Med Res Opin. 2016;32:949–957. doi: 10.1185/03007995.2016.1154520. [DOI] [PubMed] [Google Scholar]
- 46.Luyt CE, Bréchot N, Trouillet JL, Chastre J. Antibiotic stewardship in the intensive care unit. Crit Care. 2014;18:480. doi: 10.1186/s13054-014-0480-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Rodrigues AT, Ferreira M, Roque F, Falcão A, Ramalheira E, Figueiras A, et al. Physicians’ attitudes and knowledge concerning antibiotic prescription and resistance: questionnaire development and reliability. BMC Infect Dis. 2016;16:7. doi: 10.1186/s12879-015-1332-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Dallas A, van Driel M, van de Mortel T, Magin P. Antibiotic prescribing for the future: exploring the attitudes of trainees in general practice. Br J Gen Pract. 2014;64:e561–e567. doi: 10.3399/bjgp14X681373. [DOI] [PMC free article] [PubMed] [Google Scholar]