

Abstract
Objectives
To document the knowledge of, attitudes toward, and practices of adverse drug reaction (ADR) reporting and pharmacovigilance systems among healthcare professionals.
Methods
This descriptive cross-sectional study was conducted using a questionnaire. This study took place at King Fahd Hospital of the University (KFHU), Khobar, Kingdom of Saudi Arabia, between April 2015 and April 2016. Healthcare professionals, including physicians, pharmacists, pharmacy technicians, and nurses, were considered eligible and invited to take part in the study. A link to the online questionnaire was sent to each participant via E-mail, and a hard copy was circulated at the hospital after the objectives of the study were explained. The questionnaire comprised items regarding knowledge/awareness of pharmacovigilance and ADRs, perception/attitude towards pharmacovigilance and ADR reporting, and practices of ADR reporting. Descriptive statistics were used to analyze the data.
Results
A total of 400 questionnaires were distributed to the healthcare professionals and 331 participants responded, providing a response rate of 82.75%. The healthcare professionals comprised 161 physicians, 39 pharmacists, 21 pharmacist technicians, and 110 nurses. Most of the participants were female (n=198) and Saudi (61.9%). Most healthcare professionals (62.5%) were unaware of the term pharmacovigilance; the pharmacists and pharmacist technicians had the highest rate of pharmacovigilance awareness (60.5% of the pharmacists and 40% of pharmacist technicians).
Conclusion
There is a lack of awareness and knowledge of pharmacovigilance and ADR reporting among healthcare professionals working at KFHU.
The World Health Organization defines adverse drug reactions (ADRs) as “any response to a drug which is noxious and unintended and occurs at doses normally used in man for prophylaxis, diagnosis or therapy of disease or the modification of physiological function.”1 Globally, the prevalence of ADRs has been increasing in many countries, such as Sweden (12.0%), Norway (11.5%), New Zealand (12.9%), and Australia (16.6%),2 leading to increased patient-related morbidity and mortality in both the hospital and community settings. Studies have shown that ADRs are poorly reported by healthcare providers, particularly in developing countries.3,4
Once a drug is marketed, little is known about its safety profile. Information on unidentified ADRs is collected over time as the drug is used for different indications or in different subsets of people (for example, children), and this process causes the safety profile of the drug to change over its lifetime. Pharmacovigilance is defined as the “science and activities related to the detection, assessment, understanding, and prevention of adverse effects or any other possible drug-related problems.”5 The principal objectives of pharmacovigilance are to develop patient care and safety in relation to medication use; evaluate the benefits, harm, effectiveness, and risk of the medication; and efficiently communicate the safety of the medication to healthcare providers and the community.5 National pharmacovigilance centers were developed in most countries after the thalidomide tragedy in the 1960s.6
In Saudi Arabia, the National Pharmacovigilance Centre was established by the Saudi Food and Drug Authority (SFDA) in March 2009 (www.sfda.gov.sa.npc),7 and it is a member of the Uppsala Monitoring Centre in Sweden. The center gathers, evaluates, and communicates information from other members regarding the benefits, harm, effectiveness, and risks of the drugs. The spontaneous reporting system is the main way to collect information about ADRs in any setting, including hospitals. The success of any pharmacovigilance system highly depends on the contributions of healthcare professionals and the public, as well as the degree of cooperation and communication between them and the pharmacovigilance centers. Several studies have shown a lack of knowledge and awareness among healthcare professionals in Saudi Arabia.
A study of ADR reporting and pharmacovigilance in hospitals in Al-Madinah Al-Munawwarah, Saudi Arabia revealed a lack of knowledge and awareness of ADR reporting and pharmacovigilance among healthcare professionals working in hospitals.3 Another study in Saudi Arabia included 7 hospitals in Makkah. The study showed that healthcare professionals were aware of ADRs and pharmacovigilance and had positive attitudes about reporting them, but they faced many difficulties such as a lack of training, unavailability of forms, inadequate clinical knowledge, and a fear of reporting ADRs.2 In addition, a study performed at King Khalid University Hospital, Riyadh, Saudi Arabia assessed 116 physicians’ knowledge and attitudes regarding ADR reporting and pharmacovigilance. The study showed that 88.7% of the physicians did not know about the National Pharmacovigilance Centre and that 95.7% were not pleased with their training on ADR reporting. Furthermore, they emphasized the need for more education and training programs on pharmacovigilance systems.8
A cross-sectional survey of 12 governmental and private hospitals was performed in 3 main cities of Saudi Arabia (Riyadh, Jeddah, and Dammam) to examine Saudi healthcare professionals’ knowledge and awareness of pharmacovigilance. The study found that they had a narrow knowledge of pharmacovigilance, and that there was a need for a practical training program to improve the drug safety in Saudi Arabia.9 Moreover, in 2013, the National Pharmacovigilance Centre in Saudi Arabia revealed underreporting of ADRs mainly due to a lack of awareness of pharmacovigilance issues, complicated reporting systems, and a lack of motivation.2 A lack of awareness towards ADRs and ADR reporting among community pharmacists and healthcare professionals in the hospital setting has also been reported in other studies from Saudi Arabia.10
The aim of this survey was to document the knowledge and awareness of ADR reporting and pharmacovigilance systems among healthcare professionals working at King Fahd Hospital of the University (KFHU).
Methods
To explore previous studies on the same topic, the following keywords were used to cover all of the related articles: “pharmacovigilance”, “physicians”, “pharmacists”, “pharmacy technicians”, “nurses”, “knowledge”, “attitude”, “adverse drug reaction”, “practice”, “reporting,” “healthcare professionals,” “Saudi Arabia,” “hospitals”, “community”, “systematic review”, “meta-analysis”, “awareness”, “factors affecting reporting”, “causes of “underreporting” and “underreporting”. Some of these words were used in combination during the search. The search was performed using electronic databases such as Ovid and PubMed. The Google search engine was also used.
This descriptive cross-sectional study was conducted using a questionnaire. The study was conducted at KFHU, Al-Khobar, Kingdom of Saudi Arabia.
Inclusion and exclusion criteria
All of the healthcare professionals working at KFHU who dealt with medications on a daily basis were considered eligible and invited to take part in the study, including physicians, pharmacists, pharmacy technicians, and nurses. Pharmacists and pharmacy technicians with minimal dispensing activities, such as those working in medical stores or involved in the administration of total parenteral nutrition, were excluded from the study. All of the employees working in administrative positions were also excluded (for example, registrars).
Sampling strategy
All of the physicians, pharmacists, pharmacist technicians, and nurses working at KFHU were invited to take part in the study, with the exception of those who met the above-mentioned exclusion criteria. An online link to the questionnaire and study objective was distributed via E-mail to healthcare professionals working at KFHU. A hard copy of the questionnaire enclosed with a cover letter explaining the study’s aim and timeframe was also provided.
Design of the questionnaire
A self-administered questionnaire was used in this study, which was designed in accordance with previously published international literature.10-13 The questionnaire included 4 sections. The first was the demographics section, which included 5 questions. The other 3 sections contained 17 questions and addressed the following topics: knowledge and awareness of pharmacovigilance and ADRs, perception and attitude toward pharmacovigilance, and practices of ADR reporting. Two researchers reviewed the questionnaire and checked the consistency, clarity, and relevance of the questions. Slight modifications were recommended to enhance the clarity of the questions without changing the meaning. The questionnaire was distributed in English.
Ethical approval
The study was approved by the University of Dammam Institutional Review Board and was conducted between April 2015 and April 2016.
Statistical analysis
Statistical analysis was undertaken using IBM SPSS Statistics, version 23 (Armonk, NY: IBM Corp.).14 Descriptive statistics were used to analyze the data, and the results are presented as percentages and frequencies.
Results
Demographic and clinical characteristics of the sample
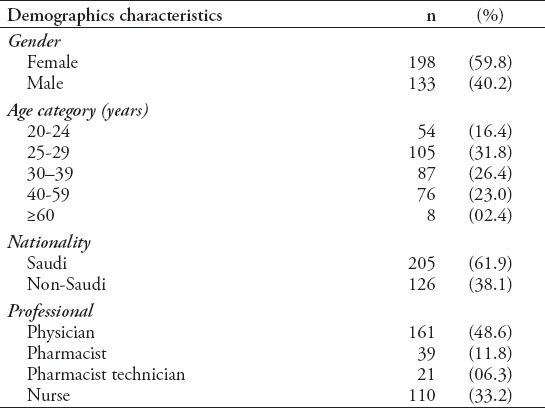
A total of 400 questionnaires were distributed to healthcare professionals, and 331 participants responded, providing a response rate of 82.75%. The healthcare professionals comprised of 161 physicians, 39 pharmacists, 21 pharmacist technicians, and 110 nurses. Most were female (n=198, 59.8%) and Saudi (n=205, 61.9%) (Table 1). The questionnaires were collected online and in the hospital.
Table 1.
Demographic characteristics of 331 healthcare professionals working at King Fahd Hospital of the University, Al-Khobar, Saudi Arabia.
Knowledge and awareness of pharmacovigilance and ADRs
In this section of the questionnaire, the healthcare professionals were asked if they were aware of the terms ‘pharmacovigilance’ and ‘ADRs’ and the type of ADRs that should be reported. Most of the healthcare professionals (62.5%) were unaware of the term ‘pharmacovigilance’. The pharmacists and pharmacist technicians had the highest percentage of pharmacovigilance awareness (60.5% of the pharmacists and 40% of the pharmacist technicians), followed by nurses (18%) and physicians (12.1%). In addition, a majority of responders (44.3%) correctly answered the second question regarding the definition of pharmacovigilance. Furthermore, 46.1% provided the correct answer regarding the definition of ADRs, and 71.6% stated that all types of ADRs should be reported. They were also asked if they were aware of any pharmacovigilance centers in Saudi Arabia, whether they had attended any courses or workshops on pharmacovigilance, and how they prefer to report an ADR. A total of 62.2% of the healthcare professionals were unaware of any pharmacovigilance centers, and 89.9% had not attended any courses and/or workshops; 36.1% believed that the best way to report an ADR was using the ADR form (Figure 1).
Figure 1.
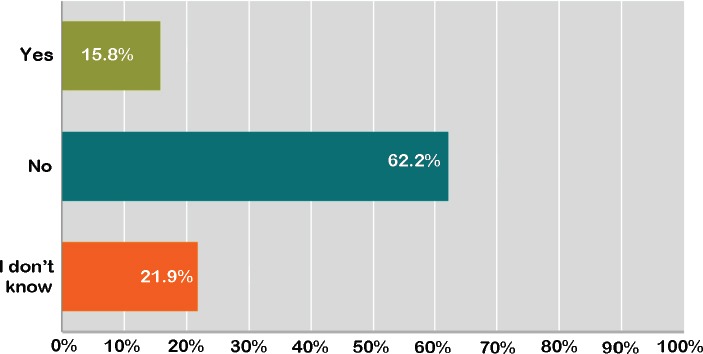
Awareness of the healthcare professionals in King Fahd Hospital of the University, Al-Khobar, Saudi Arabia toward the national pharmacovigilance system.
Perception and attitude toward pharmacovigilance and ADR reporting
The healthcare professionals were asked about the necessity of reporting an ADR and whether they believe, it is a professional obligation; 87.1% agreed that ADRs need to be reported and 75.9% agreed that it is an obligation. They were also asked if pharmacovigilance should be included in the undergraduate curriculum, and 65.9% answered “yes” (Figure 2).
Figure 2.
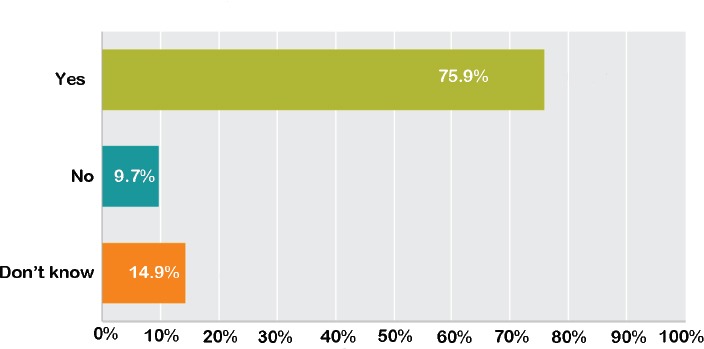
Percetion and attitude of the healthcare professionals in King Fahd Hospital of the University, Al-Khobar, Saudi Arabia toward pharmacovigilance system and adverse drug reactions.
Practices of ADR reporting
The healthcare professionals were then asked about ADR reporting. This included questions about monitoring systems, reporting forms, whether they had reported ADRs, whether they knew where to obtain the forms, to whom to report the ADRs, and what factors may discourage them from reporting ADRs. Regarding monitoring systems, 44.9% of participants stated that they were unaware of the existence of a hospital reporting system, whereas 30.5% did not know whether a system was available in the hospital. Moreover, 88.8% had never reported, submitted, or identified any ADR reports, and 74.1% did not know where to obtain the form. In response to the question about to whom the ADR should be reported, 28.2% answered to the Ministry of Health, 44.7% answered to the SFDA, 7.2% answered to the drug company, 5.8% answered to the prescriber, and 14.1% answered “other”, without specifying to whom they should report. Finally, the participants were asked about the factors that may discourage them from reporting ADRs. The responses were as follows: 43.8% did not know how to report an ADR, 17.5% did not believe that it was important, 8.6% thought that managing patients was more important, 9.9% stated that it is not part of their job, and 10.3% mentioned patient confidentiality issues.
Discussion
Adverse drug reactions are the primary cause of patient harm in healthcare. They are preventable and have the potential for re-occurrence. In some countries, ADRs rank among the top 10 leading causes of mortality.5 To prevent or minimize harm to patients, improvements in public health and tools for evaluating and monitoring drug safety in clinical use are crucial. This means that well-organized pharmacovigilance and ADR reporting systems must be established.
We performed a questionnaire survey at KFHU assessing the knowledge and awareness of ADR reporting and pharmacovigilance systems among healthcare professionals. In our study, the response rate was 82.75%, which is similar to that reported in other studies.3,15,16 Our results showed a lack of awareness and knowledge among healthcare professionals. This finding is similar to other studies from different countries indicating practical training program for healthcare professionals to improve drug safety in Saudi Arabia.3,9,11-13 A survey of private doctors was performed in Rajkot City, India. A total of 600 questionnaires were distributed, and 332 doctors responded. The study found the need for awareness among doctors and the need to improve ADR reporting,17 poor knowledge of pharmacovigilance, and attitudes associated with a high degree of underreporting.16,17 A cross-sectional survey of 12 governmental and private hospitals was performed in 3 main cities of Saudi Arabia (Riyadh, Jeddah, and Dammam) to examine the knowledge and awareness of Saudi healthcare professionals regarding pharmacovigilance. The study found a narrow knowledge of pharmacovigilance and the need for a practical training program.
Many studies have found that ADR underreporting is a worldwide problem, even in countries where pharmacovigilance programs are well established such as the United Kingdom.11,18,19 Although most healthcare professionals are willing to report ADRs and understand the importance of reporting them, some reasons for underreporting include a lack of awareness in the reporting method and forms needed as well as the belief that it is not their responsibility or obligation to report an ADR.15 In addition, pharmacovigilance should be added to undergraduate curriculums because this will eventually impact the knowledge and awareness of the new generation of healthcare professionals, leading to better patient care.
Implications for clinical practice and future recommendations
In clinical practice, well-organized pharmacovigilance and ADR reporting systems will lead to intelligent, evidence-based use of drugs and the possibility of preventing or reducing several ADRs. Healthcare professionals play a key role in pharmacovigilance programs. To improve the ADR reporting process, healthcare professionals must be taught and trained in ADR reporting. Furthermore, improvements in ADR reporting will reduce health care costs. Patients should be encouraged to report ADRs using forms provided online by the pharmacovigilance center or by contacting their health provider; this can be performed by advertising patient self-reporting and has been described in various studies.
In Saudi Arabia, the National Pharmacovigilance Centre has made both online ADR reporting forms and hard paper copies available to encourage ADR reporting by healthcare professionals and the public.7 Results from the current study showed that healthcare professionals in general had poor knowledge about pharmacovigilance and ADRs. This calls for the need to improve the knowledge and awareness about these concepts, which will reflect positively on the practice of ADR reporting and the success of the Pharmacovigilance Center. This can be accomplished by providing educational programs, training courses, and presentations to healthcare professionals. Patient involvement is also essential for improving knowledge, attitudes, and perceptions about ADRs and increasing the numbers of ADR reports.20 In KFHU, an office for Quality and Drug Safety was developed with the aim of improving the pharmacovigilance system and ADR reporting in the hospital. Future studies involving this office are being planned to help improve the pharmacovigilance system.
Study limitations
Our study had a relatively small sample size, the study period was short, and the study was limited to one hospital.
Implications for future research
Further studies are needed to reinforce the effectiveness of and need for pharmacovigilance.
In conclusion, this study highlighted the lack of knowledge and awareness among healthcare professionals in the field of pharmacovigilance and ADR reporting. Educational programs and the establishment of strategies that can be used to improve pharmacovigilance systems and ADR reporting in hospitals are needed. This will increase healthcare professionals’ role in reporting ADRs, leading to a positive impact on overall patient care.
Acknowledgment
The author thanks the Deanship of Scientific Research at the University of Dammam, Dammam, Kingdom of Saudi Arabia for funding this research.
Footnotes
Ethical Consent.
All manuscripts reporting the results of experimental investigations involving human subjects should include a statement confirming that informed consent was obtained from each subject or subject’s guardian, after receiving approval of the experimental protocol by a local human ethics committee, or institutional review board. When reporting experiments on animals, authors should indicate whether the institutional and national guide for the care and use of laboratory animals was followed.
References
- 1.International drug monitoring: the role of national centres. World Health Organ Tech Rep Ser. 1972;498:1–25. [PubMed] [Google Scholar]
- 2.Al-Hazmi N, Naylor IL. Attitude and awareness of adverse drug reaction reporting by health professionals in seven hospitals in the Holy City of Makkah, Kingdom of Saudi Arabia. Clin Trials. 2013;3:3. [Google Scholar]
- 3.Abdel-Latif MM, Abdel-Wahab BA. Knowledge and awareness of adverse drug reactions and pharmacovigilance practices among healthcare professionals in Al-Madinah Al-Munawwarah, Kingdom of Saudi Arabia. Saudi Pharm J. 2015;23:154–161. doi: 10.1016/j.jsps.2014.07.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Suyagh M, Farah D, Abu Farha R. Pharmacist’s knowledge, practice and attitudes toward pharmacovigilance and adverse drug reactions reporting process. Saudi Pharm J. 2015;23:147–153. doi: 10.1016/j.jsps.2014.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Pharmacovigilance: Ensuring the Safe Use of Medicines–WHO Policy Perspectives on Medicines, No. 009, October. 2004. [[Accessed 14th September 2015]]. Available from: http://apps.who.int/medicinedocs/en/d/Js6164e/
- 6.Fintel B, Samaras AT, Carias E. The thalidomide tragedy: lessons for drug safety and regulation. Northwestern University (IL): Helix; 2015. [Google Scholar]
- 7.The Saudi Food and Drug Authority. The National Pharmacovigilance Centre (NPC) [[Updated 2016; Accessed 2015 September 10]]. Available from URL: www.sfda.gov.sa.npc .
- 8.Al-Arifi MN, Mayet AY, Wajid S, Al-Saadi M, Babelghaith ISD, Al Ayoubi FZ. Knowledge, attitude and perception of physicians towards adverse drug reaction reporting at king khalid university hospital, Riyadh, Saudi Arabia. Trop J Pharm Res. 2015;14:907. [Google Scholar]
- 9.Alshammari TM, Alamri KK, Ghawa YA, Alohali NF, Abualkol SA, Aljadhey HS. Knowledge and attitude of health-care professionals in hospitals towards pharmacovigilance in Saudi Arabia. Int J Clin Pharm. 2015;37:1104–1110. doi: 10.1007/s11096-015-0165-5. [DOI] [PubMed] [Google Scholar]
- 10.Al-Worafi YM. Re: Improving pharmacovigilance in Europe. BMJ. 2014;340:c1694. doi: 10.1136/bmj.c1694. [DOI] [PubMed] [Google Scholar]
- 11.Rajesh R, Vidyasagar S, Varma DM. An educational intervention to assess knowledge attitude practice of pharmacovigilance among health care professionals in an Indian tertiary care teaching hospital. International Journal of Pharm Tech Research. 2011;3:678–692. [Google Scholar]
- 12.Chinenye JU, Micheael OU. Health workers and hospital patients knowledge of pharmacovigilance in Sokoto, north-west Nigeria. Nigerian Journal of Pharmaceutical Sciences. 2012;11:31–40. [Google Scholar]
- 13.Jose J, Jimmy B, Al-Ghailani A, Al Majali M. A cross sectional pilot study on assessing the knowledge, attitude and behavior of community pharmacists to adverse drug reaction related aspects in the Sultanate of Oman. Saudi Pharm J. 2014;22:163–169. doi: 10.1016/j.jsps.2013.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.IBM Corp. Released 2014. IBM SPSS Statistics for Windows, Version 23.0. Armonk (NY): IBM Corp; 2014. [Google Scholar]
- 15.Mahmoud MA, Alswaida Y, Alshammari T, Khan TM, Alrasheedy A, Hassali MA, et al. Community pharmacists’ knowledge, behaviors and experiences about adverse drug reaction reporting in Saudi Arabia. Saudi Pharm J. 2014;22:411–418. doi: 10.1016/j.jsps.2013.07.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hardeep Bajaj JK, Rakesh K. A survey on the knowledge, attitude and the practice of pharmacovigilance among the healthcare professionals in a teaching hospital in northern India. J Clin Dia Res. 2013;7:97–99. doi: 10.7860/JCDR/2012/4883.2680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Karelia BN, Piparava KG. Knowledge, attitude and practice of pharmacovigilance among private healthcare professionals of Rajkot city. Int J Basic Clin Pharmacol. 2014;3:50–53. [Google Scholar]
- 18.Fadare JO, Enwere OO, Afolabi AO, Chedi BAZ, Musa A. Knowledge, Attitude and Practice of Adverse Drug Reaction Reporting among Healthcare Workers in a Tertiary Centre in Northern Nigeria. Trop J Pharm Res. 2011;10:235–242. [Google Scholar]
- 19.Kamtane R, Jayawardhani V. Knowledge, attitude and perception of physicians towards adverse drug reaction reporting: A pharmacoepidemiology study. Asian J Pharm Clin Res. 2012;3:210–214. [Google Scholar]
- 20.Khalili H, Mohebbi N, Hendoiee N, Keshtkaar AA, Dashti-Khavidaki S. Improvement of knowledge, attitude and perception of healthcare workers about ADR, a pre- and post-clinical pharmacists’ interventional study. BMJ Open. 2012;2:e000367. doi: 10.1136/bmjopen-2011-000367. [DOI] [PMC free article] [PubMed] [Google Scholar]