

Abstract
Objectives
To investigate the prevalence of obesity among elementary school children and to examine the association between obesity and caries activity in the mixed dentition stage.
Methods
This cross-sectional study was conducted in King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia between September 2014 and June 2015 using a multi-stage stratified sample of 915 elementary school children (482 boys, 433 girls) in Jeddah, Saudi Arabia. Anthropometric measurements, consisting of height, weight, body mass index (BMI), and waist circumference (WC), were obtained. Children were classified as underweight/healthy, overweight, or obese and as non-obese or obese according to their BMI and WC, respectively. Each child’s caries experience was assessed using the decay score in the primary and permanent teeth.
Results
Based on BMI, 18% of children were obese, 18% were overweight, and 64% were underweight/normal. Based on WC, 16% of children were obese, and 84% were non-obese. Girls had a significantly higher prevalence of obesity based on WC measurements (p<0.001), but not BMI. Children enrolled in private schools had a significantly higher prevalence of obesity (p<0.05) than those in public schools. For primary and permanent teeth combined, children with higher BMI and WC had a lower prevalence of caries (p<0.05).
Conclusion
The prevalence of obesity was high among male and female elementary school children. Overall caries activity was inversely proportional to BMI and WC.
Obesity is a complex condition with a serious impact on overall health, both physically and psychologically. It is defined by the World Health Organization (WHO) as “abnormal or excessive fat accumulation that may impair health”.1 Overweight, in contrast, is defined as “a body mass index (BMI) of 25 kg/m2 or more”. The WHO uses BMI to classify obesity and it is calculated by dividing weight in kilograms by the square of height in meters (kg/m2). Given the limitations of BMI, waist circumference (WC) has been suggested as a more accurate predictor of the risk of obesity.2
Obesity remains a constant threat to overall health by causing several other medical conditions. At any age, obesity can affect the cardiovascular, respiratory, skeletal, and endocrine systems.3,4 It can also increase the risk of breast cancer in adolescence.5 Further, obesity not only affects the individual physically, but also negatively affects the psyche and self-esteem.6
The prevalence of obesity has been increasing rapidly worldwide in all age and socioeconomic groups, both in developed and developing countries.7 A report from South Africa has documented a significant rise in obesity in children aged 6-9 years of age.8 Similarly, in Australia, a review by Dyer et al9 reported an increase in the prevalence of obesity with age in the childhood years, with a rate of 27.5% in children aged 5-9 years and 38.5% in those aged 10-14 years. In the UK, more than 3% of children aged 10-11 years had severe obesity according to a study by Ells et al.10 A high prevalence of obesity has been found among school children in France and China.11,12 Since the 1970s, the prevalence of obesity in the USA has increased by 2-fold in children aged 2-5 years and by 3-fold in children aged 6-11 years.13,14 For these reasons, obesity is now regarded as an increasing problem in pediatrics and has been referred to as “an epidemic” by the WHO and in the literature.4,7,15,16
Despite improved preventive regimes and advances in early diagnostic techniques, dental caries remains a highly prevalent childhood disease, especially in Saudi Arabia.1,17-19 Because high-calorie diets are a major cause of obesity, it is speculated that these diets could also cause dental caries. Numerous studies have been performed to determine whether an association exists between overweight/obesity and caries; however, the results of these studies have been inconsistent.20-22
In Saudi Arabia, obesity is a problem at any age. A review in 2011 reported an increase in obesity with increasing age. In preschoolers, the prevalence of obesity was reported to be 8-9%, whereas in the age group of 30-60 years, rates were 70-85% in men and 75-88% in women.23 Jeddah is the second largest city in Saudi Arabia and is the commercial capital of the country. It is located along the eastern coast of the Red Sea and has a population of 3.4 million, of which more than 30% are younger than 15 years of age.24 Although studies investigating obesity among Jeddah school children have been found in the literature, there is as yet no published work targeting the entire population of elementary school children in Jeddah. The aims of this study were to investigate the prevalence of obesity and overweight among boys and girls in public and private elementary schools and to determine any associations between obesity and caries activity in the mixed dentition stage among school children in Jeddah.
Methods
The ethics committee of the Faculty of Dentistry at King Abdulaziz University (KAUFD) approved the protocol for this observational, analytical, cross-sectional study. The targeted population included all Saudi and non-Saudi children registered in elementary schools in Jeddah according to the Ministry of Education. The total population was 239,565 children. According to previous population-based studies, the prevalence of overweight and obesity in the target children was hypothesized to be 30%.25 Thus, to calculate the sample size, the percentage frequency of the outcome factor was set at 30% with 3% confidence limits. In addition, the confidence level was set at 95%, the significance level at 0.05, and the power at 85%. The estimated sample size was 894 children. The sample size was calculated using the free web-based operating system OpenEpi, version 2.26
A multistage stratified random sampling of elementary students in Jeddah was undertaken. There were 121,090 male and 118,475 female students distributed across 621 public and private elementary schools. Based on this number, a male to female ratio of 1:0.97 was used to divide the sample of 894 students into the corresponding number of subjects for each gender, resulting in 454 male and 440 female students.
The decision was made that the school would be used as the unit for sample selection according to a numbered list that was prepared previously. Two numbers representing a private school or a public school were selected in each of Jeddah’s main 4 districts (north, east, south, and west) for each gender in order to meet the required sample size. Third-grade school children were selected to ensure that all subjects were in a stage of mixed dentition. For each school, two-third grade classes were randomly assigned (by the bowl method) to join the study. If the school was found to have only one third-grade class, a different school was randomly selected. Approval to visit the selected schools and collect data from the students was obtained from the Saudi Ministry of Education in Jeddah. Moreover, approval of the school principal was obtained prior to the school visit. During the first visit, consent forms with information about the study were distributed to the students. Students were encouraged to bring back the consents on the following morning. A total of 1,200 consent forms were distributed.
At the next school visit, children who had brought back a signed consent form were examined. There were 915 students in total; 231 were male students in private schools, 251 were male students in public schools, 232 were female students in private schools, and 201 were female students in public schools. Data collection took place over the 10 months from September 2014 to June 2015.
Children were eligible to participate in the study if they were in the third grade, were aged 7-10 years, and had returned a signed parental consent form.
I. Anthropometric measurements
Anthropometric measurements, consisting of height, weight, and WC, were obtained by 3 calibrated investigators. The calibration exercise was performed using a detailed rubric for height and WC measurement. The inter-examiner reliability was assessed in 20 patients attending KAUFD clinics, and the kappa score was 0.77. The intra-examiner reliability was assessed by using 10 patients attending KAUFD clinics who were examined on 2 occasions one week apart, and the kappa score was 0.85. In the event of disagreement between investigators, consensus was reached by retaking the measurements. Two readings for each measurement were performed for each child. The median of these readings was used for the analysis.
Height was recorded using a commercial non-elastic measuring tape. The children stood barefoot, with shoulders straight, legs hanging freely, and head looking straightforward. A point was marked on large white cardboard fixed to the wall that corresponded to the highest point of the head. The tape was used to measure the distance from the floor to that point. Height was rounded to the nearest 0.1 cm.
An electronic weight scale was used to measure body weight with light clothing on and without shoes, jackets, or heavy accessories. The readings were rounded to the nearest 100 g.
Waist circumference was measured using a non-elastic measuring tape at the highest point of the iliac crest when the child was standing at minimal respiration. WC was rounded to the nearest 0.1 cm.2,14
Body mass index was calculated for each student by dividing the weight in kilograms by the square of the height in meters (kg/m2).
Dental charting
Dental charting was performed by 2 calibrated investigators other than the coauthors who obtained the anthropometric measurements. The calibration exercise was performed using a detailed rubric for dmf/DMF scoring according to the National Institute of Dental Research criteria.27 The inter-examiner reliability was assessed using 30 patients attending KAUFD clinics, and the kappa score was 0.90. The intra-examiner reliability was assessed using 10 patients attending KAUFD clinics examined on 2 occasions with a one-week interval between occasions, and the kappa score was 0.85. In the event of disagreement, consensus was reached by retaking the measurements.
Diseased or filled scores (df/DF) were used to assess the child’s caries experience in the primary and permanent teeth, respectively. Missing teeth were not charted because of insufficient accounting for the reasons for extraction. The examination was non-invasive and performed under torchlight and used basic infection control measures. The children were seated in front of the examiner on a school chair during the examination. A round-ended dental probe, a sterile, flat-surfaced non-magnifying mouth mirror, gauze, and cotton rolls were used. Teeth that contained temporary restorations were marked as d for primary or D for permanent teeth. Teeth with fissure sealants were marked as sound, as were teeth with white spot lesion/s only. After the dental examination, a confidential report was sent to the parents, informing them about their child’s oral health status and treatment needs along with a referral letter to KAUFD.
Data analysis
In this study, the classification of overweight and obesity in children was based on 2 measurements, namely, BMI and WC. The BMI was categorized using the Saudi age-specific and gender-specific BMI percentiles introduced by Al Herbish et al28 and the cut-off points suggested by Barlow & Expert29 The principal cutoff points and their corresponding classifications were as follows: underweight (<5th percentile), normal (5th-84th percentiles), overweight (85th-94th percentiles), and obese (≥95th percentile). With regard to WC, a cutoff of ≥90th age-specific and gender-specific percentile was used to define obesity.30 Diseased scores (d/D) were used to assess the caries experience in the primary and permanent teeth.
Medians and interquartile ranges (IQRs) were reported for the continuous subject characteristics. Frequencies and percentages were reported for the categorical characteristics, as well as obesity status and caries experience in the primary and permanent teeth. The associations between obesity status, caries experience, gender, and type of school attended were analyzed using the Chi-square test, as were the associations between obesity status and caries in the primary, permanent, and both primary and permanent teeth. The significance level was set at p<0.05. The statistical analysis was conducted using STATA version 13.0 software (StataCorp, College Station, TX, USA).
Results
The study included 915 elementary school children. The characteristics of the study population are shown in Table 1. The median (IQR) age of the participants was 9.0,8,9 years, with a range of 7-10 years. Girls constituted 47% of the sample. The students were enrolled in private (51%) or public (49%) elementary schools representing the 4 districts of Jeddah city. The median (IQR) BMI of the participants were 17 (15, 22) kg/m2 and WC 62 (57, 70) cm. Based on the BMI obesity classification, 18% of the students were obese, 18% were overweight, and 64% were underweight/normal. Based on the WC obesity classification, 16% of the students were obese, and 84% were non-obese.
Table 1.
Characteristics of the 915 elementary school children.
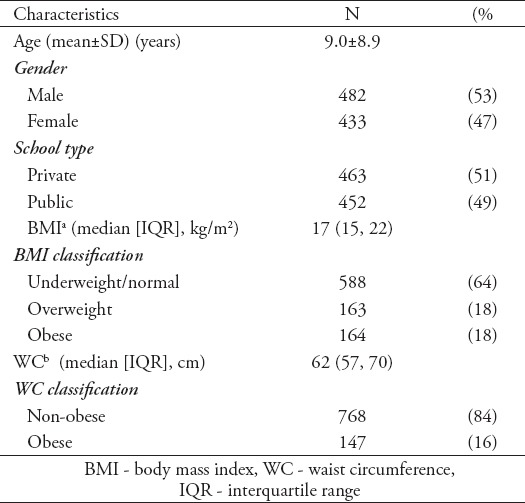
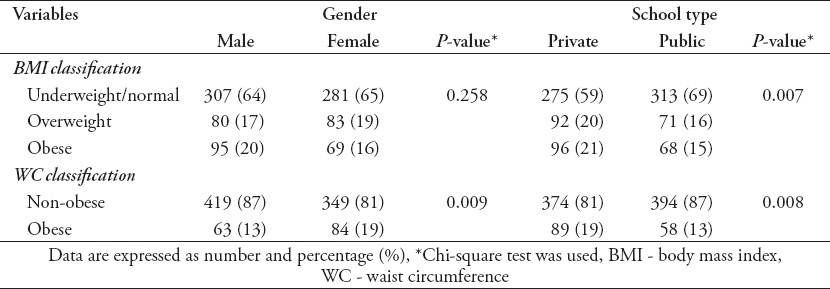
Table 2 shows the association between obesity status and gender or type of school attended. Girls had a significantly higher prevalence of obesity based on WC measurements (p=0.009) but not BMI (p=0.258). Based on WC, approximately 19% of girls were obese compared with 13% of boys. With regard to type of school, children enrolled in private schools had a significantly higher prevalence of obesity. Based on BMI, 41% of children from private schools were classified as overweight or obese compared with 31% of children from public schools (p=0.007). Based on WC, 19% of children from private schools were classified as obese compared with 13% of children from public schools (p=0.008).
Table 2.
Prevalence of obesity by gender and school type.
The relationship between the prevalence of dental caries and gender, or type of school are summarized in Table 3. The prevalence of dental caries in the primary, permanent dentition was 79%, and both primary (59%) and permanent (86%). There was no significant difference in prevalence of caries between girls and boys; however, there was a significant difference in caries prevalence between children enrolled in private and public schools. Children in private schools had a lower prevalence of caries in their primary teeth (p<0.001), permanent teeth (p<0.001), and both primary and permanent dentition combined (p<0.001).
Table 3.
Prevalence of caries (primary, permanent and both) by gender and school type.
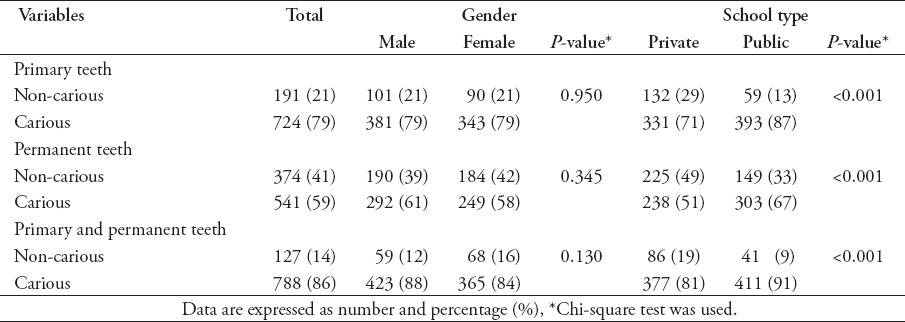
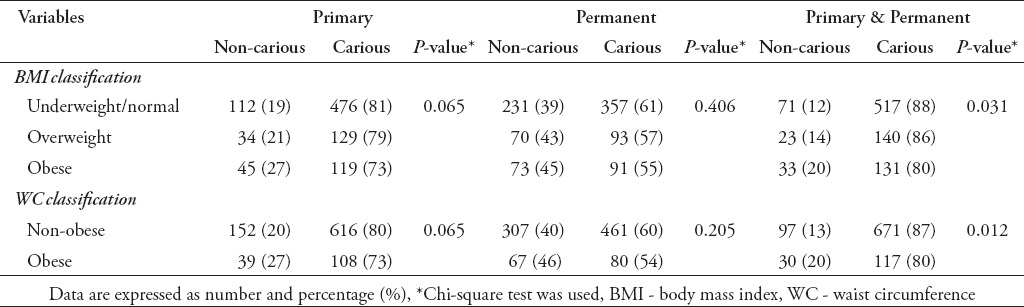
Table 4 shows the association between prevalence of caries and obesity status. Although the prevalence of caries in primary and permanent teeth was lower in children with higher BMI and WC, the differences were not statistically significant. For primary and permanent teeth combined, children with higher BMI had a lower prevalence of caries (p=0.031). The prevalence of caries was 88% for underweight/normal, 86% for overweight, and 80% for obese children. The prevalence of caries was also significantly lower among obese children (80%) than in non-obese children (87%; p=0.012) when obesity was classified based on WC.
Table 4.
Association between caries experience (primary, permanent and both) and obesity status.
Discussion
This cross-sectional survey revealed a high prevalence of obesity (36%) in elementary school children in Jeddah, Saudi Arabia. Several reports have shown that the prevalence of obesity and overweight among children is increasing in developed and developing countries, and this is becoming a public health concern.31 What was previously viewed as an adult problem is now becoming a health care issue for children as well.32 Saudi Arabia and the Gulf region are not exempt because surveys have reported a similar pattern in children of all age groups.25 It is plausible that the rapid economic changes experienced in Saudi Arabia over the last decade have changed local lifestyle and dietary habits.34-36 A study by Alghadir et al37 in 2015 reported high consumption of high-fat fast foods and drinks containing large amounts of sugar among Saudi schoolchildren. Sugar-sweetened carbonated beverages have been found to be associated with higher BMI and poor dietary choices involving, for example, frequent desserts, savory snacks, and total sugar consumption, as well as with lower milk consumption.37 The consumption of such beverages is high in Saudi children, which might explain why they have a high prevalence of obesity.37 Our research showed no significant difference in prevalence of obesity between boys and girls based on BMI. This finding is in agreement with the findings of the 2015 National Health and Nutrition Examination Survey.38 However, it is not consistent with some reports from Saudi Arabia showing higher rates of obesity in boys than in girls. A steady increase in obesity with age was noted in Saudi children such that by the age of 14-18 years, approximately 36% of boys and 19% of girls were obese.25 In contrast, Mahfouz et al39 found obesity to be more prevalent among in adolescent girls than in their male counterparts in the southwestern region.
Based on WC measurements, obesity rates were higher in girls (19%) than in boys (13%). It has been reported that boys are significantly more active and more likely to meet physical activity guidelines than girls.40 Similarly, other studies in developing countries have shown a lower prevalence of obesity in boys than in girls, which could be due to different cultural habits regarding diet and physical activity.35,41 As this study was school-based, we investigated the relationship between prevalence of obesity and type of school. Our data show that, based on BMI, obesity was more prevalent in private schools (41%) than in public schools (31%). This finding is consistent with prevalence of obesity based on WC (19% in private schools versus 13% in public schools) and with reports of significantly higher percentages of obesity in private Indian schools.42,43 The higher prevalence of obesity in private schools might be related to co-existing factors rather than to the type of schooling per se. Although most research has indicated that people of lower socioeconomic status have higher rates of obesity.44-47 there are some reports indicating a greater prevalence in the higher socioeconomic classes.47,48 For example, wealthier families are more likely to drive their children to school and not rely on walking or public transport. In addition, they are also more likely to provide more frequent and larger meals as well as afford computer and video games.41
Obesity and caries are concomitant conditions in many populations, largely because of common risk factors, including consumption of highly caloric and cariogenic substances. The current data show that the prevalence of dental caries is significantly lower in obese children than in their non-obese counterparts. There has been conflicting evidence in the literature with regard to the nature and direction of this association. Similar to our results, it has been shown that dental caries is inversely associated with all anthropometric outcomes in Saudi children, including height and weight, suggesting that untreated caries is associated with poorer growth.18 Furthermore, a survey by Werner et al49 showed that a smaller proportion of obese children than normal weight children present with dental caries at their dental initial examinations.
Dental caries could be proposed to have an indirect impact on obesity. Children with severe dental caries and pain while chewing might not be able to eat enough to meet nutritional requirements, which could ultimately result in malnutrition and impairment of growth.18,50 In addition, caries can affect the child’s weight indirectly via immune, endocrine, or metabolic responses leading to malnutrition, retardation of growth, or impairment of nutrient absorption.51
In contrast, multiple studies have demonstrated that both conditions share common risk factors, which would support a positive association. The role of diet, for example, is significant in the development of both diseases. Healthy eating, with the inclusion of fruits and vegetables, promotes better overall health. Children who make poor food choices are at greater risk of becoming obese and having dental caries.46,52 Willershausen et al53 found a significantly lower percentage of obese children to have caries-free teeth than normal-weight children.53 Further, an association between high BMI and incidence of permanent molar smooth surface caries was documented by Hilgers et al.21 Nevertheless, some investigators have found no correlation between childhood obesity and dental caries.20,54
In conclusion, the prevalence of obesity was high among male and female elementary school children. Obesity was more prevalent in elementary school girls and in private school students. Overall caries activity was inversely proportional to BMI and WC. It is of pivotal importance for health care providers and education policy-makers to raise public awareness of the obesity epidemic and to implement strategies to prevent, identify, and manage it at earlier ages and stages. Pediatric dentists could also play an important role in preventing obesity via dietary counseling and medical referrals, which could benefit both dental and overall health in children.
Study limitations
Limitations of this study include: no information was gathered on medical history, nutritional habits, socioeconomic status, or activity level of the children. Further more, despite meticulous clinical examination was used to assess caries activity, but no radiographs were used.
This study confirms the high prevalence of obesity in school children. It also shows that rates of dental caries activity are inversely proportional to obesity. Future studies containing larger samples are needed to evaluate the effect of obesity on specific types of caries (fissure versus smooth surface caries and anterior versus posterior caries). Furthermore, investigators are encouraged to investigate the association between obesity and risk factors, in particular socioeconomic status, nutritional status, and parental level of education.
Acknowledgment
This project was funded by the Deanship of Scientific Research (DSR), King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia. The authors are grateful for the technical and financial support provided by the DSR, and we would like to acknowledge the help of Dr. Dania Bahdaila and Dr. Hammam Bahammam in data collection.
Footnotes
Statistics.
Excerpts from the Uniform Requirements for Manuscripts Submitted to Biomedical Journals updated November 2003.
Available from www.icmje.org
Describe statistical methods with enough detail to enable a knowledgeable reader with access to the original data to verify the reported results. When possible, quantify findings and present them with appropriate indicators of measurement error or uncertainty (such as confidence intervals). Avoid relying solely on statistical hypothesis testing, such as the use of P values, which fails to convey important information about effect size. References for the design of the study and statistical methods should be to standard works when possible (with pages stated). Define statistical terms, abbreviations, and most symbols. Specify the computer software used.
References
- 1.World Health Organization. Obesity and over- weight. [[Updted 2015 Accessed 2008 September]]. Available from: http://www.who.int/media-centre/factsheets/fs311/en/index.html .
- 2.Janssen I, Katzmarzyk PT, Ross R. Waist circumference and not body mass index explains obesity-related health risk. Am J Clin Nutr. 2004;79:379–384. doi: 10.1093/ajcn/79.3.379. [DOI] [PubMed] [Google Scholar]
- 3.Sinha R, Fisch G, Teague B, Tamborlane WV, Banyas B, Allen K, et al. Prevalence of impaired glucose tolerance among children and adolescents with marked obesity. N Engl J Med. 2002;346:802–810. doi: 10.1056/NEJMoa012578. [DOI] [PubMed] [Google Scholar]
- 4.Corey KE, Kaplan LM. Obesity and liver disease: the epidemic of the twenty-first century. Clin Liver Dis. 2014;18(1):1–18. doi: 10.1016/j.cld.2013.09.019. [DOI] [PubMed] [Google Scholar]
- 5.Stoll BA. Teenage obesity in relation to breast cancer risk. Int J Obes Relat Metab Disord. 1998;22:1035–1040. doi: 10.1038/sj.ijo.0800769. [DOI] [PubMed] [Google Scholar]
- 6.Strauss RS. Childhood obesity and self-esteem. Pediatrics. 2000;105:e15. doi: 10.1542/peds.105.1.e15. [DOI] [PubMed] [Google Scholar]
- 7.Organization WH. Controlling the global obesity epidemic. [[cited 2003]]. Available from: http://www.who.int/nutrition/topics/obesity/en/
- 8.Pienaar AE. Prevalence of overweight and obesity among primary school children in a developing country: NW-CHILD longitudinal data of 6-9-yr-old children in South Africa. BMC Obes. 2015;2:2. doi: 10.1186/s40608-014-0030-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dyer SM, Gomersall JS, Smithers LG, Davy C, Coleman DT, Street JM. Prevalence and Characteristics of Overweight and Obesity in Indigenous Australian Children: A Systematic Review. Crit Rev Food Sci Nutr. :2015, 0. doi: 10.1080/10408398.2014.991816. [DOI] [PubMed] [Google Scholar]
- 10.Ells LJ, Hancock C, Copley VR, Mead E, Dinsdale H, Kinra S, et al. Prevalence of severe childhood obesity in England 2006-2013. Arch Dis Child. 2015;100:631–636. doi: 10.1136/archdischild-2014-307036. [DOI] [PubMed] [Google Scholar]
- 11.Thibault H, Carriere C, Langevin C, Kossi Deti E, Barberger-Gateau P, Maurice S. Prevalence and factors associated with overweight and obesity in French primary-school children. Public Health Nutr. 2013;16:193–201. doi: 10.1017/S136898001200359X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.He F, Liu J. Prevalence of obesity among primary students from 2009 to 2014 in China: an update meta-analysis. Int J Clin Exp Med. 2014;7:5348–5352. [PMC free article] [PubMed] [Google Scholar]
- 13.Koplan JP, Liverman CT, Kraak VI. Committee on Prevention of Obesity in C Youth. Preventing childhood obesity: health in the balance: executive summary. J Am Diet Assoc. 2005;105:131–138. doi: 10.1016/j.jada.2004.11.023. [DOI] [PubMed] [Google Scholar]
- 14.Li C, Ford ES, Mokdad AH, Cook S. Recent trends in waist circumference and waist-height ratio among US children and adolescents. Pediatrics. 2006;118:e1390–e1398. doi: 10.1542/peds.2006-1062. [DOI] [PubMed] [Google Scholar]
- 15.Vann WF, Jr, Bouwens TJ, Braithwaite AS, Lee JY. The childhood obesity epidemic: a role for pediatric dentists? Pediatr Dent. 2005;27:271–276. [PubMed] [Google Scholar]
- 16.Slyper AH. The pediatric obesity epidemic: causes and controversies. J Clin Endocrinol Metab. 2004;89:2540–2547. doi: 10.1210/jc.2003-031449. [DOI] [PubMed] [Google Scholar]
- 17.Al Agili DE. A systematic review of population-based dental caries studies among children in Saudi Arabia. Saudi Dent J. 2013;25:3–11. doi: 10.1016/j.sdentj.2012.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Alkarimi HA, Watt RG, Pikhart H, Sheiham A, Tsakos G. Dental caries and growth in school-age children. Pediatrics. 2014;133:e616–e623. doi: 10.1542/peds.2013-0846. [DOI] [PubMed] [Google Scholar]
- 19.Khan SQ, Khan NB, Arrejaie AS. Dental caries. A meta analysis on a Saudi population. Saudi Med J. 2013;34:744–749. [PubMed] [Google Scholar]
- 20.Tripathi S K, Kamala B.K. Relationship between obesity and dental caries in children - A preliminary study. J Int Oral Health. 2010;2:65–72. [Google Scholar]
- 21.Hilgers KK, Kinane DE, Scheetz JP. Association between childhood obesity and smooth-surface caries in posterior teeth: a preliminary study. Pediatr Dent. 2006;28:23–28. [PubMed] [Google Scholar]
- 22.Willerhausen B, Blettner M, Kasaj A, Hohenfellner K. Association between body mass index and dental health in 1,290 children of elementary schools in a German city. Clin Oral Investig. 2007;11:195–200. doi: 10.1007/s00784-007-0103-6. [DOI] [PubMed] [Google Scholar]
- 23.Ng SW, Zaghloul S, Ali HI, Harrison G, Popkin BM. The prevalence and trends of overweight, obesity and nutrition-related non-communicable diseases in the Arabian Gulf States. Obes Rev. 2011;12:1–13. doi: 10.1111/j.1467-789X.2010.00750.x. [DOI] [PubMed] [Google Scholar]
- 24.Municipality J. About Jeddah City. 2015. [[cited 2015 September]]. Available from: https://www.jeddah.gov.sa/english/JeddahCity/Geographical.php .
- 25.Al-Dossary SS, Sarkis PE, Hassan A, Ezz El Regal M, Fouda AE. Obesity in Saudi children: a dangerous reality. East Mediterr Health J. 2010;16:1003–1008. [PubMed] [Google Scholar]
- 26.Dean AG, Sullivan KM, Soe MM. OpenEpi: Open Source Epidemiologic Statistics for Public Health Version. [[Updated 2013/04/06, accessed 2016/11/06]]. Available from: www.OpenEpi.com .
- 27.National Institute of Dental Research. Diagnostic Criteria and Procedures. [[Updated 1991. Accessed 2015]]. Available from: ftp://ftp.cdc.gov/pub/Data/DOH/DiagnosticCriteria.pdf .
- 28.Al Herbish AS, El Mouzan MI, Al Salloum AA, Al Qureshi MM, Al Omar AA, Foster PJ, et al. Body mass index in Saudi Arabian children and adolescents: a national reference and comparison with international standards. Ann Saudi Med. 2009;29:342–347. doi: 10.4103/0256-4947.55162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Barlow SE, Expert C. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics. 2007;120(Suppl 4):S164–S192. doi: 10.1542/peds.2007-2329C. [DOI] [PubMed] [Google Scholar]
- 30.Bassali R, Waller JL, Gower B, Allison J, Davis CL. Utility of waist circumference percentile for risk evaluation in obese children. Int J Pediatr Obes. 2010;5:97–101. doi: 10.3109/17477160903111722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lobstein T, Baur L, Uauy R, TaskForce IIO. Obesity in children and young people: a crisis in public health. Obes Rev. 2004;5(Suppl 1):4–104. doi: 10.1111/j.1467-789X.2004.00133.x. [DOI] [PubMed] [Google Scholar]
- 32.Reilly D, Boyle CA, Craig DC. Obesity and dentistry: a growing problem. Br Dent J. 2009;207:171–175. doi: 10.1038/sj.bdj.2009.717. [DOI] [PubMed] [Google Scholar]
- 33.DeNicola E, Aburizaiza OS, Siddique A, Khwaja H, Carpenter DO. Obesity and public health in the Kingdom of Saudi Arabia. Rev Environ Health. 2015;30:191–205. doi: 10.1515/reveh-2015-0008. [DOI] [PubMed] [Google Scholar]
- 34.Abalkhail B. Overweight and obesity among Saudi Arabian children and adolescents between 1994 and 2000. East Mediterr Health J. 2002;8:470–479. [PubMed] [Google Scholar]
- 35.Al-Hazzaa HM, Musaiger AO, Abahussain NA, Al-Sobayel HI, Qahwaji DM. Lifestyle correlates of self-reported sleep duration among Saudi adolescents: a multicentre school-based cross-sectional study. Child Care Health Dev. 2014;40:533–542. doi: 10.1111/cch.12051. [DOI] [PubMed] [Google Scholar]
- 36.NM AQ. Obesity among Saudi Female University Students: Dietary Habits and Health Behaviors. J Egypt Public Health Assoc. 2010;85:45–59. [PubMed] [Google Scholar]
- 37.Collison KS, Zaidi MZ, Subhani SN, Al-Rubeaan K, Shoukri M, Al-Mohanna FA. Sugar-sweetened carbonated beverage consumption correlates with BMI, waist circumference, and poor dietary choices in school children. BMC Public Health. 2010;10:234. doi: 10.1186/1471-2458-10-234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Ogden CL, Carroll MD, Fryar CD, Flegal KM. Prevalence of Obesity Among Adults and Youth: United States 2011-2014. NCHS Data Brief. 2015;(219):1–8. [PubMed] [Google Scholar]
- 39.Mahfouz AA, Shatoor AS, Khan MY, Daffalla AA, Mostafa OA, Hassanein MA. Nutrition, physical activity, and gender risks for adolescent obesity in Southwestern Saudi Arabia. Saudi J Gastroenterol. 2011;17:318–322. doi: 10.4103/1319-3767.84486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Borraccino A, Lemma P, Iannotti RJ, Zambon A, Dalmasso P, Lazzeri G, et al. Socioeconomic effects on meeting physical activity guidelines: comparisons among 32 countries. Med Sci Sports Exerc. 2009;41:749–756. doi: 10.1249/MSS.0b013e3181917722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Mwaikambo SA, Leyna GH, Killewo J, Simba A, Puoane T. Why are primary school children overweight and obese? A cross sectional study undertaken in Kinondoni district, Dar-es-salaam. BMC Public Health. 2015;15:1269. doi: 10.1186/s12889-015-2598-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Patnaik L, Pattanaik S, Sahu T, Rao EV. Overweight and Obesity among Adolescents, A Comparative Study Between Government and Private Schools. Indian Pediatr. 2015;52:779–781. doi: 10.1007/s13312-015-0716-9. [DOI] [PubMed] [Google Scholar]
- 43.Jagadesan S, Harish R, Miranda P, Unnikrishnan R, Anjana RM, Mohan V. Prevalence of overweight and obesity among school children and adolescents in Chennai. Indian Pediatr. 2014;51:544–549. doi: 10.1007/s13312-014-0444-6. [DOI] [PubMed] [Google Scholar]
- 44.Lobstein T, Frelut ML. Prevalence of overweight among children in Europe. Obes Rev. 2003;4:195–200. doi: 10.1046/j.1467-789x.2003.00116.x. [DOI] [PubMed] [Google Scholar]
- 45.Magnusson MB, Sjoberg A, Kjellgren KI, Lissner L. Childhood obesity and prevention in different socio-economic contexts. Prev Med. 2011;53:402–407. doi: 10.1016/j.ypmed.2011.09.019. [DOI] [PubMed] [Google Scholar]
- 46.Marshall TA, Eichenberger-Gilmore JM, Broffitt BA, Warren JJ, Levy SM. Dental caries and childhood obesity: roles of diet and socioeconomic status. Community Dent Oral Epidemiol. 2007;35:449–458. doi: 10.1111/j.1600-0528.2006.00353.x. [DOI] [PubMed] [Google Scholar]
- 47.Observation NO. Obesity and Socioeconomic status. [[Updated 2010]]. Available from: http://www.noo.org.uk/uploads/doc/vid_7929_Adult.Socioeco Data Briefing October.2010.pdf .
- 48.Dake FA, Tawiah EO, Badasu DM. Sociodemographic correlates of obesity among Ghanaian women. Public Health Nutr. 2011;14:1285–1291. doi: 10.1017/S1368980010002879. [DOI] [PubMed] [Google Scholar]
- 49.Werner SL, Phillips C, Koroluk LD. Association between childhood obesity and dental caries. Pediatr Dent. 2012;34:23–27. [PubMed] [Google Scholar]
- 50.Tang RS, Huang MC, Huang ST. Relationship between dental caries status and anemia in children with severe early childhood caries. Kaohsiung J Med Sci. 2013;29:330–336. doi: 10.1016/j.kjms.2012.10.003. [DOI] [PubMed] [Google Scholar]
- 51.Stephensen CB. Burden of infection on growth failure. J Nutr. 1999;129(2S Suppl):534S–538S. doi: 10.1093/jn/129.2.534S. [DOI] [PubMed] [Google Scholar]
- 52.American Academy of Pediatric Dentistry. Policy on vending machines in schools. [[Updated 2009]]. Available from: http://www.aapd.org/media/Policies_Guidelines/P_VendingMachines.pdf .
- 53.Willershausen B, Haas G, Krummenauer F, Hohenfellner K. Relationship between high weight and caries frequency in German elementary school children. Eur J Med Res. 2004;9:400–404. [PubMed] [Google Scholar]
- 54.Mojarad F, Maybodi MH. Association between dental caries and body mass index among hamedan elementary school children in 2009. J Dent (Tehran) 2011;8:170–177. [PMC free article] [PubMed] [Google Scholar]