

Abstract
Objectives:
To check the amount of cellular damage caused by serial transfusions of blood in thalassemia patients.
Methods:
A cross-sectional study was conducted in the University of Lahore, Lahore, Pakistan between August 2012 and December 2012. A total of 43 thalassemia patients underwent at least 10 blood transfusions. Comprehensive biochemical analysis of blood was performed to record the levels of creatinine, urea, uric acid, albumin, liver function tests, malondialdehyde (MDA), and ferritin.
Results:
Serum creatinine (0.732±0.23mg/dl) and uric acid (6.7±0.94mg/dl, p<0.05) were significantly higher in patient groups as compared with the control. Ferritin levels were significantly higher in patients as compared with the control (3103.9±1747.4, p<0.05). Hemoglobin levels were observed in controls 14±1.3g/dl and in patients 7.1±1.03g/dl. No clear relationship exists between age and hematological parameters of thalassemic patients. Serum ferritin level is positively related with serum alanine transaminase, aspartate aminotransferase, and alkaline phosphatase and MDA (p<0.05).
Conclusion:
Serum MDA and serum ferritin of patients (r=0.593, p<0.05) reflects that both are crucial parameters estimating the cellular damage in patients suffering from thalassemia.
Thalassemia is among the most common genetic disorders worldwide. Thalassemia patients require blood transfusion on regular basis for their treatment. Patients develop iron overload as a result of excessive number of blood transfusion. 1mg of iron overload has to be borne by the body for each 1ml of red blood cells.1,2 Excess iron gets accumulated in different organs of the body namely; liver, kidney, pancreas, and heart.3 For the conversion of molecular oxygen to highly reactive radical species by Fenton Chemistry iron ions are required, which are not available normally. Iron deposits can exceed the storage and detoxification capacity of ferritin. Consequently, this free iron begins to accumulate in the blood and tissues. Very injurious compounds such as hydroxyl radical are formed as a result of free iron reactions. Patients suffering from beta thalassemia encounter increased levels of lipid peroxidation (LPO) products like malondialdehyde (MDA).4 Moreover, when there is an increase in LPO due to oxidative stress, it results in decreased antioxidative substances.5,6 Oxidative stress is a natural mechanism that happens in biological system by production of free radicals that interact chemically with other biological molecules, and damage to genetic material, membranes, and proteins leading to oxidative injury. On contrary, as natural defense mechanism biological system produces antioxidants to cope with free radicals/oxidants. Two important essential components of antioxidant defense mechanism of red blood cell are glutathione and its redox enzyme system.7
Methods
Study design and sample collection
Cross-sectional study design was selected and implicated on the samples. Samples were collected from Sundas Foundation of Thalassemia, Lahore, Pakistan. Detailed physical examination was performed and all the available blood tests reports were taken. A total of 43 thalassemia patients that satisfied the inclusion criteria were included in the study and compared with 8 healthy control individuals with same gender, age, and body mass index (BMI). Informed written consent was taken from all the patients and controls participating in the study according to the Helsinki declaration. The study was also approved by the ethical committee of the University of Lahore, Lahore, Pakistan. The study was performed between August 2012 and December 2012.
Inclusion criteria
Blood was taken from patients who had undergone with at least 10 blood transfusions.
Exclusion criteria
The patients who received less than 10 blood transfusions, or with other health problems were excluded from the study.
Biochemical analysis
All the biochemical tests were performed at the Biochemistry and Physiology of Stress Tolerance Lab, Institute of Molecular biology and Biotechnology (IMBB), The University of Lahore, Pakistan. Serum levels of creatinine (Cr), urea (U), uric acid (UA), and albumin were measured by spectrophotometer by using commercial Redox kits. Liver function tests (LFT’s) including serum alanine transaminase (ALT), aspartate aminotransferase (AST), and alkaline phosphatase (ALP) were also measured by using commercial Redox kits. Serum level of MDA was measured by standard method.6 Enzyme linked colorimetric immunoassay was used for serum ferritin evaluation.
Statistical analysis
The data is represented as Mean±SD and determined by the Independent T-test and Mann-Whitney Test and correlations (Spearman) between patients of thalassemia and control individuals using the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, USA) version 17. The significance difference was taken as p<0.05.
Results
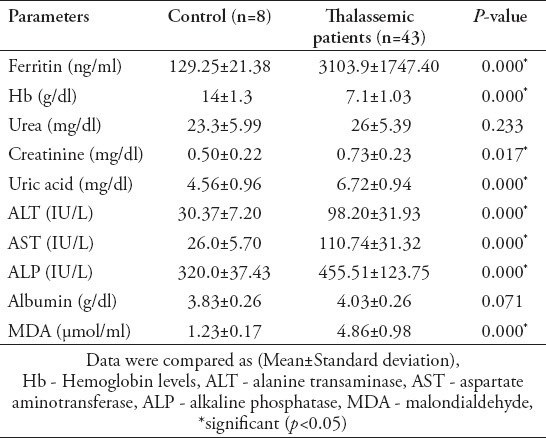
The results of the study shows that serum urea and serum albumin were not differ statistically between patients and controls (p>0.05) (Table 1). Serum creatinine (0.732±0.23mg/dl) and uric acid (6.7±0.94mg/dl, p<0.05) are significantly higher in patient groups and as compared with control. Ferritin levels are significantly higher in patients as compared with control (3103.9±1747.4, p<0.05). Hemoglobin levels (Hb) in controls are 14±1.3g/dl and patients are 7.1±1.03g/dl (Table 1).
Table 1.
Circulating biochemical and stress markers between control and thalassemics
Discussion
Patients suffering from b-thalassemia major (b-TM) have to face another problem referred as iron overload/hemochromatosis due to excessive blood transfusion, and it is generally called second disease.8 Ferritin is an intracellular protein that stores as well as release iron in a controlled fashion as per requirement of biological system. However, ferritin is evaluated in serum as indirect measurement of iron deficiency and/or iron overload. Single measure, in case of b-thalassemia, is insufficient and unreliable for iron levels. As a novel approach, magnetic resonance imaging (MRI) could be employed for measuring iron contents in the body because MRI is considered as more sensitive as compared with routine ferritin evaluation from serum.9 Low levels of ferritin in serum reflect lesser risk for various clinical problems as well as longer survival for patients with thalassemia.10 Long lasting anemia, iron overload, toxicity of deferoxamine (an iron-chelating agent) and chronic hypoxia lead to renal dysfunctions in patients with b-TM.1
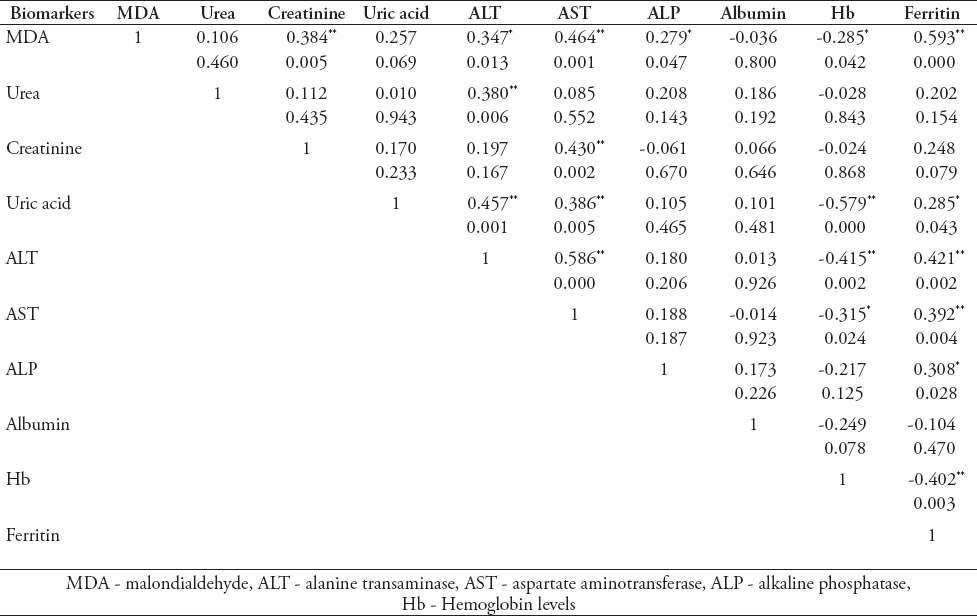
In the present study, high serum creatinine was observed only in 12% of the patients, which were in the age group of 15-20 years and those in the chelation therapy for more than 15 years. In the present study, the mean serum uric acid levels were significantly higher in the patient (6.7±0.94mg/dl) group than in the controls (4.5±0.96mg/dl). In addition to rapid erythrocyte turnover, proximal tubular damage may lead to hyperuricemia in these patients, because the filtered uric acid can be reabsorbed from the proximal tubules. Serum alanine transaminase, aspartate aminotransferase, and alkaline phosphatase abnormality in results suggested that patients developed chronic liver malfunctioning. The correlation between ALT activity and serum ferritin (r=.421; p=.002) level refers to hepatocellular injury (Table 2). Chronic iron overload in hepatocytes leads to cirrhotic outcomes as well as hepatic carcinoma that is referred as hepatoma. Hence, rate of mortality is associated with hepatocellular carcinoma (HCC), diabetes, cardiomyopathy, and liver dysfunctioning.11 Moreover, increasing serum ferritin level seems to be associated with liver cirrhosis.12 There is a strong association between serum ferritin and MDA, it is proved that both these parameters are important to estimate cellular damage in thalassemia. Moreover, enhanced plasma LPO marker MDA has also been observed previously in patients suffering from thalassemia.7,13,14 No clear relationship exists between age and hematological parameters of thalassemic patients. Serum ferritin level is positively related with serum ALT, AST, ALP, and MDA (p<0.05). Serum MDA and serum ferritin of patients (r=.593, p<0.05) reflects that both are crucial parameters estimating the cellular damage in patients suffering from thalassemia (Table 2). We used limited sample size due to financial constraints and the limitation of patients suffering from thalassemia that have undergone at least 10 blood transfusions and does not show any other health problems. Further research should include more patients with less than 10 blood transfusions.
Table 2.
Correlation matrix circulating biomarkers in beta thalassemia patients.
In conclusion, patients with thalassemia show various clinical signs and symptoms that seem to be unavoidable due to the regular transfusion of blood and its associated physiological as well as pathological outcomes. Having insights into various clinical aspects of thalassemia it can be concluded that antioxidative therapy may be more helpful for long survival of patients with thalassemia with conventional iron chelating therapy.
Acknowledgment
The authors gratefully acknowledge the Deanship of Scientific Research, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia for the financial and technical support.
Footnotes
References
- 1.Ali BA, Mahmoud AM. Frequency of glomerular dysfunction in children with beta thalassaemia major. Sultan Qaboos Univ Med J. 2014;14:88–94. doi: 10.12816/0003341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Raghupathy R, Manwani D, Little JA. Iron overload in sickle cell disease. Adv Hematol. 2010;2010:272940. doi: 10.1155/2010/272940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kohgo Y, Ikuta K, Ohtake T, Torimoto Y, Kato J. Body iron metabolism and pathophysiology of iron overload. Int J Hematol. 2008;88:7–15. doi: 10.1007/s12185-008-0120-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pavlova LE, Savov VM, Petkov HG, Charova IP. Oxidative stress in patients with beta-thalassemia major. Prilozi. 2007;28:145–154. [PubMed] [Google Scholar]
- 5.Malik A, Qureshi MS, Manan A, Saleem S, Munir M, Fatima A, et al. assessment of oxidative stress in hepatitis C patients receiving interferon therapy. Pakistan Journal of Medicine and Dentistry. 2013;2:10–15. [Google Scholar]
- 6.Shazia Q, Mohammad ZH, Rahman T, Shekhar HU. Correlation of oxidative stress with serum trace element levels and antioxidant enzyme status in beta thalassemia major patients: A review of the literature. Anemia. 2012:1–7. doi: 10.1155/2012/270923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Walter PB, Fung E, Killilea DW, Jiang Q, Hudes M, Madden J. Oxidative stress and inflammation in iron-overloaded patients with beta thalassemia or sickle cell disease. Br J Haematol. 2006;135:254–263. doi: 10.1111/j.1365-2141.2006.06277.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kremastinos DT, Farmakis D. Iron overload cardiomyopathy in clinical practice. Circulation. 2011;124:2253–2263. doi: 10.1161/CIRCULATIONAHA.111.050773. [DOI] [PubMed] [Google Scholar]
- 9.Eghbali A, Taherahmadi H, Shahbazi M, Bagheri B, Ebrahimi L. Association between serum ferritin level, cardiac and hepatic T2-star MRI in patients with major b-thalassemia. Iran J Ped Hematol Oncol. 2014;4:17–21. [PMC free article] [PubMed] [Google Scholar]
- 10.Borgna-Pignatti C, Vergine G, Lombardo T, Cappellini MD, Cianciulli P, et al. Hepatocellular carcinoma in the thalassemia syndromes. Br J Haematol. 2004;124:114–117. doi: 10.1046/j.1365-2141.2003.04732.x. [DOI] [PubMed] [Google Scholar]
- 11.Rasool M, Rashid S, Arooj M, Ansari SA, Khan KM, Malik A, et al. New possibilities in hepatocellular carcinoma treatment. Anticancer Res. 2014;34:1563–1571. [PubMed] [Google Scholar]
- 12.Mary AK, Jonathan AS, Lan GC, Suzy VT, Frank MT. Ferritin for the clinician. Blood Rev. 2009;23:195–104. [Google Scholar]
- 13.Chakraborty I, Mitra S, Gachhui R, Kar M. Non-haem Iron-mediated Oxidative Stress in Haemoglobin E Beta-thalassaemia. Ann Acad Med Singapore. 2010;39:13–16. [PubMed] [Google Scholar]
- 14.Laksmitawati DR, Handayani S, Udyaningsih-Freisleben SK, Kurniati V, Adhiyanto C, Hidayat J. Iron status and oxidative stress in beta-thalassemia patients in Jakarta. Biofactors. 2003;19:53–62. doi: 10.1002/biof.5520190107. [DOI] [PubMed] [Google Scholar]
- 15.Ohkawa H, Ohishi N, Yagi K. Assay for lipid peroxides in animal tissues by thiobarbituric acid reaction. Anal Biochem. 1979;95:351–358. doi: 10.1016/0003-2697(79)90738-3. [DOI] [PubMed] [Google Scholar]