

Abstract
Background:
There are approximately 2.8 million youth football players between the ages of 7 and 14 years in the United States. Rates of injury in this population are poorly described. Recent studies have reported injury rates between 2.3% and 30.4% per season and between 8.5 and 43 per 1000 exposures.
Hypothesis:
Youth flag football has a lower injury rate than youth tackle football. The concussion rates in flag football are lower than in tackle football.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Three large youth (grades 2-7) football leagues with a total of 3794 players were enrolled. Research personnel partnered with the leagues to provide electronic attendance and injury reporting systems. Researchers had access to deidentified player data and injury information. Injury rates for both the tackle and flag leagues were calculated and compared using Poisson regression with a log link. The probability an injury was severe and an injury resulted in a concussion were modeled using logistic regression. For these 2 responses, best subset model selection was performed, and the model with the minimum Akaike information criterion value was chosen as best. Kaplan-Meier curves were examined to compare time loss due to injury for various subgroups of the population. Finally, time loss was modeled using Cox proportional hazards regression models.
Results:
A total of 46,416 exposures and 128 injuries were reported. The mean age at injury was 10.64 years. The hazard ratio for tackle football (compared with flag football) was 0.45 (95% CI, 0.25-0.80; P = .0065). The rate of severe injuries per exposure for tackle football was 1.1 (95% CI, 0.33-3.4; P = .93) times that of the flag league. The rate for concussions in tackle football per exposure was 0.51 (95% CI, 0.16-1.7; P = .27) times that of the flag league.
Conclusion:
Injury is more likely to occur in youth flag football than in youth tackle football. Severe injuries and concussions were not significantly different between leagues. Concussion was more likely to occur during games than during practice. Players in the sixth or seventh grade were more likely to suffer a concussion than were younger players.
Keywords: youth football, flag football, concussion, youth sports
Recently, the safety of youth football has been brought into question in the popular media.2 Flag football has been proposed to be a safer alternative to tackle football. However, injury rates in youth football remain poorly described. Previous studies on youth football injuries have been conducted on small samples (n < 1000 athletes) or suffered from methodological limitations. In order to better understand the risk of injury in youth football, there is a need for a larger study to determine the types of injuries suffered by youth football players, injury incidence, the risk factors associated with these injuries, and whether flag football is indeed a safer alternative to tackle football for young players. A recent American Academy of Pediatrics Policy Statement on tackling in youth football recommended nontackling leagues should be expanded.4 We hypothesize that youth flag football has a lower injury rate than youth tackle football.
In the United States, approximately 2.8 million youth between the ages of 6 and 14 years participate in youth football each year.2 Sport-related injuries are the leading cause of injury among children and adolescents.3 Previous studies of youth football have suffered from inaccurate estimates of athletic exposure and varied definitions of injury. This is reflected in the large variability in reported injury epidemiology between studies. Recent studies report injury rates between 2.3% and 38.2% per season.2,6–8,10,12,18–22 Games resulted in 8.5 to 43 injuries per 1000 exposures, and practices had 1 to 13.5 injuries per 1000 exposures. Overall for games and practices combined, these studies showed 2 to 17.8 injuries per 1000 exposures.6,12–16,20,21 Despite these variations, it is likely that the risk of injury is higher in youth football than in other popular youth sports, including basketball, soccer, wrestling, and gymnastics.16,22
The most commonly reported injures in youth football are fractures, sprains, strains, and contusions. The rates of fracture have been the most consistent between studies, with 27% to 35% of reported injuries being fractures. Injuries with more subjective diagnostic criteria, such as sprains, strains, and contusions, have suffered from more variability in reporting, with 9% to 69% of reported injuries being sprains, strains, and contusions.2,8,10,14,15,18–21 Players in grades 7 and 8 have almost twice the injury risk when compared with players in grades 4, 5, and 6.12 In studies in which athlete-exposures were measured, the injury risk in older and more experienced athletes could be attributed to the more experienced players’ increased playing time. Interestingly, youth football players with more advanced sexual maturity ratings have been shown to have a higher risk for injury.10,11,17
Sport-related concussion has gained widespread attention in the popular media and scientific literature. Previous studies of youth football have identified remarkably few concussions compared with other levels of play. However, Kontos et al9 recently reported on a cohort of 468 youth football players with rates of concussion comparable to high school and collegiate football players. USA Football reports a concussion incidence in youth football of nearly 4%.2 Additionally, Daniel et al5 recently reported on accelerometer-instrumented helmet-based measurements of collisions during youth football. Youth football players experienced fewer impacts per season. On average, these collisions were less forceful than those in high school and collegiate athletes. However, the top 5% of reported collisions were almost as forceful as the highest-force collisions seen in high school and collegiate players. Most of the highest-force impacts occurred during practice rather than during a game. This is in opposition to previous epidemiologic studies, which have shown up to a 10-fold greater risk of concussion in youth football games when compared with practice.
We hypothesize that youth flag football has a lower injury rate than youth tackle football. We also hypothesize that concussion rates in flag football will be lower than in tackle football.
Methods
Participants
Three youth football leagues (2 tackle leagues and 1 flag league) with a total of 3794 players (3525 tackle football players and 269 flag football players) participated in this prospective cohort study. Tackle league A contained 43 teams, and all 43 teams reported at least 1 data point. Tackle league B contained 124 teams, and only 72 teams reported at least 1 data point. The flag football league contained 20 teams, and 18 teams reported at least 1 data point. Leagues were enrolled and provided with technical assistance. Individual athletes were not enrolled in the study. Specifically, the research team provided the leagues with an online database to monitor player attendance at practices and games. The database also provided leagues with an injury reporting system for tracking injuries and loss of playing time according to their league’s policies and procedures. Deidentified data elements were extracted from the online database and used for this analysis.
Tackle and flag football differ in their equipment and in how they determine the end of a down. In tackle football, players are allowed to wear pads and helmets, but in flag football, pads and helmets are not allowed and players must wear a belt around their waist with 3 flags. In tackle football, the end of a down is defined when the ball carrier’s forward progress is halted and not resumed, the ball carrier is forced to go out of bounds, or when a body part other than hands or feet touch the ground. In flag football, the end of a down is defined when a player runs out of bounds or when 1 of 3 flags is pulled off a belt worn around the waist.
Measures and Procedures
Teams within each league documented player attendance at practices and games and reported any injury that resulted in the loss of playing time following their league’s policies and procedures. These records contained personally identifiable information, but no research team member was able to access this personal information. Coaches input their practice and competition attendance into an online database provided by the research team. All injury information was deidentified and reported to the research team through the online database. Participation was measured with the date of the game or practice and attendance and participation status. The date of each football game and practice along with the number of players who participated was recorded. These metrics were used to determine the total number of exposures. An exposure was defined as a single game or practice where a player had the potential to be injured (eg, a social gathering where football was not practiced or played would not count as a practice). Deidentified exposure information was available to the research team via the online database. The research team’s deidentified database did assign injured players a number in case the player was injured multiple times. The total number of players per league was provided to the research team by the leagues based on their registrations at the beginning of the season.
All injuries that resulted in loss of playing time were included. The injury report contained information that could be used to identify the injured player for the league’s use. However, the online database used by the research team excluded name, emergency contact, date of birth, telephone number, and team. The leagues also had access to other information such as date of injury, type of play or drill, location of injury, and description of injury, which was not used by the research team. The deidentified injury information used by the research team included the following items: sex, age, grade, type of league (tackle vs flag), setting (game vs practice), position on the field (quarterback, running back, linebacker, etc), type of injury (contact, noncontact), number of days missed after injury, return to play at any point (yes, no), and diagnosis.
Teams were instructed to complete this form after every practice or competition. One person for each team was designated to input information into the database after each practice or game. This person could be a coach, volunteer parent, or team athletic trainer. The team designees were provided with a tutorial on how to complete the online form prior to the start of the season.
Data Analyses
Participation and injury report forms were used to calculate injury rates. For each injury that occurred, we abstracted the following variables: grade (dichotomized into second through fifth and sixth through seventh), league type (flag and tackle), setting (game or practice), team (defense or offense), position (lineman or nonlineman), and injury type (contact and noncontact injuries).
Grade was chosen instead of age because all the leagues were organized by grade in school and not by age. Nearly all injured players were age appropriate for their grade. Injured players were within 1 year of age except 1 injured fifth grader who was an extra year older than the remaining fifth graders (12 years old instead of 10-11 years old). Sex was not chosen as an analyzed variable because no female players were injured. Positions were dichotomized to lineman or nonlineman due to the limited number of injuries, which occurred at each position. Tight ends were considered nonlinemen. Contact injuries were defined as any injury sustained due to impact with another player, regardless of whether the injury occurred while playing flag or tackle football. An injury was considered noncontact if it occurred without an external force exhibited by another player, such as those experienced during a running drill. An injury was considered severe if it resulted in a concussion, fracture, or ligament tear. All other injuries were considered nonsevere. The leagues encouraged their teams to use the International Consensus Statement Guidelines for Sport-Related Concussion.13
Poisson regression with a log link was used to compare overall injury rates, concussion rates, and severe injury rates in the tackle and flag leagues. The model for each league type was log(μi) = log(Ei) + Li, where μi is the mean number of injuries for the given league type, Ei is the number of exposures, and Li is a league type–specific indicator. The numerator of the ratio estimates is the rate in the flag league and the denominator is the rate in the tackle league. The 95% CIs and corresponding P values were also calculated.
Multivariable logistic regression was employed to fit models for concussion status and whether an injury was severe. To determine which model was best in predicting both response variables of interest, all subsets of predictors were considered and the model with the smallest Akaike information criterion (AIC) value was used.1 Only the main effects were considered as possible predictors in this model selection procedure, but this assumption was verified by using the deviance statistic to assess whether any interaction terms were needed in the models. Demographic information was only available for players who sustained an injury. The analyses were conditioned such that an injury had occurred. For instance, we were able to model the probability that an injury was severe but we were unable to determine the probability of sustaining a severe injury.
The final analysis involved determining which predictors were important in characterizing the number of days until an injured player returned. Only 100 of the 128 injuries were used in these analyses due to either inconsistent coding of exposure data (19 players) or the player being injured on the final day of the season (9 players). Of the 100 injuries used, the player’s date of return was recorded in 83 instances. For the remaining 17 injuries, the player either did not return before the end of the season or the coach stopped reporting before the season ended. In these 17 instances, the variable’s value was considered to be censored, and we recorded the value of this variable to be the difference between the last day of recording and the date of injury. These censored data are taken into account in the time to event analysis.
For each predictor of interest, Kaplan-Meier curves were constructed displaying the probability a player’s injury would still cause the player to be unable to participate a given number of days after the injury occurred. Cox proportional hazards regression was used to fit models predicting the amount of time a player would lose to an injury. To determine which model was best in predicting a player’s time loss, we used forward and backward model selection techniques at significance levels of .05 and .10. The following were possible predictors in the final model: grade, league type, setting, team, position, injury type, injury severity, and concussion status. Note that only included main effects were included as possible predictors. Finally, for the predictors chosen in the final model, time-dependent covariates were tested to assess the validity of the proportional hazards assumption.
Results
All 3 leagues had a total of 46,416 exposures where an injury could have occurred. Of the 46,416 exposures, there were a total of 128 injuries, representing 121 different players. The players who were injured ranged from 8 to 13 years of age, with a mean age of 10.6 years and a median age of 11 years. The overall injury rate was 2.76 injuries per 1000 exposures. Of the 128 injuries, 65 were considered severe. Of the 65 severe injuries, 33 were classified as concussions. Table 1 presents the number of exposures, injuries, severe injuries, and concussions by league type.
TABLE 1.
Exposures and Injuries by League Type
| League Type | Exposures | Total Injuries | Severe Injuries | Concussions | Injuries per 1000 Exposures | Severe Injuries per 1000 Exposures | Concussions per 1000 Exposures |
|---|---|---|---|---|---|---|---|
| Tackle | 44,164 | 115 | 62 | 30 | 2.60 | 1.40 | 0.68 |
| Flag | 2,252 | 13 | 3 | 3 | 5.77 | 1.33 | 1.33 |
Of the 128 injuries, 54 happened to players on defense and 74 on offense. Of the 54 defensive injuries, 44 occurred in the tackle leagues and 10 in the flag league. Of the 74 offensive injuries, 71 happened in tackle leagues and 3 occurred in the flag league. Of the 128 injures, 37 happened to lineman and 91 to nonlineman. All 37 injuries to lineman happened in the tackle leagues. Of the 91 nonlineman injuries, 78 happened in tackle leagues and 13 were in the flag league.
Overall injury rates, severe injury rates, and concussion rates were compared between flag and tackle leagues. The results are shown in Table 2.
TABLE 2.
Comparison of Injury Rates Between League Types
| League Type | Response Variable | Ratio Estimate | 95% CI | P Value |
|---|---|---|---|---|
| Flag vs tackle | Injury rate | 2.217 | 1.249, 3.934 | .0065 |
| Flag vs tackle | Severe injury rate | 0.9489 | 0.2979, 3.0229 | .9293 |
| Flag vs tackle | Concussion rate | 1.961 | 0.5985, 6.4257 | .2660 |
Using both forward and backward model selection techniques, the best model for predicting whether an injury was severe included only league type as a predictor. The predicted probability that an injury is severe is presented in Table 3.
TABLE 3.
Estimated Probability an Injury is Severe by League Type
| League Type | Predicted Probability an Injury is Severe |
|---|---|
| Tackle | .540 |
| Flag | .231 |
The best model for predicting whether an injury produced a concussion included the predictors setting and grade. Note all concussions occurred on contact plays, so this predictor was excluded from analyses. The estimated probability an injury resulted in a concussion for each combination of grade and setting is presented in Table 4.
TABLE 4.
Estimated Probability an Injury Results in a Concussion by Setting and Grade
| Setting = Game | Setting = Practice | |
|---|---|---|
| Grade ≤ fifth | 0.254 | 0.129 |
| Grade ≥ sixth | 0.426 | 0.245 |
Kaplan-Meier curves displaying time loss for each predictor of interest were created and are displayed in Figures 1 through 4. Figure 1 compares the number of days a player from the tackle league sat out due to their injury versus a player in the flag league. Figure 2 shows the difference in the amount of time players who had severe injuries sat out versus players with minor injuries. Figure 3 splits the severe injuries from Figure 2 into severe nonconcussed injuries and severe concussion-related injuries. Figure 4 combines the minor injuries and severe nonconcussed injuries to compare concussion injuries to all nonconcussion-related injuries.
Figure 1.
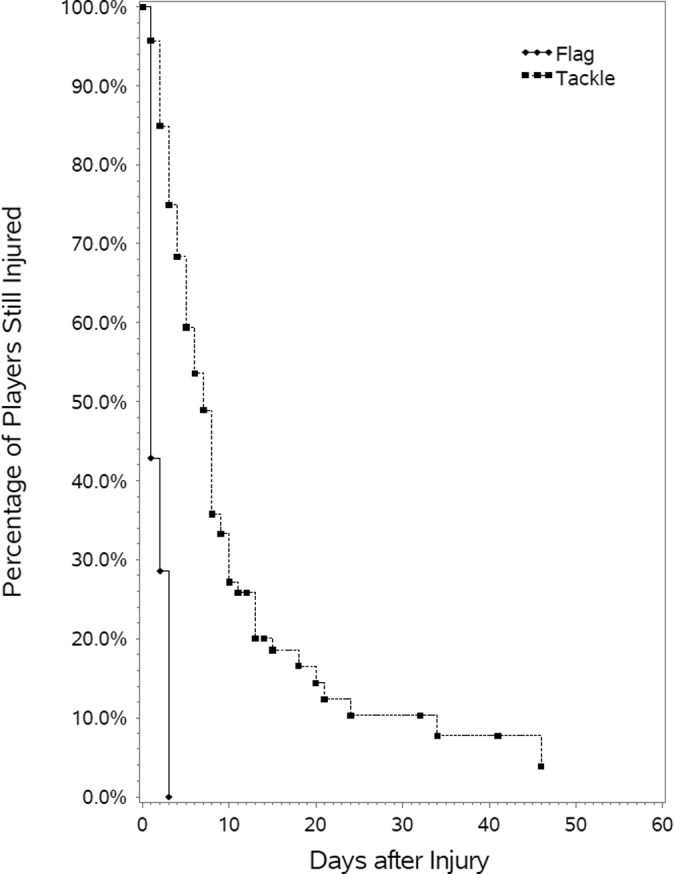
Kaplan-Meier curve stratified by league type.
Figure 2.
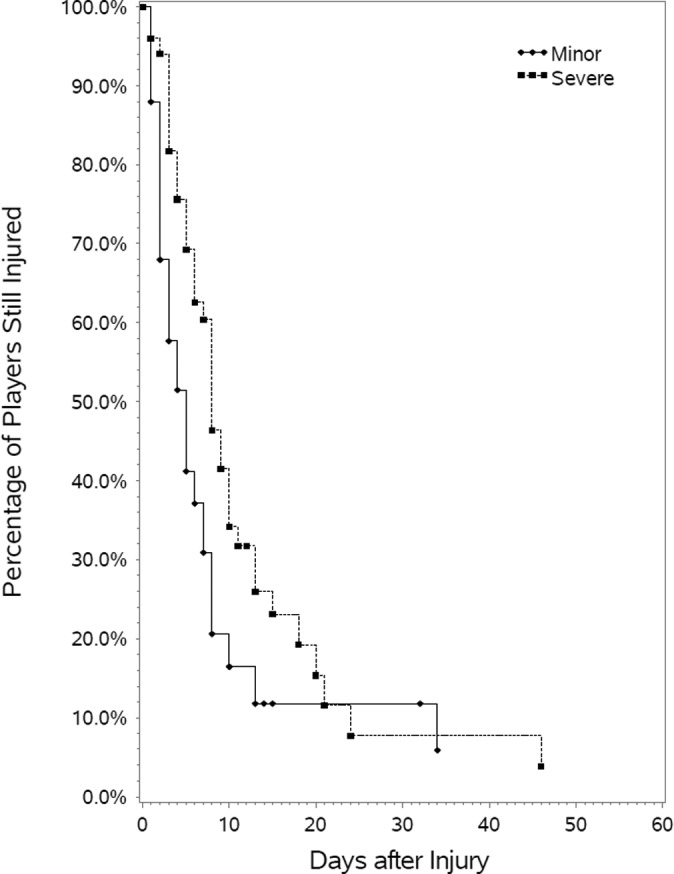
Kaplan-Meier curve stratified by injury severity.
Figure 3.
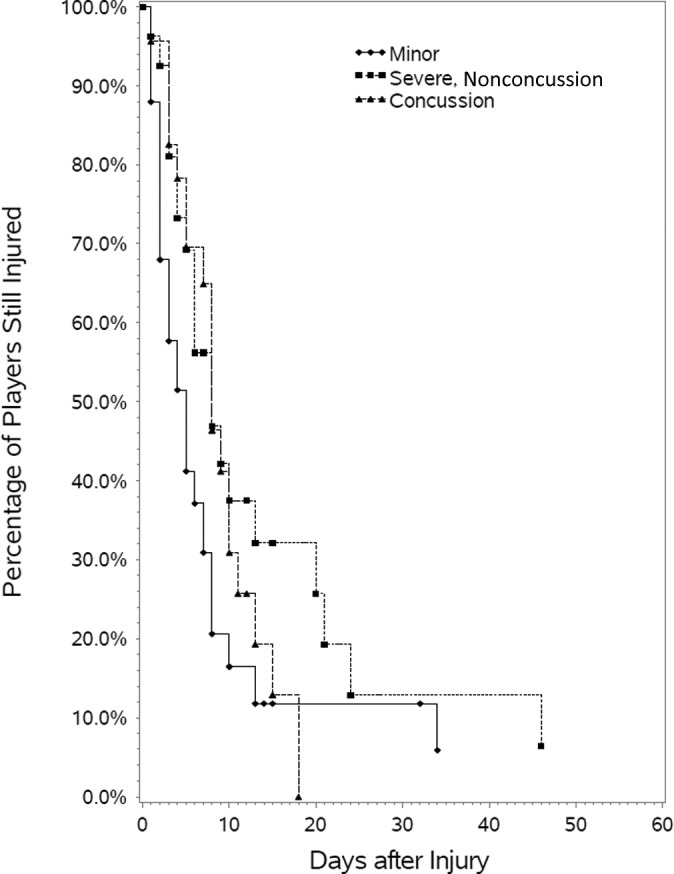
Kaplan-Meier curve stratified by injury severity and concussion status.
Figure 4.
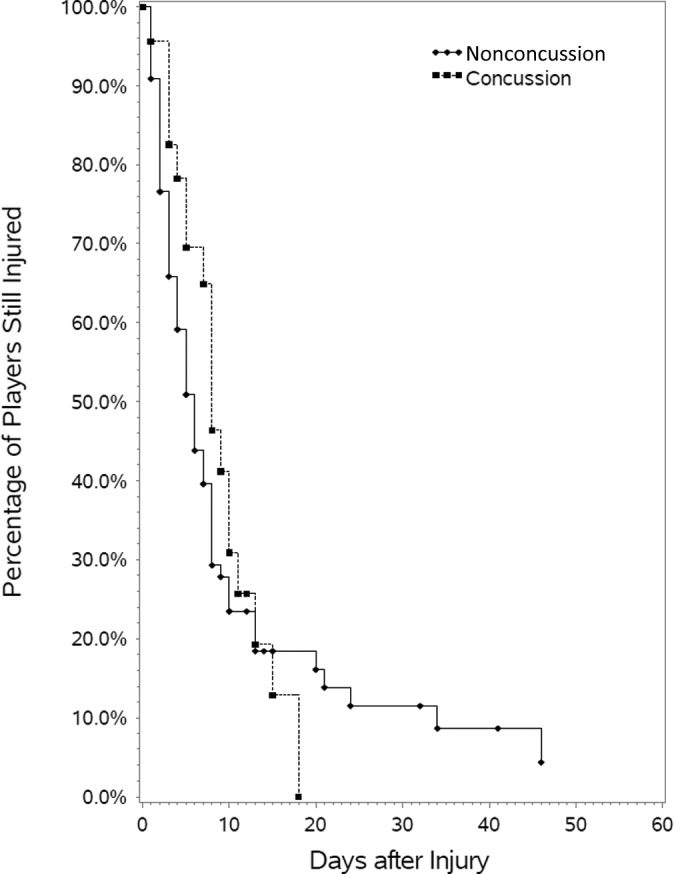
Kaplan-Meier curve stratified by concussion status.
The final analyses determined which predictors were important in characterizing how long a player’s injury forced the player to sit out. The best model for predicting how long a player’s injury caused the player to sit out included both league type and injury severity. Neither league type nor injury severity showed significant deviations from the proportional hazards assumption. Table 5 provides an estimate of the imminent probability of return ratio, the 95% CI for the imminent probability of return ratio, and a corresponding P value.
TABLE 5.
Inferential Results for Time Loss Analysis
| Predictor | Level of Predictor | Imminent Probability Ratio | 95% CI | P Value |
|---|---|---|---|---|
| League type | Flag vs tackle | 9.505 | 3.940, 22.930 | <.0001 |
| Injury severity | Minor vs severe | 1.610 | 1.037, 2.501 | .0339 |
Discussion
Our first objective was to determine whether flag football had lower injury rates than youth tackle football. The injury rate found in the youth flag league is significantly higher than the injury rate in youth tackle football (P = .0065). Therefore, we reject our initial hypothesis. The higher injury rate in flag football could be due to a number of factors. Flag football players do not wear protective equipment like tackle football players. There are differences in the mechanics of play. Tackle football has significant contact with blocking, but flag football involves players running and diving for flags. This may also represent an intrinsic difference between the participants in youth flag football and the participants in youth tackle football.
Injury rates measured similar to what had previously been reported. Other studies found overall injury rates per 1000 exposures ranged from 2 to 17.8 injuries per 1000 exposures.6,12–16,20,21 These studies were predominantly looking at youth tackle football. The 2.60 injuries per 1000 exposures described in this study is slightly lower than has been found in similar studies, but our study had more players and more exposures than other studies. There is no comparable literature that has evaluated injury rates in youth flag football.
In comparing the injuries in tackle and flag football, time to return to play after an injury was much longer in the tackle leagues than in the flag leagues. This presents a paradox in trying to determine which league type is “safer.” Tackle football players suffer fewer injuries, but the injuries that do occur result in more lost playing time. There are countless reasons why a player might sit out longer or shorter from an injury. However, there were no rules or other systematic reasons that would have affected this at the league level. Individual teams can even have different policies and procedures.
The imminent probability a player will return from an injury on any day (given he or she has not returned to play already) is 9.505 times higher for a player in the flag league than a player in the tackle league (P < .0001) (Table 5). That is, for a given practice or game, an injured player in the flag football league is almost 10 times as likely to return to play than a player in a tackle football league. The imminent probability a player will return from their injuries is 1.610 times higher for a player whose injuries are minor. These data serve as an internal control for our model because we expect players with minor injuries to return to play more quickly than players with a severe injuries.
Some research shows older players tend to have an increased injury rate.4,6–8,10,12,14–15,20,22 Not all studies agree with this assumption.18 The prominent age-related finding of this study was a conditional risk of concussion by grade and type of exposure for injured players (Table 4). For athletes in fifth grade or lower and athletes in sixth grade or higher, injuries sustained during games were almost twice as likely to be a concussion than injuries sustained during practice. Injuries were also more likely to be concussions in older athletes than in younger athletes. Because of the nature of the data collected, we are not concluding rates of concussion were higher in games or in older athletes but rather that among injured youth football players, being older and playing in a game increases the chances the injury is a concussion.
The second main objective was to compare the concussion rates of tackle football and flag football. There was a trend toward a higher concussion rate in the flag league than in the tackle leagues, but this result is based on only 3 concussions in the flag league and is not statistically significant. Interestingly, despite the fact that flag football is supposed to be a noncontact sport, all concussions occurred during contact with another player.
Concussions were also analyzed by looking at the time to return to play. Players with concussions and those with severe nonconcussed injuries had a similar proportion of players return to play within 10 days (Figure 3). However, all concussed players returned to play within 20 days, while not all of the severely injured nonconcussed players returned by 20 days. Severely injured players who were not concussed tended to be less likely to quickly return from their injuries than players who had concussions.
For the first 15 days after an injury occurs, a non-concussed player is more likely to return from an injury than a concussed player, but after that time, a concussed player is more likely to return than a nonconcussed player (Figure 4). This is logical as the majority of players returning the first 15 days would be the nonconcussed players with minor injuries. After 15 days, most of the remaining injuries would be in nonconcussed patients with severe injuries (like a ligament tear or a fracture) that needed much more time to heal before returning to play.
Limitations
The biggest limitation of this study is that player-specific variables were only recorded if the player was injured. This limits the degree to which injury types and severity can be described by demographic information such as age, sex, position, and so on. For this reason, analysis of concussion by grade and setting (Table 4) is limited to the condition of injury. That is, only the conditional probability of an injury being a concussion can be reported given that they are injured, in a specific age range, and participating in a specific setting. For example, the specific rates of concussion among fifth grade linemen during practice cannot be reported because the denominator is unknown (the pool of athletes who fit this description and can be injured at a given event). Only the total number of athletes participating is known and whether they are in the tackle or flag league.
A second limitation is that this study is dependent on semivoluntary attendance and injury reporting. Each league requires their coaches to collect attendance and report any injuries to the league. Our partnership with the leagues has made the process easier for the team personnel than it was before we provided electronic infrastructure, but there may still be variability between coaches and team personnel in attendance and injury reporting. Also, “nonmedical” personnel reported the injuries based on who was designated by the team. Some teams had athletic trainers who filled out the injury reports, but other coaches and staff did not have a way of confirming the diagnosis with physicians or athletic trainers.
Another limitation is players and their parents self-select what league they participate in. Parents of flag football players may be concerned about possible injuries and selected flag football based on personal safety bias. If that is the case, they may be more inclined to report injuries when others may not.
Finally, the number of injuries seen in the flag football league was relatively small, and the number of participants in the flag league was much smaller than the number of participants in the tackle leagues. For these reasons, the comparisons made between leagues are somewhat limited.
Conclusion
Rates of injury in youth football are relatively low. Youth flag football has a higher injury rate than tackle football. A significantly different rate of severe injury or concussion between tackle and flag football was not identified, but players did return to play more slowly after an injury in the tackle leagues than they did in the flag league. Furthermore, we cannot conclude that youth flag football is a safer alternative to youth tackle football. The higher injury rate in flag football needs to be considered when determining the relative safety of flag football and tackle football. Future safety analyses should include looking at injury rates, severity, type of injury, lost time, and future consequences of injury.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was waived by the University of Iowa Institutional Review Board.
References
- 1. Akaike H. A new look at the statistical model identification. IEEE Trans Automat Control. 1974;19:716–723. [Google Scholar]
- 2. Alic S. USA Football releases preliminary data in study examining youth football player health and safety. 2013. http://usafootball.com/health-safety/usafootball-releases-preliminary-date-study-examining-youth-football-playerhealth-an. Accessed November 23, 2013.
- 3. Bijur PE, Trumble A, Harel Y, Overpeck MD, Jones D, Scheidt PC. Sports and recreation injuries in US children and adolescents. Arch Pediatr Adolesc Med. 1995;149:1009–1016. [DOI] [PubMed] [Google Scholar]
- 4. Council on Sports Medicine and Fitness. Tackling in youth football. Pediatrics. 2015;136:e1419–e1430. [DOI] [PubMed] [Google Scholar]
- 5. Daniel RW, Rowson S, Duma SM. Head impact exposure in youth football. Ann Biomed Eng. 2012;40:976–981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Dompier TP, Powell JW, Barron MJ, Moore MT. Time-loss and non-time-loss injuries in youth football players. J Athl Train. 2007;42:395–402. [PMC free article] [PubMed] [Google Scholar]
- 7. Ellison L, Mackenzie S. Sports injuries in the database of the Canadian hospitals injury reporting and prevention program—an overview. Chronic Dis Can. 1993;14:96–104. [Google Scholar]
- 8. Goldberg B, Rosenthal PP, Robertson LS, Nicholas JA. Injuries in youth football. Pediatrics. 1988;81:255–261. [PubMed] [Google Scholar]
- 9. Kontos AP, Elbin RJ, Fazio-Sumrock VC, et al. Incidence of sports-related concussion among youth football players aged 8-12 years. J Pediatr. 2013;163:717–720. [DOI] [PubMed] [Google Scholar]
- 10. Linder MM, Townsend DJ, Jones JC, Balkcom IL, Anthony CR. Incidence of adolescent injuries in junior high school football and its relationship to sexual maturity. Clin J Sport Med. 1995;5:167–170. [DOI] [PubMed] [Google Scholar]
- 11. Malina RM, Dompier TP, Powell JW, Barron MJ, Moore MT. Validation of a noninvasive maturity estimate relative to skeletal age in youth football players. Clin J Sport Med. 2007;17:362–368. [DOI] [PubMed] [Google Scholar]
- 12. Malina RM, Morano PJ, Barron M, Miller SJ, Cumming SP, Kontos AP. Incidence and player risk factors for injury in youth football. Clin J Sport Med. 2006;16:214–222. [DOI] [PubMed] [Google Scholar]
- 13. McCrory P, Meeuwisse W, Aubry M, et al. Consensus statement on concussion in sport—the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Clin J Sport Med. 2013;23:89–117. [DOI] [PubMed] [Google Scholar]
- 14. Mello MJ, Myers R, Christian JB, Palmisciano L, Linakis JG. Injuries in youth football: national emergency department visits during 2001-2005 for young and adolescent players. Acad Emerg Med. 2009;16:243–248. [DOI] [PubMed] [Google Scholar]
- 15. Nation AD, Nelson NG, Yard EE, Comstock RD, McKenzie LB. Football-related injuries among 6- to 17-year-olds treated in US emergency departments, 1990-2007. Clin Pediatr (Phila). 2011;50:200–207. [DOI] [PubMed] [Google Scholar]
- 16. Radelet MA, Lephart SM, Rubinstein EN, Myers JB. Survey of the injury rate for children in community sports. Pediatrics. 2002;110:e28. [DOI] [PubMed] [Google Scholar]
- 17. Rochelle R, Kelliher M, Thorton R. Relationship of maturation age to incidence of injury in tackle football. Res Q Exerc Sport. 1961;32:78–82. [Google Scholar]
- 18. Roser LA, Clawson DK. Football injuries in the very young athlete. Clin Orthop Relat Res. 1970;69:219–223. [PubMed] [Google Scholar]
- 19. Silverstein B. Injuries in youth league football. Phys Sportsmed. 1979;7:105–111. [DOI] [PubMed] [Google Scholar]
- 20. Stuart MJ, Morrey MA, Smith AM, Meis JK, Ortiguera CJ. Injuries in youth football: a prospective observational cohort analysis among players aged 9 to 13 years. Mayo Clin Proc. 2002;77:317–322. [DOI] [PubMed] [Google Scholar]
- 21. Turbeville SD, Cowan LD, Asal NR, Owen WL, Anderson MA. Risk factors for injury in middle school football players. Am J Sports Med. 2003;31:276–281. [DOI] [PubMed] [Google Scholar]
- 22. Zaricznyj B, Shattuck LJ, Mast TA, Robertson RV, D’Elia G. Sports-related injuries in school-aged children. Am J Sports Med. 1980;8:318–324. [DOI] [PubMed] [Google Scholar]